CRANIOFACIAL GROWTH AND DEVELOPMENT POSTNATAL Sites and Types
























 FIRST THEORY Bone is the primary determinant of its own")


 SECOND THEORY Cartilage is the primary determinant of skeletal growth, while bone responds")




 The soft tissue matrix in which")





- Slides: 41
CRANIOFACIAL GROWTH AND DEVELOPMENT : POSTNATAL
Sites and Types of Growth in the Craniofacial Complex 1. CRANIAL VAULT (the bones that cover the upper and outer surface of the brain) made up of a number of flat bones that are formed directly by intramembranous bone formation, without cartilaginous precursors
v At birth, the flat bones of the skull are widely separated by loose connective tissues. These open spaces, the fontanelles, allow a deformation of the skull at birth. This helps in allowing the large head to pass through the birth canal. v After birth, apposition of bone eliminates these open spaces, but the bones remain separated by a thin, periosteum-lined suture for many years, eventually fusing in adult life. v Mechanism of growth in cranial vault: a) apposition of new bone at sutures b) remodelling at inner and outer surfaces.
2. CRANIAL BASE: Bones of the cranial base are formed initially in cartilage and are later transformed by endochondral ossification to bone. This is particularly true of the midline structures. As one moves laterally, growth at sutures and surface remodeling become more important. As ossification proceeds, bands of cartilage called synchondroses remain between the centers of ossification These important growth sites are the synchondrosis - between the sphenoid and occipital bones: spheno-occipital synchondrosis, - intersphenoid synchondrosis, between two parts of the sphenoid bone, - spheno-ethmoidal synchondrosis, between the sphenoid and ethmoid bones.
Histologically, a synchondrosis looks like a twosided epiphyseal plate. The synchondrosis has an area of cellular hyperplasia in the center with bands of maturing cartilage cells extending in both directions, which will eventually be replaced by bone. A significant difference from the bones of the extremities is that immovable joints develop between the bones of the cranial base
3. NASOMAXILLARY COMPLEX: Nature of growth: The maxilla develops postnatally entirely by intramembranous ossification. Sites of growth: Since there is no cartilage replacement, growth occurs in two ways : (PRIMARY TRANSLATION) (1) by apposition of bone at the sutures that connect the maxilla to the cranium and cranial base, ( the space that opens up at the sutures is filled in by proliferation of bone at these locations (2) by surface remodeling In addition, the maxilla is moved forward by growth of the cranial base behind it. (SECONDARY TRANSLATION)
The growth pattern of the face requires that it grow "out from under the cranium, “which means downward and forward” Accomplished in two ways: (1) By a push from behind created by cranial base growth(secondary translation) (2) By growth at the sutures and/or remodelling (primary translation).
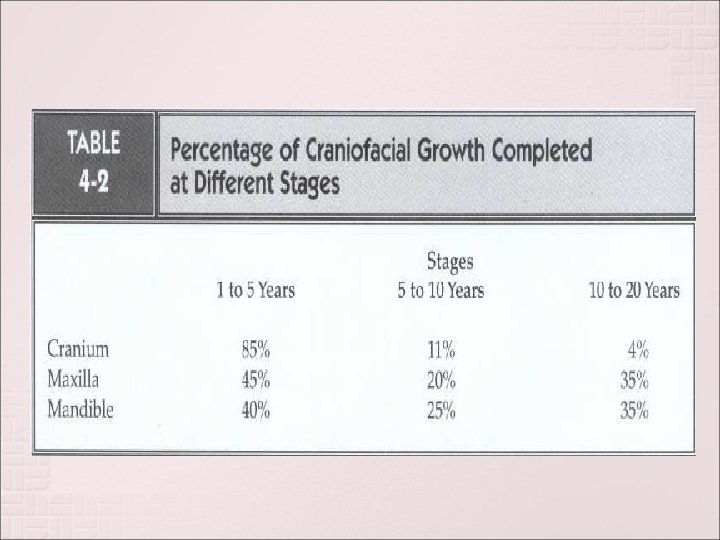
TIMING : Up until about age 6, displacement from cranial base growth is an important part of the maxilla's forward growth. At about age 7, cranial base growth stops, and sutural growth is the only mechanism for bringing the maxilla forward. ADVANTAGES OF GROWTH PATTERN: This displacement allows for growth at the posterior aspect of the maxilla as well as at the maxillary tuberosities to accommodate for the eruption of the permanent molars.
Also allows for the enlargement of the nasal and oral pharynx to accommodate for the increased respiratory functional demands of the growing child. To allow for the increased functional demands in the nasal cavities, the nasal floor is lowered by being translated bodily downward and simultaneously undergoing surface resorption. This is accompanied by bone deposition on the oral side of the palatal shelves of the maxillary bone
Note : Bone is removed from most of the anterior surface, although the anterior surface is growing forward. Changes in Maxillary Width - Growth in width at the mid-palatal suture occurs during the first 5 years of life. - At later stages of development, increase in the width of the anterior maxilla occurs as a result of bone deposition on the outer surfaces of the maxilla and by the buccal eruption of the permanent teeth.
4. MANDIBLE : Nature of growth: In contrast to the maxilla, both endochondral and periosteal activity are important in growth of the mandible. It needs to be remembered that the original (embryonic) primary cartilage of the mandible (Meckel's cartilage) disappears early during intrauterine life with only few remnants, namely the malleus and incus ossicles in the middle ear and the sphenomandibular ligament. Therefore the condylar cartilage is solely derived from secondary cartilage.
Growth pattern of mandible: The overall pattern of growth of the mandible can be represented in two ways : - If the cranium is the reference area, the chin moves downward and forward. - On the other hand, if data from vital staining experiments are examined, it becomes apparent that the principal sites of growth of the mandible are the posterior surface of the ramus and the condylar and coronoid processes. There is little change along the anterior part of the mandible. From this frame of reference this is correct.
As a growth site, the chin is almost inactive. It is translated downward and forward, as the actual growth occurs at the mandibular condyle and along the posterior surface of the ramus. The body of the mandible grows longer by periosteal apposition of bone on its posterior surface while the ramus grows higher by endochondral replacement at the condyle accompanied by surface remodeling
It is correct to view the mandible as being translated downward and forward, while at the same time increasing in size by growing upward and backward. The body of the mandible grows longer as the ramus moves away from the chin, and this occurs by removal of bone from the anterior surface of the ramus and deposition of bone on the posterior surface. The bony chin becomes more prominent with age mostly as a result of bone resorption above the chin (rather than bone deposition on the chin) accompanied with forward mandibular growth
5. ALVEOLAR PROCESSES : The growth of the alveolar bone is completely dependent on the presence and eruption of teeth. The increase in the vertical height of the face is the result of the growth of the maxillary and mandibular alveolar processes, which is associated with the eruption of teeth. Following tooth extraction, the alveolar processes start to resorb.
6. FACIAL SOFT TISSUES : Growth of the facial soft tissues does not perfectly parallel the growth of the underlying hard tissues. Growth of the Lips: - The lips trail behind the growth of the jaws prior to adolescence. - Because lip height is relatively short during the mixed dentition years, lip separation at rest (often termed lip incompetence) is maximal during childhood and decreases during adolescence. - Undergo a growth spurt to catch up the jaws during adolescence.
Growth of the Nose : - Growth of the nasal bone is complete at about age 10. - Growth thereafter is only of the nasal cartilage and soft tissues in the adolescent spurt.
Growth trends for maxilla nad mandible The growth pattern relationship between maxilla and mandible were given by Tweed by studying sequential cephalograms. The main groups into which he categorised them are: a. TYPE A: --Maxilla nad mandible grow together, --ANB angle unchanged --If it is associated with Class 1 molar relationship and ANB not exceeding 4. 5 degrees, no treatment is indicated.
Growth trends for maxilla nad mandible b. TYPE A subdivision: -- Maxilla protrudes with ANB exceeding 4. 5 --Restriction of growth of maxilla and allowing mandible to grow is needed. ---may require extractions -- prognosis is good c. TYPE B: -- maxilla and mandible grow together downward and forward with growth of maxilla exceeding that of mandible.
Growth trends for maxilla nad mandible -- Has poor prognosis as point B will not catch up with point A -- such people are vertical growers d. TYPE B subdivision: -- ANB is large and continues to increase -- unfavorable prognosis
Growth trends for maxilla nad mandible e. TYPE C: -- Mandible grwos forward and downward more than maxilla with ANB decreasing -- favorable -- no treatment needed f. TYPE C Subdivision: -- Mandible grows at avery rapid rate than maxilla -- mand. Incisors touch lingual surface of maxillaty incisors. --this causes mand incisors to tip lingually or maxillaty incisors to tip labially
CRANIOFACIAL GROWTH THEORIES Since a major part of the need for orthodontic treatment is created by disproportionate growth of the jaws, in order to understand the etiologic processes of malocclusion and dentofacial deformity, it is necessary to learn how facial growth is influenced and controlled. Exactly what determines the growth of the jaws, however, remains unclear and continues to be the subject of intensive research
CRANIOFACIAL GROWTH THEORIES Three major theories in recent years have attempted to explain the determinants of craniofacial growth. The major difference in theories is the location at which genetic control is expressed
Growth Centers vs. Growth Sites A site of growth is merely a location at which growth occurs, whereas a center is a location at which independent (genetically controlled) growth occurs. All centers of growth also are sites, but the reverse is not true.
CRANIOFACIAL GROWTH THEORIES (1) FIRST THEORY Bone is the primary determinant of its own growth. In this theory the genetic control is expressed directly at the level of the bone, so that it is the growth centre. The sutures between the membranous bones of the cranium and jaws were considered growth centers, along with the sites of endochondral ossification in the cranial base and at the mandibular condyle were considered growth centres.
If this theory were correct, growth at the sutures should occur largely independently of the environment, and it would not be possible to change the expression of growth at the sutures very much. Though it was the dominant view until the 1960 s, it has largely been discarded.
It is clear now that sutures, and the periosteal tissues more generally, are not primary determinants of craniofacial growth. Two lines of evidence lead to this conclusion. The first is that when an area of the suture between two facial bones is transplanted to another location (to a pouch in the abdomen, for instance), the tissue does not continue to grow. This indicates a lack of innate growth potential in the sutures. Second, it can be seen that growth at sutures will respond to outside influences under a number of circumstances. SO THEY ARE NOT GROWTH CENTRES.
(1) SECOND THEORY Cartilage is the primary determinant of skeletal growth, while bone responds secondarily and passively. This theory suggests that genetic control is expressed in the cartilage, while bone responds passively to being displaced. This indirect genetic control is called epigenetic.
If cartilaginous growth were the primary influence, the cartilage at the condyle of the mandible could be considered as a pacemaker for growth of that bone, and the remodeling of the ramus and other surface changes could be viewed as secondary to the primary cartilaginous growth. One way to visualize the mandible is by imagining that it is like the diaphysis of a long bone, bent into a horseshoe with the epiphyses removed, so that there is cartilage representing "half an epiphyseal plate" at the ends.
Growth of the maxilla is more difficult but not impossible to explain on a cartilage theory basis. Although there is no cartilage in the maxilla itself, there is cartilage in the nasal septum. Proponents of the cartilage theory hypothesize that the cartilaginous nasal septum serves as a pacemaker for other aspects of maxillary growth The cartilage is located so that its growth could easily lead to a downward and forward translation of the maxilla
Transplantation experiments demonstrate that not all skeletal cartilage acts the same when transplanted. Epiphyseal plate of a long bone continue to grow in a new location or in culture, indicating innate growth potential Cartilage from the spheno-occipital synchondrosis of the cranial base also grows when transplanted, but not as well. Nasal septal cartilage was found to grow nearly as well in culture as epiphyseal plate cartilage. Mandibular condyle showed significantly less growth in culture than the other cartilages.
Experiments to test the effect of removing cartilages are also informative. In rodents, removing a segment of the cartilaginous nasal septum causes a considerable deficit in growth of the midface. It can be argued that the surgery itself and the accompanying interference with blood supply to the area, not the loss of the cartilage, cause the growth changes. There are few similar reported cases of early loss of the cartilaginous nasal septum in humans.
3. THIRD THEORY (Functional Matrix Theory of Growth) The soft tissue matrix in which the skeletal elements are embedded is the primary determinant of growth, and both bone and cartilage are secondary followers. The third theory assumes that genetic control is mediated to a large extent outside the skeletal system, and that growth of both bone and cartilage is controlled epigenetically, occurring only in response to a signal from other tissues. This point of view was put formally in the 1960 s by Moss, in his "functional matrix theory" of growth, and was reviewed and updated by him in the 1990 s
In this conceptual view, the soft tissues grow, and both bone and cartilage react. Eg : a) Pressure exerted by the growing brain separates the cranial bones at the sutures, and new bone passively fills in at these sites so that the brain case fits the brain. b) An enlarged eye or a small eye will cause a corresponding change in the size of the orbital cavity. In this instance, the eye is the functional matrix. Moss theorizes that the major determinant of growth of the maxilla and mandible is the enlargement of the nasal and oral cavities, which grow in response to functional needs (The theory does not make it clear how functional needs are transmitted to the tissues around the mouth and nose)
From the view of this theory, however, absence of normal function would have wide-ranging effects. Eg : We have already noted that in 75% to 80% of human children who suffer a condylar fracture, the resulting loss of the condyle does not impede mandibular growth. What about the 20% to 25% of children in whom a growth deficit occurs after condylar fracture? the answer is “ankylosis”
It appears that the mechanical restriction caused by scar tissue in the vicinity of the temporomandibular joint impedes translation of the mandible as the adjacent soft tissues grow, and that this is the reason for growth deficiency in some children after condylar fractures under some circumstances, bone can be induced to grow at surgically created sites by the method called distraction osteogenesis
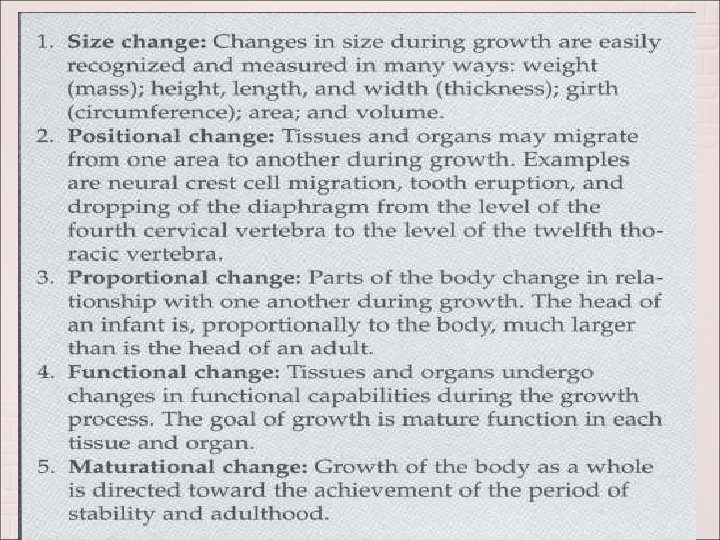
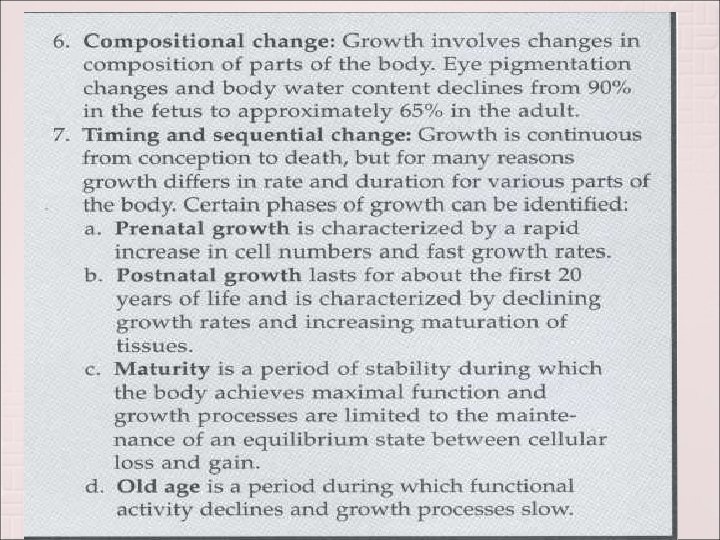
TYPES OF GROWTH CHANGES
INDICES OF MATURITY 1. 2. 3. 4. Several methods are used to assess the level of maturity attained by a child during postnatal growth MORPHOLOGIC AGE : based on height comparison in the same age group. DENTAL AGE : baesed on either tooth eruption or developmental stage of the tooth as in radiographs. SKELETAL AGE : based on development of hand-wrists as in radiographs. SEXUAL AGE : based on secondary sexual characteristics. Useful only in adolescents.