Craniocervical Arterial Dissection Spectrum of Imaging Findings Radiographics

 �spontaneous (coughing, vomiting, sports, cervical")


. �Mural hematoma and thrombus may be")





, which corresponds to")
")




 Angiography: MR angiography can also demonstrate subacute intramural")









 owing to")



 and the “string and pearl” sign (thick")
- Slides: 45
Craniocervical Arterial Dissection: Spectrum of Imaging Findings Radiographics 2008 E. Khalili Pouya
�Causal Factors: �traumatic (severe blunt head and neck trauma) �spontaneous (coughing, vomiting, sports, cervical manipulation), trigger in pts with underlying arteriopathy (FMD, Ehlers Danlos IV, Marfan syndrome, autosomal dominant polycystic kidney disease, and osteogenesis imperfecta type I
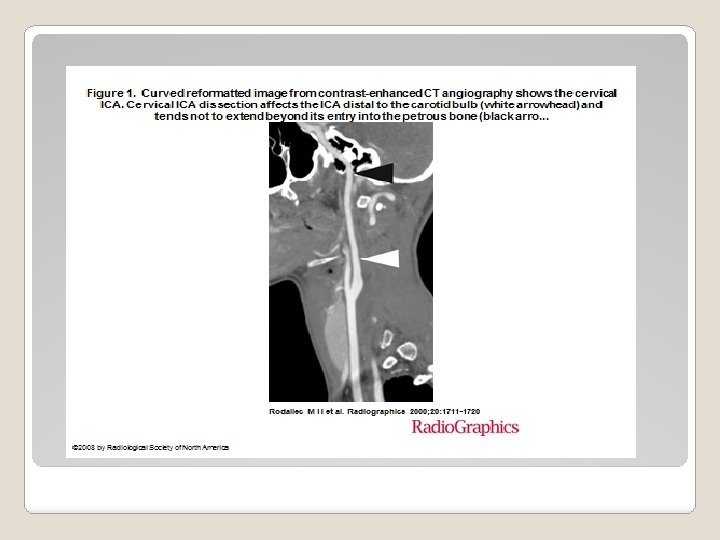
�Anatomic Distribution: �The extracranial segments of the carotid and vertebral arteries are much more likely to undergo dissection than their intracranial segments �Extracranial ICA dissection affects the cervical part of the artery distal to the carotid bulb and tends not to extend beyond its entry into the petrous portion
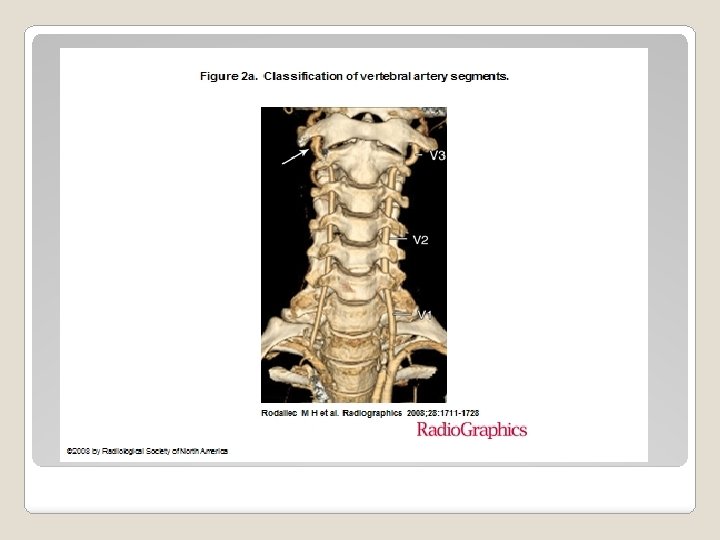
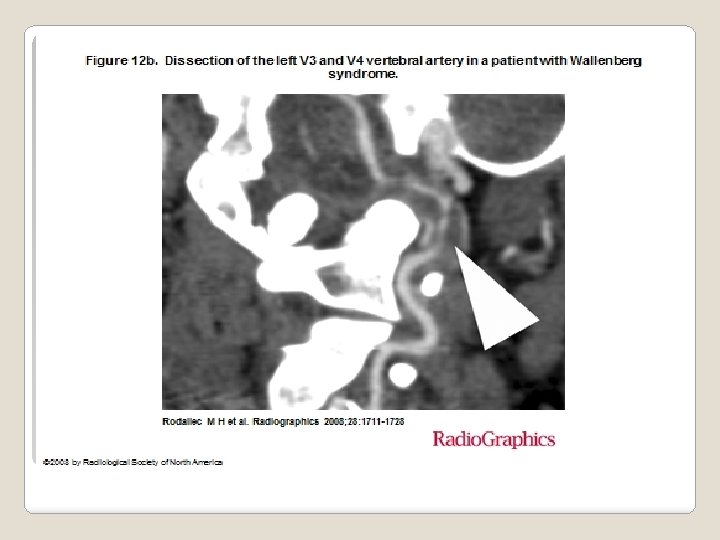
segments of the vertebral artery. V 1 = between its origin and its entry into the transverse foramen of the C 6 vertebra, V 2 = midcervical course between the processes of C 6 to C 2, V 3 = atlas loop region, V 4 = intracranial segment. Note the asymmetric venous plexus enhancement around the V 3 segment (arrow in a).
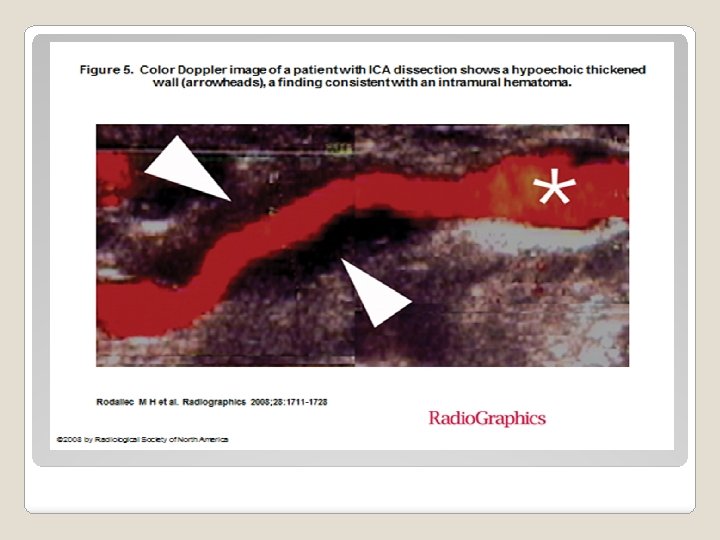
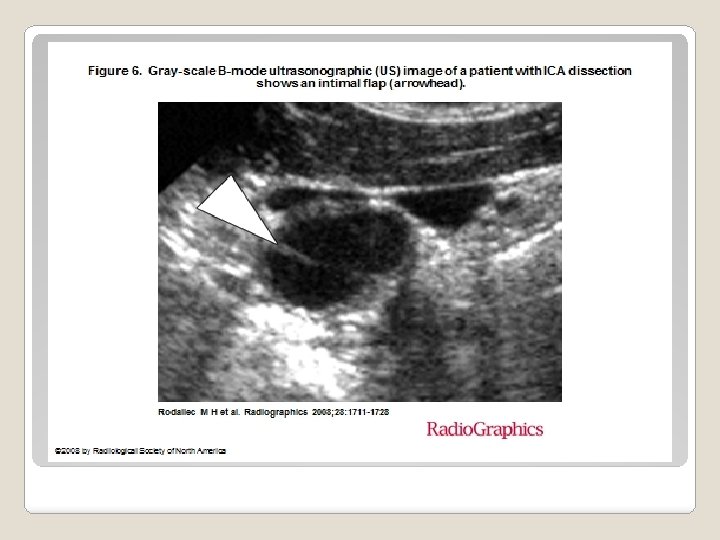
�Color Duplex US: �linear transducers (4– 8 MHz). �Mural hematoma and thrombus may be detected as a thickened hypoechoic vessel wall �Usually, wall hematoma and intraluminal thrombus cannot be differentiated with Bmode imaging �inner intimal echo helps in distinguishing wall hematoma from intraluminal thrombus or plaque in patients with thickening of the ICA wall
�CT Angiography: Unenhanced brain CT is helpful to document associated ischemic and hemorrhagic events scanning range from the aortic arch to the circle of Willis section thickness of 0. 625 mm pitch of 0. 9 80 m. L of nonionic contrast medium (iodine, 350 mg/m. L) followed by a saline bolus at a rate of 3. 5 m. L/sec.
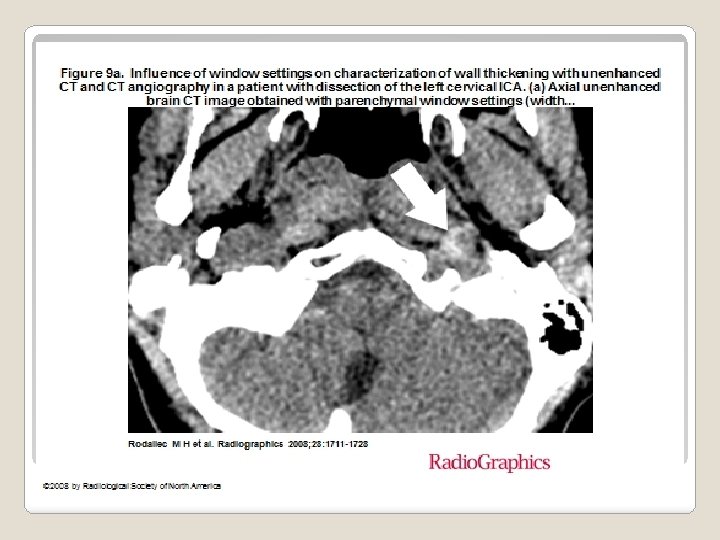
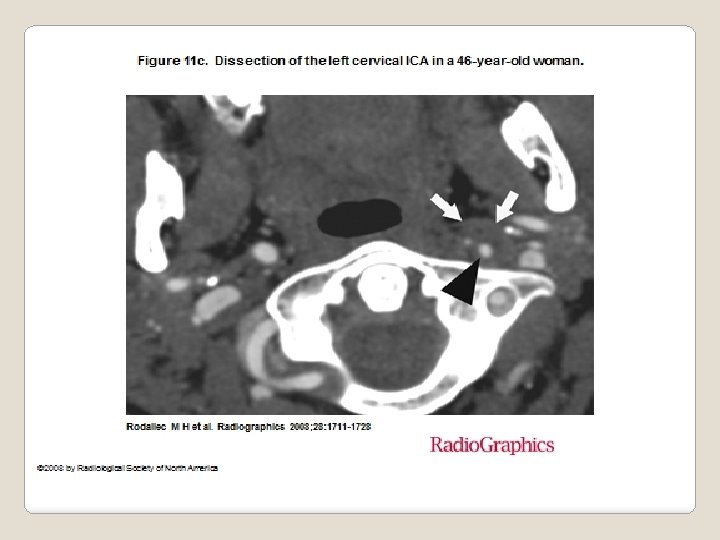
ICA dissection is characterized by a narrow eccentric lumen with increase of the external diameter of the artery �At unenhanced brain CT, a spontaneous crescent-shaped hyperattenuating area corresponding to a wall hematoma may be noticed in acute dissection at the upper portion of the cervical ICA. However, when correct window settings are applied for CT angiography, intramural hematoma appears isoattenuating to the surrounding muscles and cannot be differentiated from atherosclerotic thickening or thrombus Thus, familiarity with common dissection sites is essential to diagnose ICA dissection with CT angiography. �
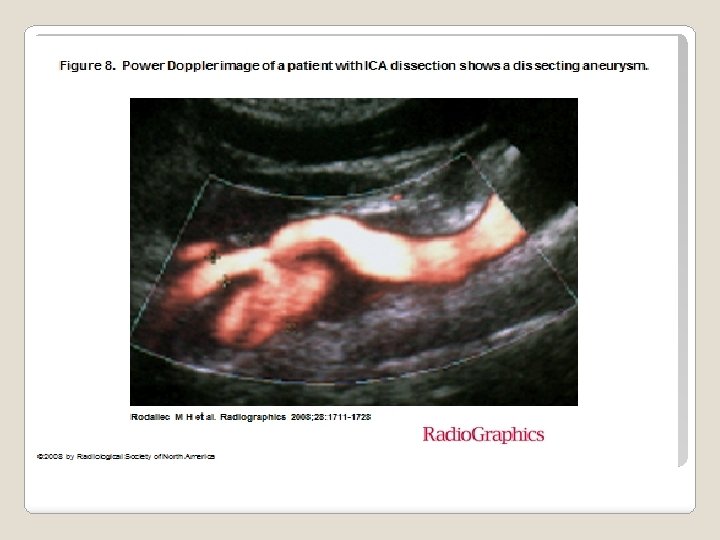
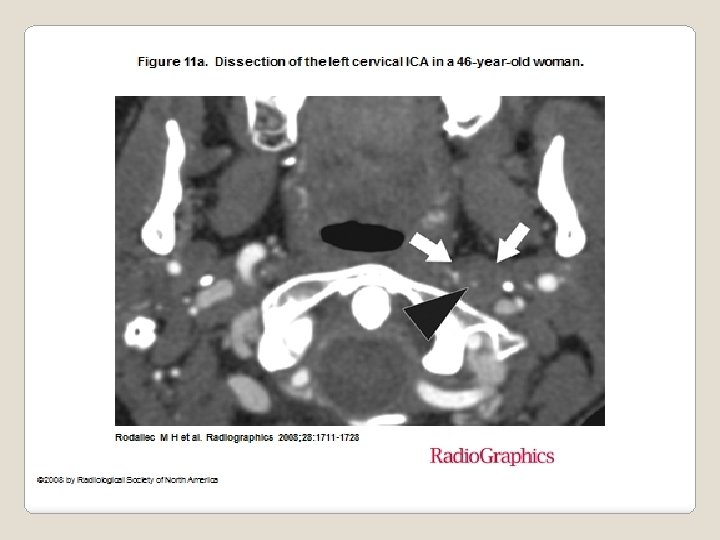
�The typical target picture (narrow eccentric lumen surrounded by crescentshaped mural thickening and thin annular enhancement) is a very specific yet less sensitive sign of arterial dissection �Peripheral enhancement is probably due to the contrast enhancement of the vasa vasorum in the adventitial layer �Other fairly reliable signs of arterial dissection are an intimal flap, a dissecting aneurysm
Axial image from CT angiography obtained with the same window settings does not show any parietal abnormality.
On an axial image from CT angiography obtained with wide window settings (width = 500 HU, level = 100 HU), the intramural wall hematoma (arrow) is isoattenuating relative to the surrounding muscles and cannot be differentiated from atherosclerotic thickening.
Axial unenhanced brain CT image shows a crescentshaped hyperattenuating area (arrow), which corresponds to an intramural hematoma in the right ICA.
Axial image from CT angiography shows the residual lumen (arrowhead)
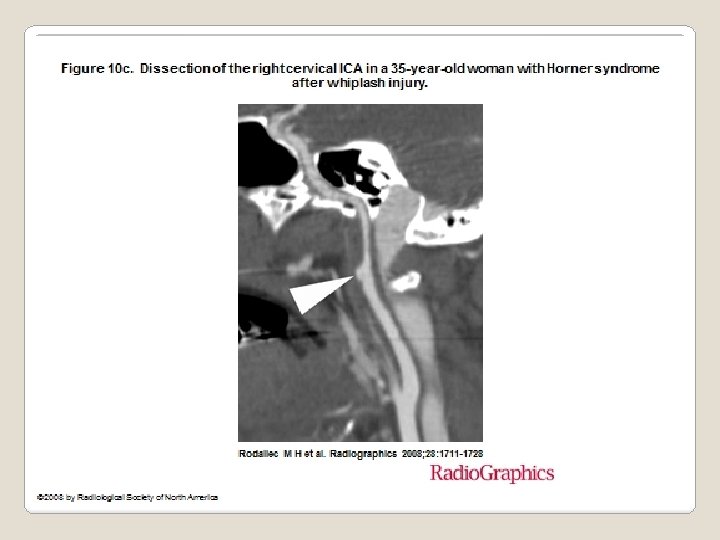
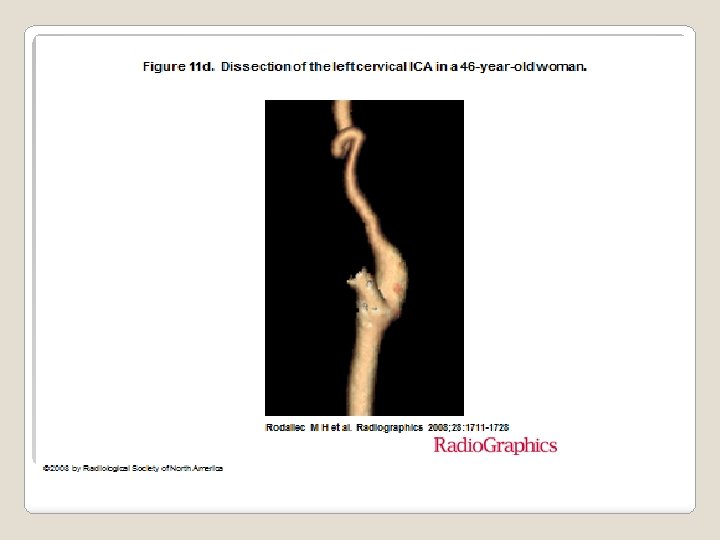
Volume-rendered image from CT angiography shows a long tapered stenosis that begins distal to the carotid bulb (the string sign)
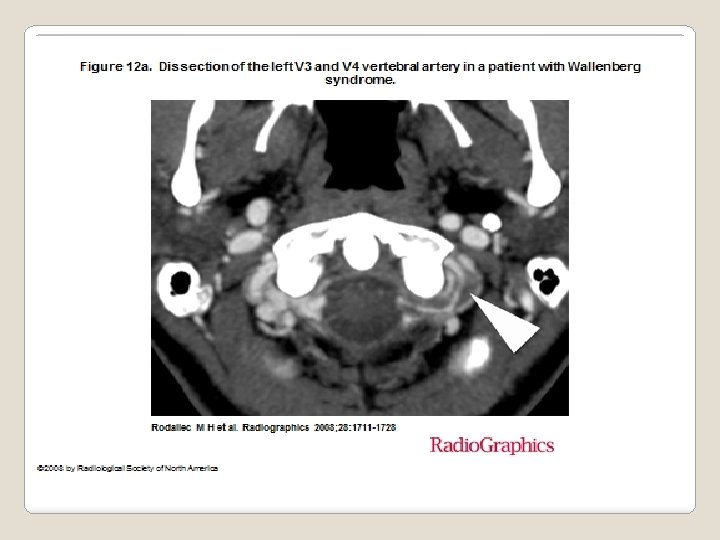
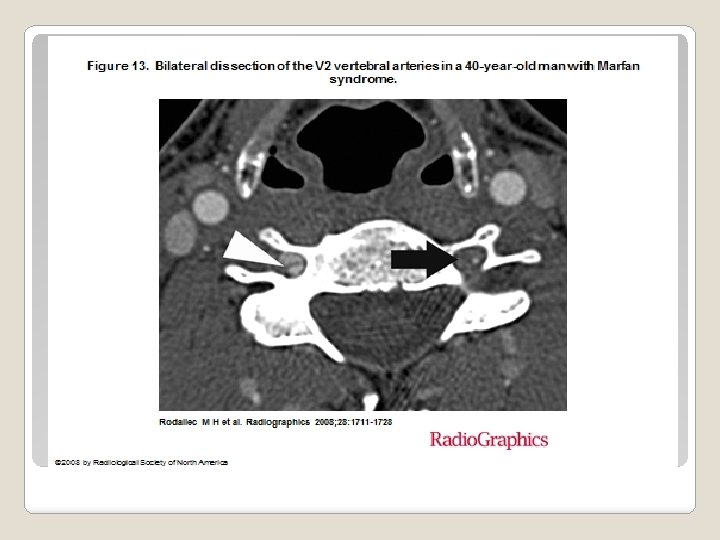
�Vertebral Artery Dissection: �Increased external diameter and crescentshaped mural thickening � both signs can be found in nondissected vertebral arteries � typical target sign was also demonstrated � intimal flap is less frequent than an intramural hematoma
Axial image shows intracranial extension of the dissection with crescent-shaped parietal thickening of the left V 4 vertebral artery (arrow).
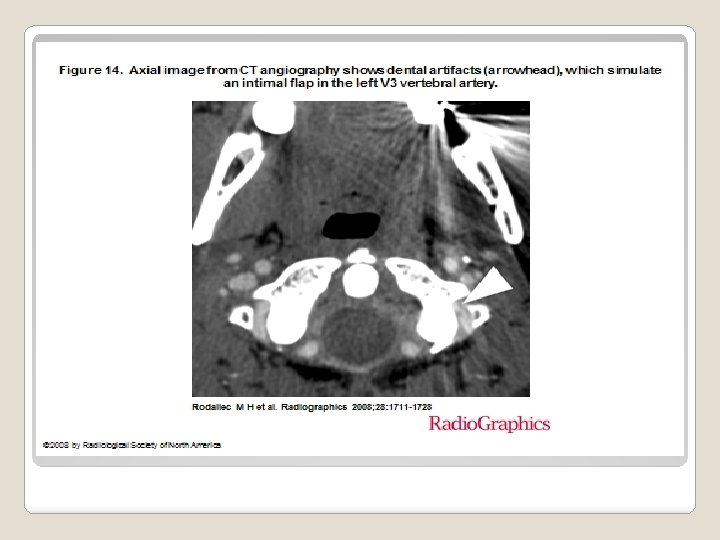
�Potential Pitfalls: � source images and reformatted 2 D and 3 D images from CT angiography can be affected by bone artifacts at the skull base and by dental artifacts
�MR Imaging and MR �Time-of-flight (TOF) Angiography: MR angiography can also demonstrate subacute intramural hematoma �phase-contrast MR angiography and contrast-enhanced MR angiography demonstrate only the vessel lumen � TOF MR angiography and contrastenhanced MR angiography are commonly used to evaluate the intracranial and extracranial vessels, whereas experience with phase-contrast MR angiography is limited in carotid and vertebral artery dissection.
�The hematoma shows a typical evolution of signal intensity related to the paramagnetic effects of the products of hemoglobin breakdown. In the early and chronic stage, the hematoma is usually isointense to surrounding structures, whereas between 7 days and 2 months it is almost invariably bright on T 1 -weighted images. Acute dissection can hardly be detected on T 1 -weighted images with fat saturation because isointense hematoma may be obscured when surrounded by isointense tissues.
�The hematoma usually becomes isointense within 6 months or disappears �Subacute hematoma is more clearly visualized on T 1 -weighted images with fat saturation and appears characteristically as a crescent-shaped hyperintense area around an eccentric flow void corresponding to the vessel lumen
Axial T 1 -weighted MR image shows isointense wall thickening of the right ICA (arrowheads), a finding consistent with an acute intramural hematoma (oxyhemoglobin or deoxyhemoglobin phase
fat-saturated T 1 -weighted MR image obtained in another patient shows slightly hyperintense wall thickening of the left ICA (arrowheads), a finding consistent with an early subacute intramural hematoma (methemoglob in phase).
Axial T 1 weighted MR images obtained with fat saturation (a obtained at a higher level than b) show a narrowed eccentric flow void (arrowhead) surrounded by a crescentshaped circumferential subacute intramural hematoma that expands the vessel diameter. The hematoma spirals around the vessel . lumen
�The criteria used for dissection are: �increase in the external diameter of the artery and narrowing of the lumen. �flow void narrowing is a less useful indicator of dissection because it can be encountered in other conditions. �“train track” sign, a sign of poststenotic laminar flow in the petrosal horizontal portion of the ICA, can be mistaken for intrapetrous extension of ICA dissection. �Increase in the external diameter of the artery may be present in cases of dissecting aneurysm
�MR imaging is not as helpful in diagnosis of vertebral artery dissection � Dissection at V 2 may be difficult to identify because inflow enhancement in the venous plexus of the foramen transversarium may mimic subacute hematoma �Another problem with diagnosis of vertebral artery dissection is the common exclusion of V 1 from the imaged volume �MR imaging demonstrated excellent sensitivity in diagnosis of internal carotid dissection
Axial T 1 weighted MR image obtained with fat saturation shows hyperintense crescent-shaped mural thickening, a finding consistent with a subacute intramural hematoma. Note the intermediate signal intensity of the venous plexus around the left vertebral artery and in the anterior epidural space.
Threedimensiona l TOF MR image shows pseudoenla rgement of the lumen due to a subacute intramural hematoma (arrowhea d).
Axial diffusionweighted MR image demonstrate s the hyperintense subacute intramural hematoma (arrowhead) owing to the T 2 “shinethrough” effect.
contrast-enhanced MR angiography of the cervical vasculature occasionally results in segmental blurring or signal intensity loss within the vertebral arteries, especially in young patients with rapid circulation times �This “feathering” artifact results from rapidly changing signal intensity in small vascular structures around the vertebral arteries �This pseudostenosis artifact may mimic vertebral artery dissection �
�Our protocol for craniocervical arterial dissections : �cross-sectional T 1 -weighted + fat saturation of the neck �contrast-enhanced MR angiography. �Additional axial T 1 - and T 2 -weighted images may be required in cases of acute dissections. �nonenhanced MR angiography when gadolinium-containing contrast agents are contraindicated.
�Digital Subtraction Angiography: � string sign, the angiographic hallmark of ICA dissection, is a long, tapered, usually eccentric and irregular stenosis that begins distal to the carotid bulb � Focal narrowing with a distal site of dilatation is referred to as the “string and pearl” sign �Pathognomonic signs, such as a double lumen or intimal flap, are rarely observed �“flame” sign, a tapered occlusion that spares the carotid bulb, is highly suggestive of dissection
Angiogram shows the string sign (thin arrow) and the “string and pearl” sign (thick arrow), findings consistent with bilateral ICA dissections. Note the “string of beads” sign (arrowhead), which is consistent with fibromuscular dysplasia of the left vertebral artery.