Cracking of a Surgical Aortic Valve Isaac George















 P<0. 001 80 42 ± 11 P<0.")
 Avalus")





")











- Slides: 36
Cracking of a Surgical Aortic Valve Isaac George, M. D. Surgical Director Structural Heart and Valve Center New York Presbyterian Hospital-Columbia University Medical Center
Disclosure Statement of Financial Interest Isaac George, MD Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Company Affiliation/Financial Relationship • Consultant • • Mitre. Medical Cardio. Mech Vdyne Atricure
Patient Prosthesis Mismatch Lives Matter
How do we prevent Surgical PPM in VIV? For young patients, should we be doing more root enlargements at the initial operation? • Place larger valves • Facilitate TAVR VIV in the future
Bioprosthetic Valve Fracture: A New Method to Treat Surgical PPM Nielsen-Kudsk JE, et al. Circ Cardiovasc Intv 2015
WTF? That sounds crazy! • Potential Benefits 1. Allow for larger TAVR VIV 2. Allow for overexpansion of TAVR VIV 3. Reduce PPM, optimize hemodynamics 4. Higher EOA, lower MG
Bioprosthetic Valve Fracture
Bioprosthetic Valve Fracture
Bioprosthetic Valve Fracture
Bioprosthetic Valve Fracture • Valve explanted due to persistent symptoms • Patient clinically improved after redo MVR • Explanted valve demonstrates issue of “covered stent”
Bioprosthetic Valve Fracture: A New Method to Treat Surgical PPM
Bioprosthetic Valve Fracture: Clinical Experience • 20 consecutive patients* from 7 US centers treated with bioprosthetic valve fracture at the time of Vi. V TAVR (8 at MAHI) • Mean age 76 years; mean STS-PROM 8. 4% • Valves treated: Mitroflow, Perimount, Magna/Magna-Ease, Biocor Epic/Epic-Supra, and Mosaic • Treated with both self-expanding (n=12) and balloon expandable (n=8) TAVR valves • 15/20 underwent BVF after TAVR valve deployed
• 75 pts • Sapien 57%, Evolute 43%
Timing • Prior to TAVR – – • No damage to TAVR leaflets ? greater opening of valve frame Severe AI pre TAVR, hemodynamic instability Embolic risk Post-TAVR – – Risk of TAVR leaflet injury TAVR in place may be protective No hemodynamic instability Much less embolic risk
Balloon Placement: Low or High? • If doing BVF after TAVR placed, may sure shoulder is below TAVR constrained area or can damage leaflets
Mean Gradient 100 Mean Gradient (mm. Hg) P<0. 001 80 42 ± 11 P<0. 001 60 21 ± 7 40 7± 4 20 0 Baseline Post-TAVR Post-BVF
To date, the only valves that cannot be fractured are: Hancock II (MDT) Avalus (MDT)
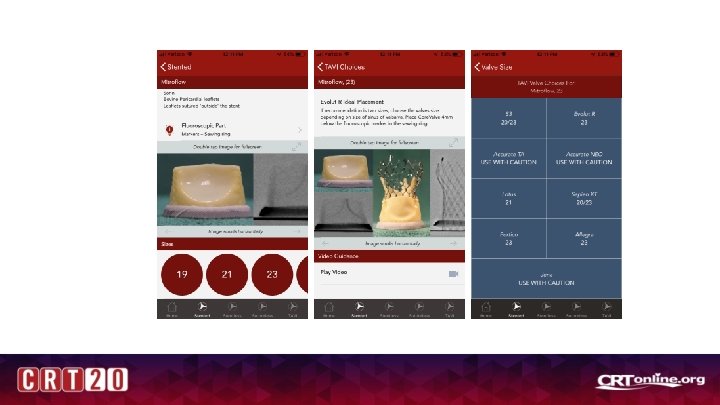
BVF: what size balloon? • • • The pressure is applied from within What is fractured: Stent frame at inflow Balloon size – 1 mm more than label size , or – 2 mm more than STENT ID Valve type Label size Stent ID True Balloon Stent ID+2 according to label size+1 Mitroflow 23 19 21/22 24 Perimount 23 22 24 24 Mosaic 23 21 23/24 24 Epic Supra 23 23 25/26 24
Mitroflow 23 Stent ID 19 True Balloon Size: 22 mm
Bioprosthetic Valve Fracture Complications • Annular rupture • Balloon rupture (we have had 2, 1 CVA) • If BVF prior to valve, severe AI • CVA from debris • Valve embolization • Leaflet damage • Higher pacemaker? • Mitral valve damage
BVF is not high risk but its not zero risk. So who should get BVF? 1. Small valves (#19, #21, #23) in order to improve hemodynamics. 2. Valves that will allow upsizing of TAVR VIV 1. #23 (21 ID) BVF 23 ID so #26 S 3 or #29 Evolute 2. #27 (25 ID) BVF 27 ID so #29 S 3 or #31/34 Evolute 3. It may not make sense from risk-benefit profile to BVF a #25, as it won’t change the implanted TAVR VIV (remains a #26 S 3 or #29 Evolute). 4. It is debatable if you should BVF a #27 or #29 valve – the VIV hemodynamics are very good to begin with.
VFit technology‡ incorporates two novel features designed for potential future valve-in -valve (Vi. V) procedures VFit technology Fluoroscopically visible size markers Expansion zone ‡ Refer to device instructions for use for important warnings related to VFit technology. These features have not been observed in clinical studies to establish the safety and effectiveness of the model 11500 A for use in Vi. V procedures. VFit technology is available on sizes 19 -25 mm.
Case 1: Too Much of a Good Thing • 72 yo M • #23 Magna in 2005 • Presented for VIV • BVF with #24 Tru
Persistent Mod PVL: Annular Damage?
Valve-in-valve TAVR with valve fracture 23 mm Evolut Pro aortic bioprosthesis within a Magna 19 mm surgical valve
Valve positioning
Valve deployment MG 18
Post-dilatation with a 20 mm x 40 mm True Balloon, MG 8
Fractured valve
TF-TAVR VIV without BVF Sapien 3 #26 in #25 Perimount 2700
CT analysis
Deployment, MG 6 • Dont always need to do BVF • Top of stent frame bows out for Perimount – that is where you get hemodynamic advantage
Thank you!