CPR By Dr Zaki Bettamer MD zikoechoyahoo com

CPR By Dr. Zaki Bettamer, MD zikoecho@yahoo. com 29/12/2016

CARDIAC ARREST Sudden & complete loss of cardiac function

Causes of cardio respiratory arrest 1 - Airway obstruction: CNS depression, blood, vomitus, FB, epiglottises , oedema, laryngospasm and secretions 2 - breathing problems: A-Respiratory drive -CNS depression B-Respiratory effort - muscle weakness , nerve damage and # ribs C-Lung disorders -infection, aspiration, COPD, asthma, PE, ARDS, pulmonary oedema, pneumothorax……ect 3 -Circulatory problems: primary or secondary heart diseases (IHD, HHD, valve diseases, drugs, electrolyte disorders, acidosis, hypothermia, electrocution ……. etc

Causes of SCD Most common cause of SCD in adult population is CAD 90 -95% VF/PLVT in 75 -80% of cases A systole <20% of cases Non CAD SCD 5 -10%

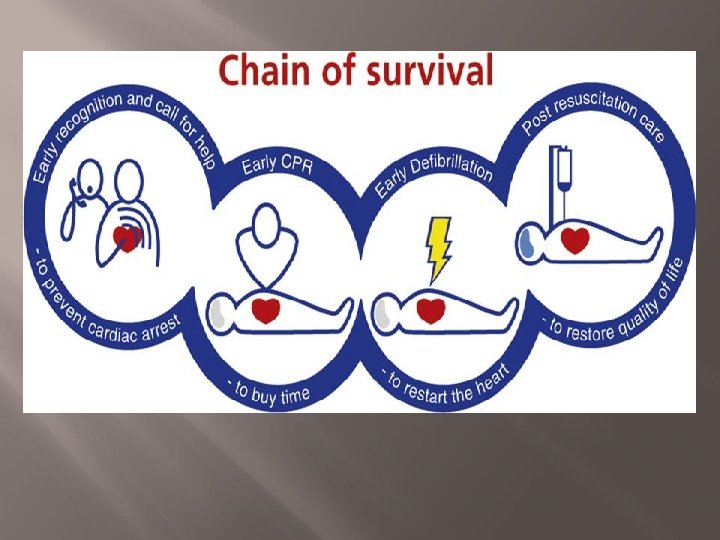
THE VICTIM OF CA IS MOST LIKELY TO SURVIVE IF THE FOLLOWING STEPS ARE APPLIED
 – to buy")
Ø Ø Early recognition and call for help Early CPR (BLS) – to buy time Early defibrillation (ALS) – to restart the heart Post resuscitation care – to restore quality of life
 It consists of those elements of resuscitation that can be")
Basic Life Support (BLS) It consists of those elements of resuscitation that can be performed without additional equipment Advanced Life support (ALS) Monitoring Defibrillation Advanced airway management Drugs

Basic life support The aim of BLS is to maintain the circulation until more definitive treatment with ALS can be administered

Collapsed/sick patient Ensure personal safety Shout for help & check patient for a response If no response Signs of life EMT yes If respond Assess ABCD+oxygen+ Monitoring +IV access no CPR 30: 2 ALS EMT or RT

Collapsed / sick patient Ensure personal Safety

Ensure personal safety Patient's surroundings & protection (gloves, eye protection, mask, risk of infection, poisons, chemicals, electricity … )

Collapsed /sick patient Ensure personal safety Shout for help & check patient for a response


 Gently shake the")
Call resuscitation team or EMT ( easy Telephone No like 111) Gently shake the patient and ask loudly How are you. Are you all right ?

Collapsed /sick patient Ensure personal safety Shout for help & check patient for a response If respond Positioning+ ABCD approach+ Oxygen +monitoring +IV access


Collapsed /sick patient Ensure personal safety Shout for help & check patient for a response If respond Positioning+ ABCD approach+ Oxygen +monitoring +IV access

ABCDE approach in critically ill patients A B C D E AIRWAY BREATHING CIRCULATION DISABILITY EXPOSTURE

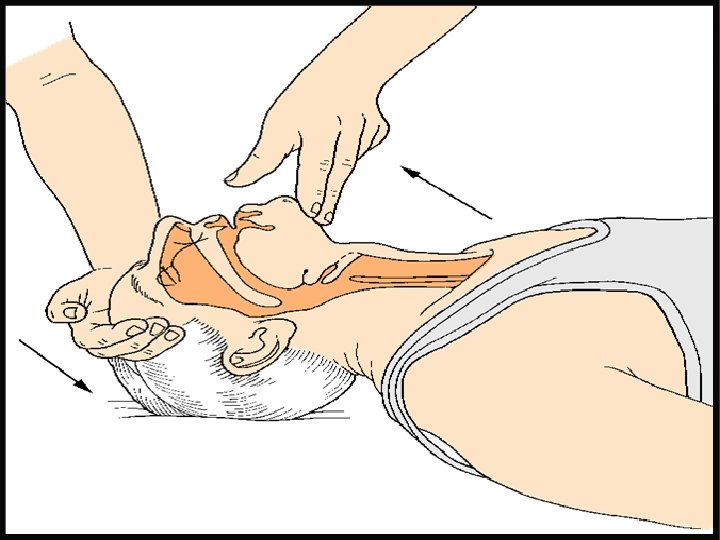
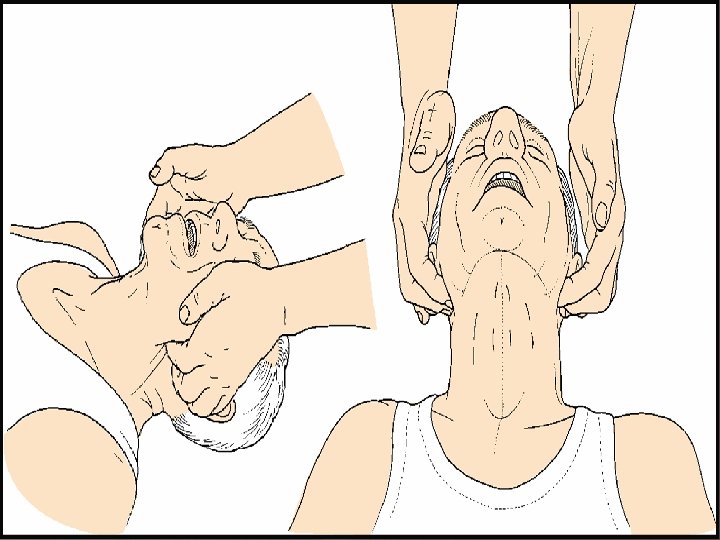
AIRWAY Ø Ø Look for signs of airway obstruction (paradoxical chest/abdomen movement, no breath sounds, noisy breathing…) Cyanosis is late sign In most cases: airway opening maneuvers , airway suction, oropharyngeal airway and ETT (ALS) High oxygen concentration

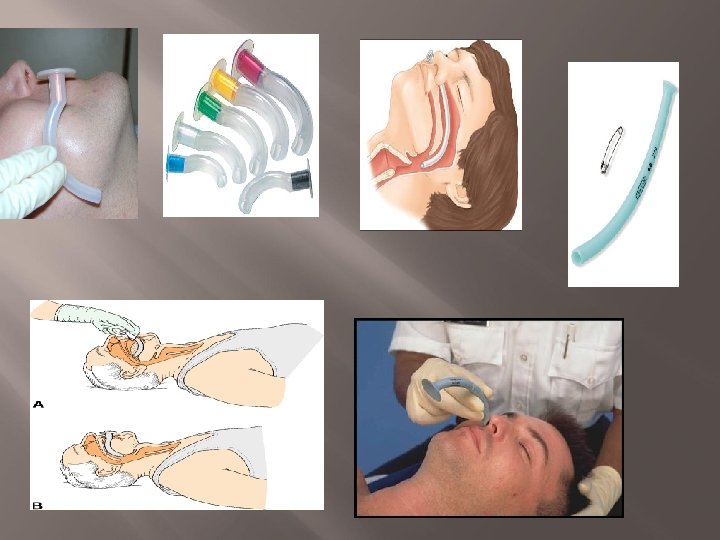

Advanced Airways Endotracheal Tube Laryngeal Mask Airway LMA
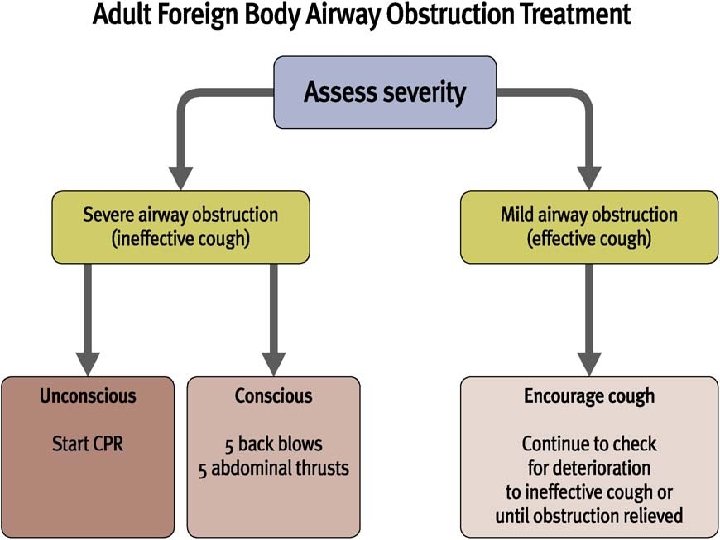

ABDOMINAL THRUSTS

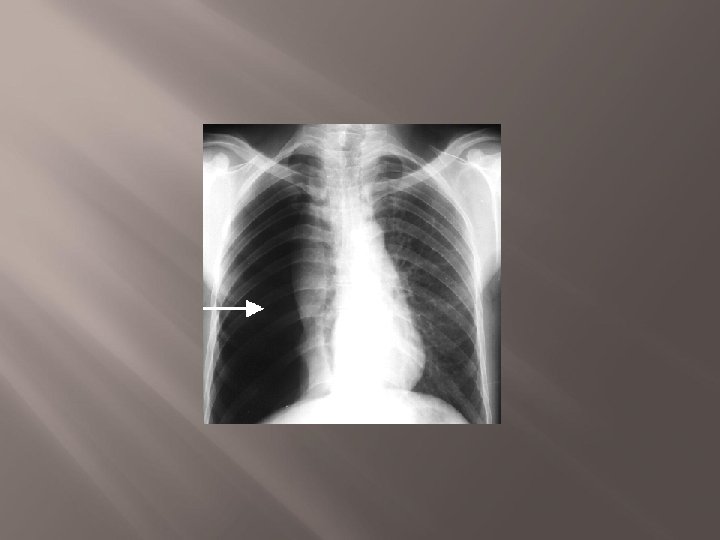
BREATHING Ø Ø Ø Signs of respiratory distress ( sweating , central cyanosis, access muscles, …. ) Count the RR and assess the depth and pattern of breathing R/O pneumothorax Pulse oxymeter Bag mask or pocket mask ventilation


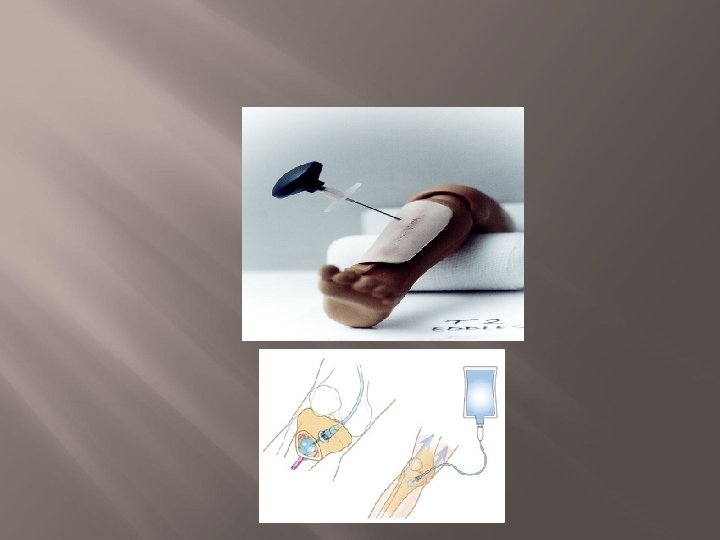
CIRCULATION Color & temperature of the hand & digits Ø CRT……<2 sec Ø BP, pulse and monitor (ALS) Ø I/V access Ø 12 lead ECG Ø

DISABILITY &EXPOSTURE Ø Ø Ø Review & treat ABCs Exclude hypoxia Drugs- antagonists, dextrose…. Pupils Assess conscious level (AVPU or GCS) Exposure & examination

Collapsed /sick patient Ensure personal safety Shout for help & check patient for a response If no response If respond EMT Open airway ABCD approach+ Oxygen+monitoring+IV access RT or EMT

Collapsed /sick patient Ensure personal safety Shout for help & check patient for a response If no response If respond EMT Open airway Signs of life ABCD approach+ Oxygen+monitoring+IV access RT or EMT
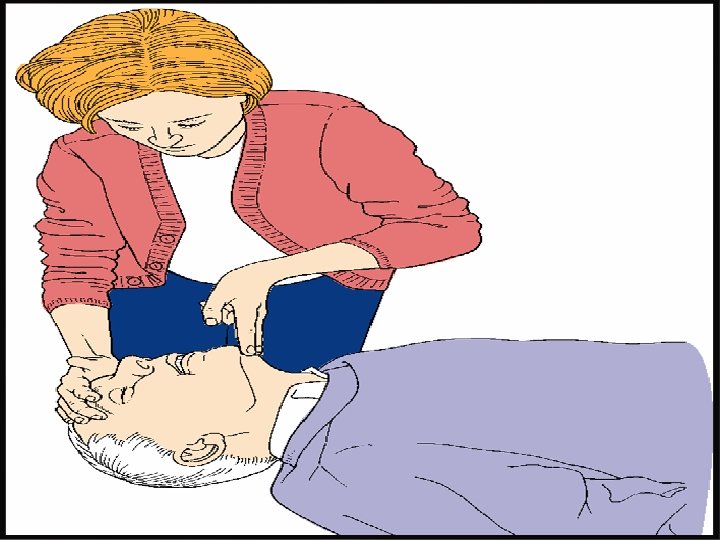
 Look – chest movement (breathing or coughing )")
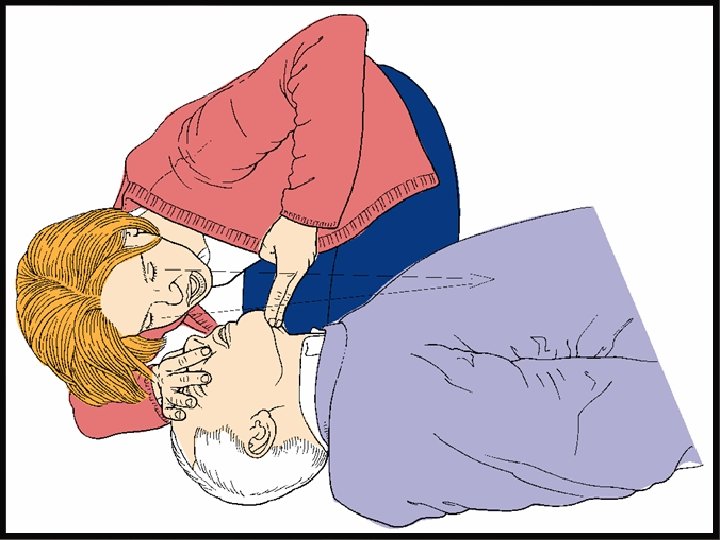
Signs of life (simultaneous &<10 sec) Look – chest movement (breathing or coughing ) Listen— at the victim's mouth for breath sound Feel – for air on your cheek - carotid pulse

Collapsed /sick patient Ensure personal safety Shout for help & check patient for a response If no response If respond EMT Open airway Signs of life No CPR 30: 2 ABCD approach+ Oxygen+monitoring+IV access yes ALS RT or EMT

30 2
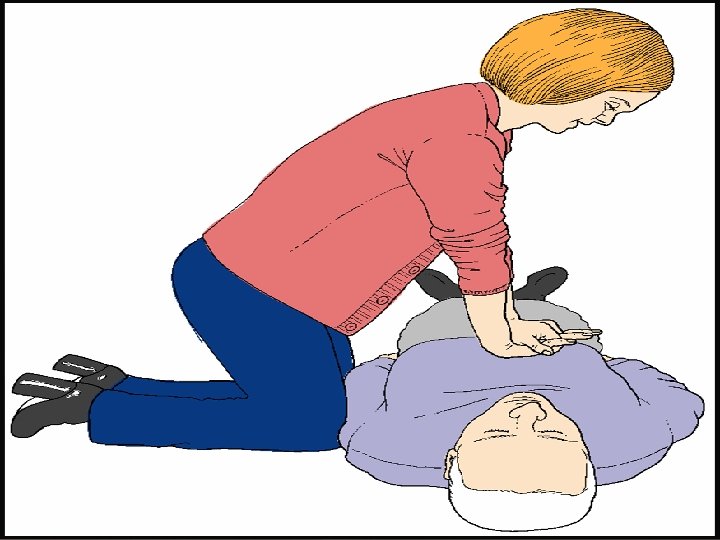
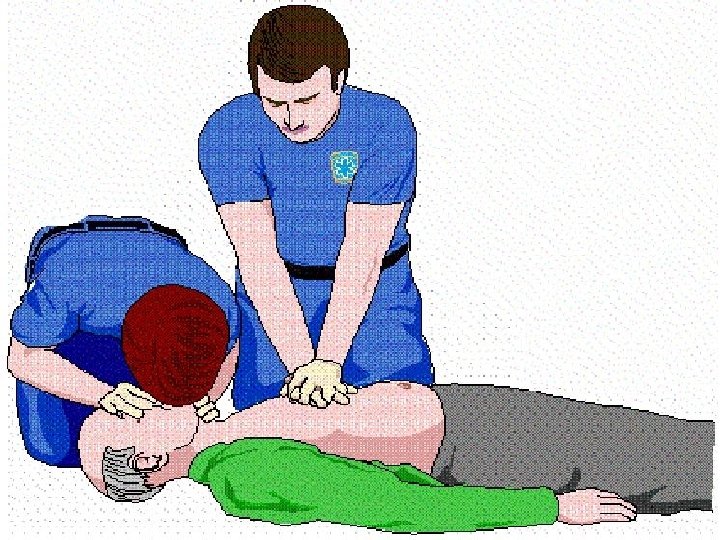
 Ø Ø Ø Ø Uninterrupted chest compressions Give 30 compressions")
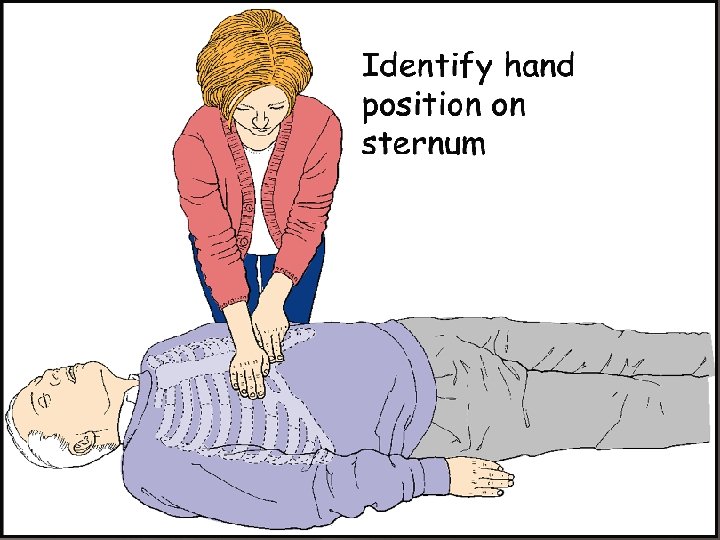
During CPR (chest compression) Ø Ø Ø Ø Uninterrupted chest compressions Give 30 compressions to 2 breaths The priority for compressions Ideally compress chest by 4 -5 cm At rate of 100/min Pause every 2 min <10 sec (ALS) Pause for intubation < 30 sec (ALS) Don't wait after giving DC shock for the electrical cardiac response (ALS)

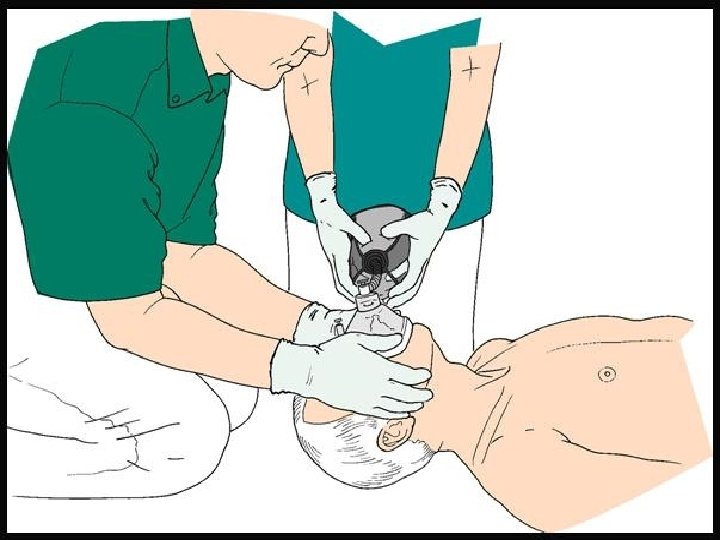
Ventilation Mouth to mouth or mouth to nose breathing Use equipment available (bag mask, pocket mask…. ) Two ventilations after 30 chest compressions Remember …the blood oxygen content after VF can maintain life for about 4 – 6 min After securing airways give uninterrupted ventilations at a rate of 10 per min (ALS)

Collapsed/sick patient Shout for help and assess patient no Call resuscitation team CPR 30: 2 With oxygen & airway adjuncts Signs of life yes Assess ABCDE Recognize & treat Oxygen, monitoring & I/V access Call resuscitation team If appropriate Monitor/defib if needed Handover to resuscitation team ALS
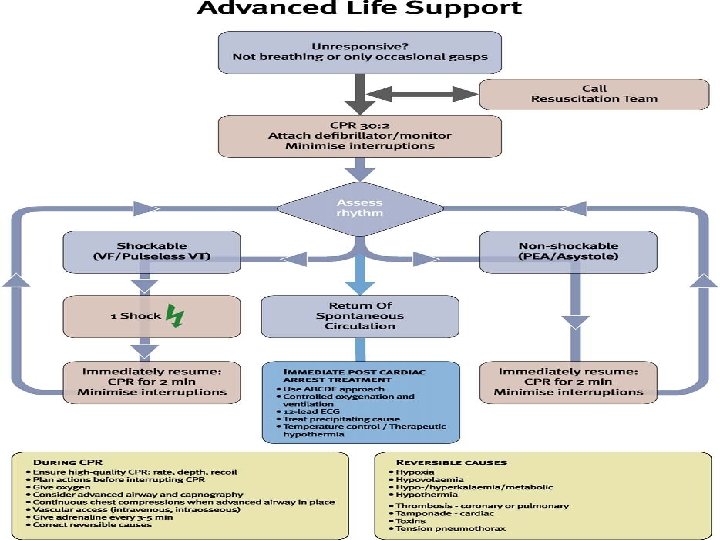

Cardio respiratory arrest CPR , check for ROSC every 2 min & Adrenaline 1 mg every alternate loop Defibrillator /monitor Shockable rhythm
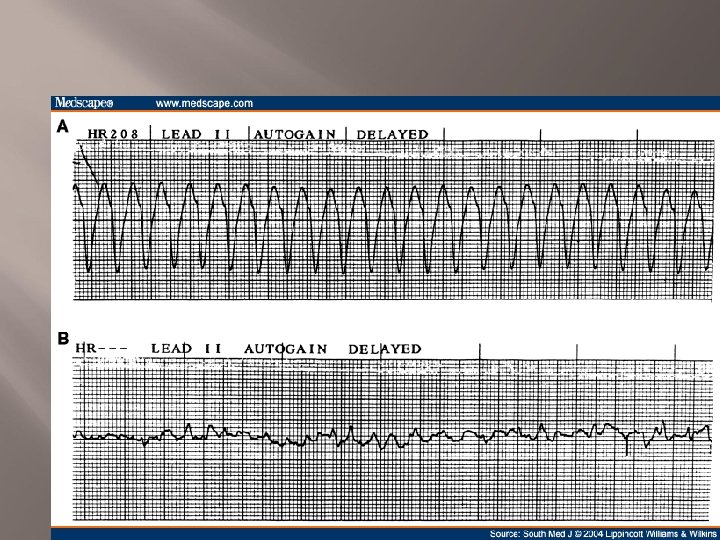


Cardio respiratory arrest CPR , check for ROSC every 2 min & Adrenaline 1 mg every alternate loop Defibrillator /monitor Shockable rhythm 1 st DC shock+CPR for 2 min 2 nd DC shock +CPR for 2 min 3 rd DC shock +Adrenaline +Amiodaron 300 mg+ CPR 2 min DC shock+CPR every 2 min DC shock +adrenaline in alternate loop +CPR 2 min

Cardio pulmonary arrest CPR +check ROSC every 2 min+ Adrenaline 1 mg every alternate loop Monitor Non Shockable rhythm

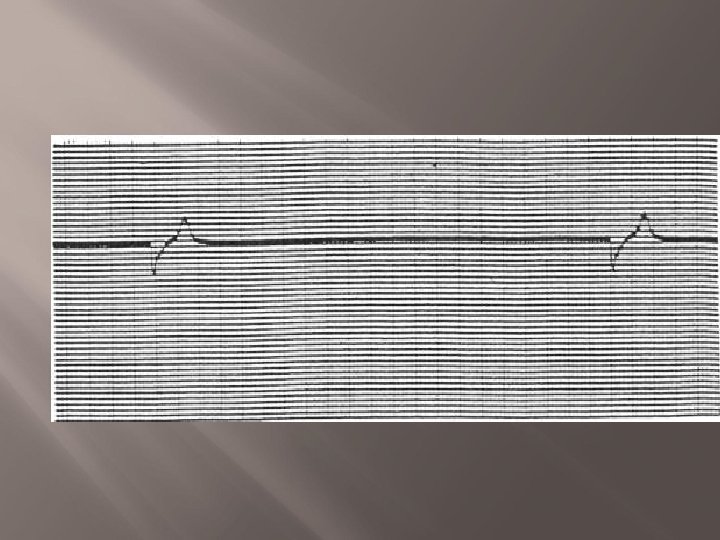

Cardio pulmonary arrest CPR +check ROSC every 2 min+ Adrenaline 1 mg every alternate loop Monitor Non Shockable rhythm CPR +check rhythm every 2 min +adrenaline 1 mg every alternate loop
 4 Hs Hypoxia Hypothermia Hypo/hyperkalemia& electrolyt Hypovolemia 4 Ts Tension")
During CPR (reversible causes) 4 Hs Hypoxia Hypothermia Hypo/hyperkalemia& electrolyt Hypovolemia 4 Ts Tension pneumothorax Tamponade Toxins Thrombosis (coronary/pulmonary)

Thank you
- Slides: 61