CPC Prep Class Lamon Willis CPCO CPCI COC








 •")



 • Superficial, epidermis or dermis • Intermediate (12031 -12057)")



 • Also known as Z-plasty, W-plasty, Rotation")




 • Split Thickness or Full Thickness •")
 • With an Allograft")
























 • The structural balloon was placed in the preperitoneal space and")



 is scheduled for a circumcision. He")













; 1")





 • Not reported when")






































- Slides: 115
CPC Prep Class Lamon Willis, CPCO, CPC-I, COC, CPC AHIMA-Approved ICD-10 -CM/PCS Trainer
Disclaimers • CPT® codes are the registered trademarked nomenclature of the American Medical Association (AMA) and are licensed and purchased for use in payment schema, including software systems through that organization. • ICD-CM codes are licensed for use by the World Health Organization (WHO), and ICD-PCS codes are developed and offered for use by the Centers for Medicare and Medicaid Services (CMS) within the United States of America.
TOP MISSED CODING CONCEPTS
Lesion Excisions • Things to look for in documentation: • How is the lesion excised? • What type of lesion is it? • How large is the excised diameter? • What is the depth of the excision? • How is the defect closed? • Can the closure be coded in addition to the excision? • Are there multiple lesions?
Shave Lesions • The sharp removal of an epidermal or dermal lesion that does not require suturing • 11300 -11303 • Per lesion located on the trunk, arms or legs • 11305 -11308 • Per lesion located on the scalp, neck, hands, feet, genitalia • 11310 -11313 • Per lesion located on the face, ears, eyelids, nose, lips, mucous membrane • Note the size in your code selection
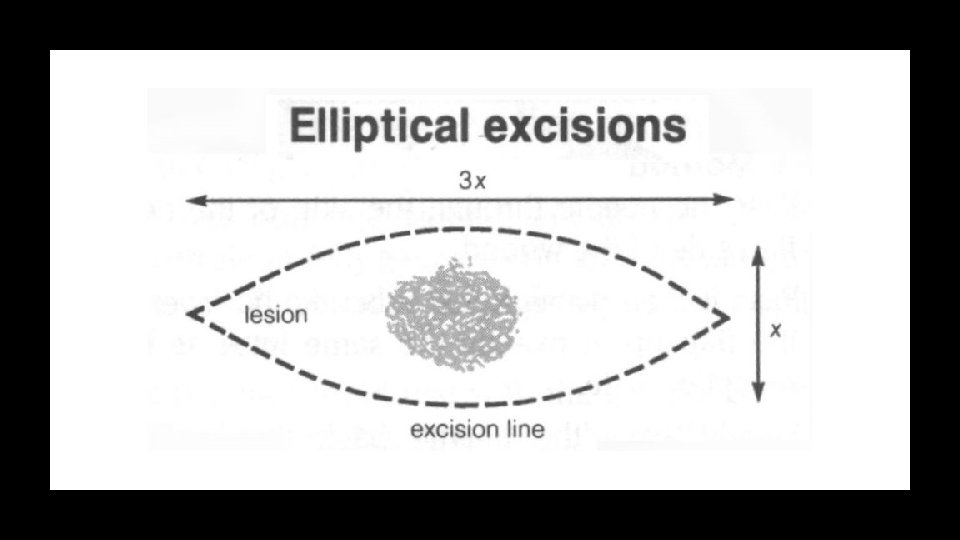
Coding Lesion Excision • Measuring and Coding of Lesion Removal • Per CPT - Excision is defined as full thickness removal of a lesion, including margins. • Code selection is based on measuring the greatest clinical diameter of the lesion plus the narrowest margins required for complete excision.
Lesion Measurement • Largest excised diameter plus margins • Lesion measuring 2. 0 cm x 1. 0 cm with 0. 2 cm margins = what? • 2. 0+0. 2 = 2. 4 cm? or • 2. 0+1. 0+0. 2 = 3. 4 cm?
Lesion Measurement • Examples of lesion at widest dimension + margin at narrowest width: • 1. 0 cm lesion with 0. 5 cm margin left and 0. 5 cm margin right = 2. 0 cm • 1. 0 cm x 2. 0 cm lesion with 1. 0 cm margin left and 1. 0 cm margin right = 4. 0 cm • 2. 5 cm x 0. 6 cm lesion with 0. 3 cm margin left and 0. 3 cm margin right = 3. 1 cm
Benign or Malignant Lesions • Code selection is based on: • Diagnosis (Pathology) • Location • Excised site with narrow margins
Benign Lesions • 11400 -11406 • Trunk, arms or legs • 11420 -11426 • Scalp, neck, hands, feet, genitalia • 11440 -11446 • Face, ears, eyelids, nose, lips, mucous
Malignant Lesions • 11600 -11606 • Trunk, arms or legs • 11620 -11626 • Scalp, neck, hands, feet, genitalia • 11640 -11646 • Face, ears, eyelids, nose, lips, mucous
Closure with Excisions • Adjacent tissue transfer or rearrangement excision of lesions are NOT reported separately • Simple closures are NOT reported separately with lesion excisions • Intermediate and Complex closures are reported in addition to the excision • Skin grafts are reported in addition to the excision
Repairs • Simple (12001 -12021) • Superficial, epidermis or dermis • Intermediate (12031 -12057) • Layered, deeper layers of sub-q tissue • Complex (13100 -13160) • Scar revision, debridement, undermining
Simple Repair • Used when the wound is superficial. • Typically involves the epidermis or dermis, or subcutaneous tissues without significant involvement of the deeper structure of the skin. • A ONE-layer closure
Intermediate Repair • Includes the repair of wounds that in addition to what is described in the Simple Repair, required layered closure of one or more of the deeper layers of subcutaneous tissue and superficial (nonmuscle) fascia, in addition to the skin closure. • Single layer closure of heavily contaminated wounds that have required extensive cleaning or removal of particulate matter also constitutes the use of intermediate repair codes.
Complex Repair • Includes the repair of wounds requiring more than layered closure, such as scar revision, debridement, extensive undermining, stents or retention sutures. • Necessary preparation includes creation of a defect for repairs or the debridement of complicated lacerations or avulsions.
Adjacent Tissue Transfer • Flaps (14000 -14350) • Also known as Z-plasty, W-plasty, Rotation Flap • Measured in square cm • Code determined based on location • As described per CPT; excision (including lesion) and/or repair by adjacent tissue transfer or rearrangement.
Adjacent Tissue Transfer • Skin graft necessary to closed secondary defect is considered an additional procedure. • The primary defect resulting from the excision and the secondary defect resulting from the flap design to perform the reconstruction are measured together to determine code selection.
Flaps and Grafts
Flaps and Grafts
Flaps and Grafts
Flaps and Grafts • Grafts (15002 -15278) • Split Thickness or Full Thickness • Allograft or Xenograft • STSG – Split Thickness Skin Grafts (Autograft) • In doing an STSG healthy upper layers of the skin are transplanted to the defective area • FTSG – Full Thickness Skin Grafts (Autograft) • In doing an FTSG the surgeon obtains a full thickness graft that includes the layers of the skin and blood vessels
Flaps and Grafts • Allograft (Donor Graft – Skin Substitute) • With an Allograft this is from a human donor, typically a cadaver • Xenograft (Porcine Graft – Skin Substitute) • With Xenograft, this typically is the skin of a pig that would be used to close the wound
Split Thickness/Full Thickness Grafts • Code range for STSG • 15100 -15101 (Truck, arms, and legs) • 15120 -15121 (Face, scalp, eyelids, mouth, neck, ears, orbits, genitalia, hands, feet and/or multiple digits) • Code range for FTSG • 15200 -15201 (Trunk) • 15220 -15221 (Scalp, arms, and legs) • 15240 -15241 (Forehead, cheeks, chin, mouth, neck axillae, genitalia, hands and feet) • 15260 -15261 (Nose, ears, eyelids, and lips)
Skin Substitute Grafts • Codes 15271 -15278 were added to CPT in 2012 to account for substitute products for skin replacement. • The codes cover the body area for coverage, total square centimeter of the wound surface, with add-on codes for additional increase in square centimeter of coverage materials.
Skin Substitute Grafts • Example: A 345 sq cm skin substitute graft of the right arm and a 95 sq cm substitute graft of the left arm • Codes: 15273, 15274 x 4
Kyphoplasty and Vertebroplasty
Documentation Issues • Things to look for: • Is a balloon used to create a cavity? Report kyphoplasty. • How many vertebral bodies are involved? • What type of imaging guidance is used?
Documentation Issues • Terminology changes • Kyphoplasty now referred to as “percutaneous vertebral augmentation” • Codes are found at 22513 -22515 • Codes are for one “ 1” vertebral body for the body areas listed: • Thoracic • Lumbar • Codes are unilateral or bilateral • Imaging is included
Documentation Issues • Vertebroplasty codes are 22510 -22512 • These are percutaneous codes • The codes are for one (1) vertebral body for the body areas listed: • Cervicothoracic • Lumbosacral • Codes are unilateral or bilateral • Bone biopsy is included • Imaging is included
Vertebroplasty
Kyphoplasty
Vertebroplasty • Vertebroplasty is often utilized because: • More extensive repair experience • Good pain relief record • Relatively quick procedure • Performed as an outpatient procedure • Less costly than kyphoplasty
Selective Catheter Placement
Documentation Issues • Which vessel and which order? • Use Appendix L of the CPT 4 manual. • Are other interventions performed (such as angioplasty)? • What services are bundled with the procedures?
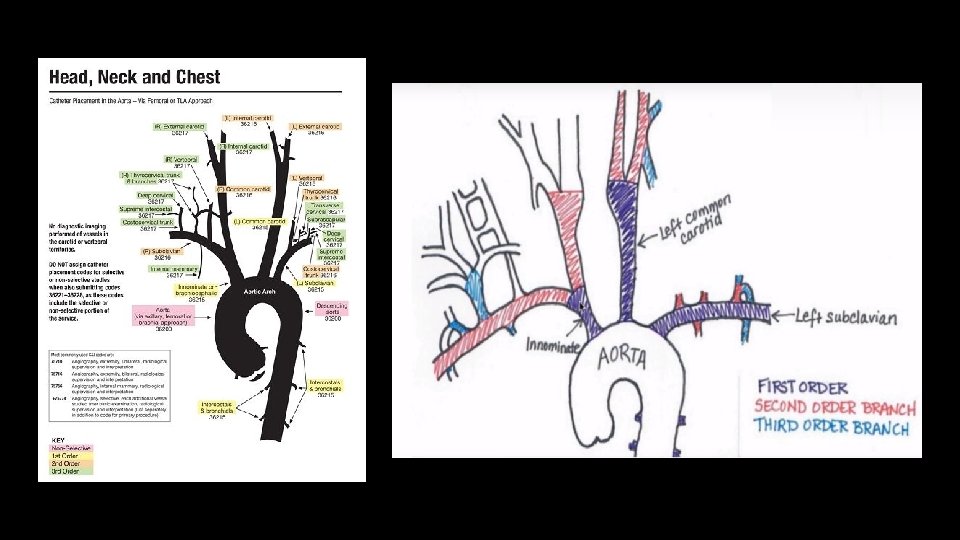
What Is Appendix L? • Appendix L is a tree of vascular families intended to help you assign codes for catheterizations performed assuming: • Normal anatomy • Catheterization started in the aorta
Selective Arterial Cath Placement • Codes 36215 -36218 used for thoracic and brachiocephalic arterial system • Codes 36245 -36248 used for abdominal, pelvic, and lower extremity • Codes 36251 -36254 used for renal arteries
Example Procedure • A catheter was placed into the abdominal aorta via the right common femoral artery access. Abdominal aortography was performed. These images demonstrated a patent single left renal artery, but the right renal artery was inadequately visualized. The catheter was used to selectively catheterize the right renal artery. Selective right renal angiography was then performed, demonstrating a widely patient right renal artery.
Endovascular Revascularization • For treatment of occlusive disease in lower extremities • Three territories 1) Iliac 2) Femoral/Popliteal 3) Tibial/Peroneal
Endovascular Revascularization • Codes arranged in a hierarchy for each territory • Stent placement with atherectomy (highest) • Atherectomy • Stent placement • Angioplasty (lowest)
Endovascular Revascularization • Services which are bundled in the procedure: • Conscious sedation • Vascular access • Catheter placement • Traversing the lesion • Imaging related to the intervention (previously billed as supervision and interpretation code for specific intervention) • Use of embolic protection device (EPD) • Imaging for closure device placement • Closure of the access site
Hernia Repairs
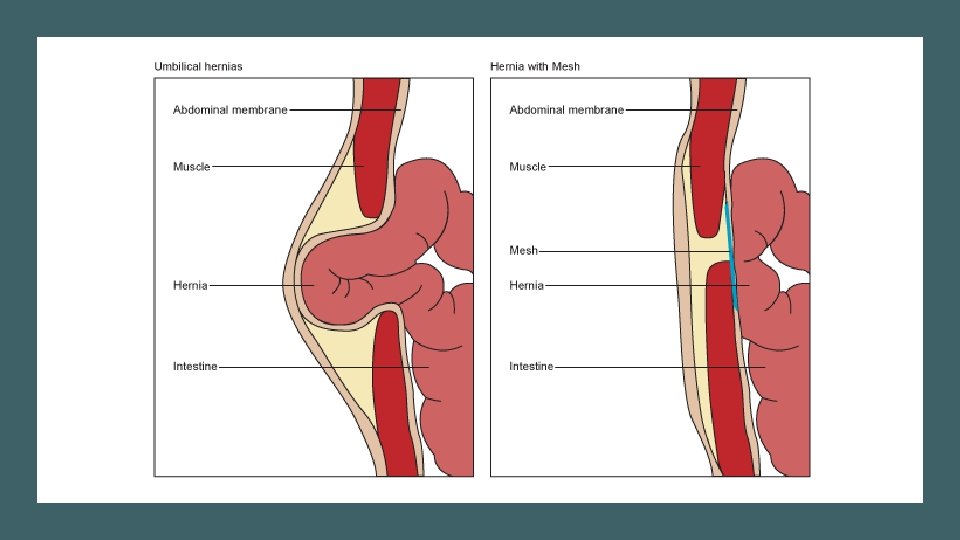
Documentation Issues • What type of hernia is it? • Is it recurrent or initial? • Is it incarcerated or strangulated? • What is the age of the patient? • Is mesh used and can it be reported with the type of hernia repair?
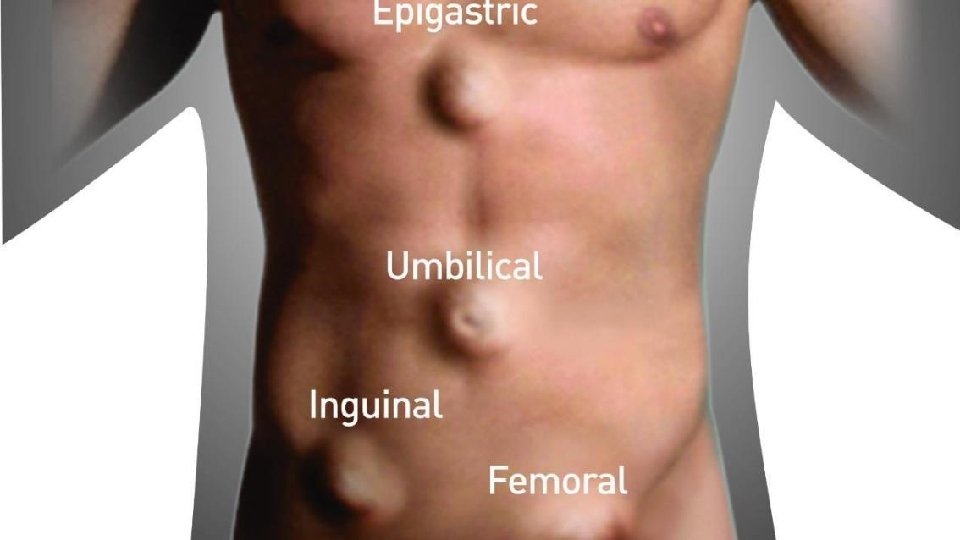
Documentation Issues • A hernia is an abnormal protrusion of the whole or part of a viscus through an opening in the wall or cavity which contains it. • Inguinal (groin) Hernia – commonly occurs in males, multiple in type: • Dual/Pantaloon/Saddle – both direct and indirect sacs • Sliding – retroperitoneal organ is part of the sac • Richter’s – only part of circumference of the small gut is obstructed • Maydl’s – a “W” shaped hernia • Littre’s – Meckel’s diverticulum • Amyand’s - Appendix
Documentation Issues • Femoral Hernia • Laugier’s – through lacunar ligament • Serofini’s – occurs behind femoral vessels • Teale’s – in front femoral vessels • Callison-Cloquet – through pectineal fascia • Hesselbach’s – occurs lateral to femoral artery • Narath’s – occurs behind femoral artery, in congenital dislocation of hip
Documentation Issues • Ventral Hernia – any protrusion through the anterior abdominal wall is referred to as a “ventral hernia” • Categorized as “spontaneous” or “acquired” • Spontaneous – primary defects in abdominal fascia includes: • Umbilical and periumbilical hernia • Epigastric hernia • Spigelian hernia • Acquired – incisional hernia and parastomal hernia • NOTE: CPT groups ventral, umbilical, Spigelian, or epigastric hernia together in the code set.
Example Case • Preoperative Diagnosis: Lower left inguinal pain Postoperative Diagnosis: Inguinal hernia Procedure: This 30 -year-old patient presented with lower left inguinal pain and on examination was found to have a left inguinal hernia. The decision to perform a left inguinal hernia repair was made. The procedure was performed in the outpatient hospital surgery center. Risks and benefits of the surgery were discussed with the patient and the patient decided to proceed with the surgery. A skin incision was placed at the umbilicus where the left rectus fascia was incised anteriorly. The rectus muscle was retracted laterally. Balloon dissector was passed below the muscle and above the peritoneum. Insufflation and deinsufflation were done with the balloon removed.
Example Case (continued) • The structural balloon was placed in the preperitoneal space and insufflated to 10 mm Hg carbon dioxide. The other trocars were placed in the lower midline times two. The hernia sac was easily identified and was well-defined. It was dissected off the cord anteromedially. It was an indirect sac. It was taken back down and reduced into the peritoneal cavity. The cord, structures, and vas were left intact. The trocars were removed. The wounds were closed with 0 Vicryl for the fascia, 4 -0 for the skin. Steri-Strips were applied. The patient was awakened and carried to the recovery room in good condition, having tolerated the procedure well. • What is the correct CPT 4 and/or modifier code for assignment?
Circumcision
Documentation Issues • Is a clamp or device used? • What is the age of the patient? • Is a dorsal penile or ring block performed?
Circumcision • When coding for circumcision, if a clamp or device is used, report 54150 regardless of age. It includes dorsal penile or ring block. • If the block is not performed, append modifier 52 per CPT. • If excision without device, code based on age. • 28 days or less report 54160 • Older than 28 days report 54161
Example Case • Newborn male (10 days old) is scheduled for a circumcision. He is sterilely prepped and draped; a penile nerve block is performed. The circumcision is performed by a ring device. Hemostasis is achieved. Vaseline Gauze dressing applied. Patient tolerated the procedure well. • What is the correct CPT 4 and modifier code for assignment?
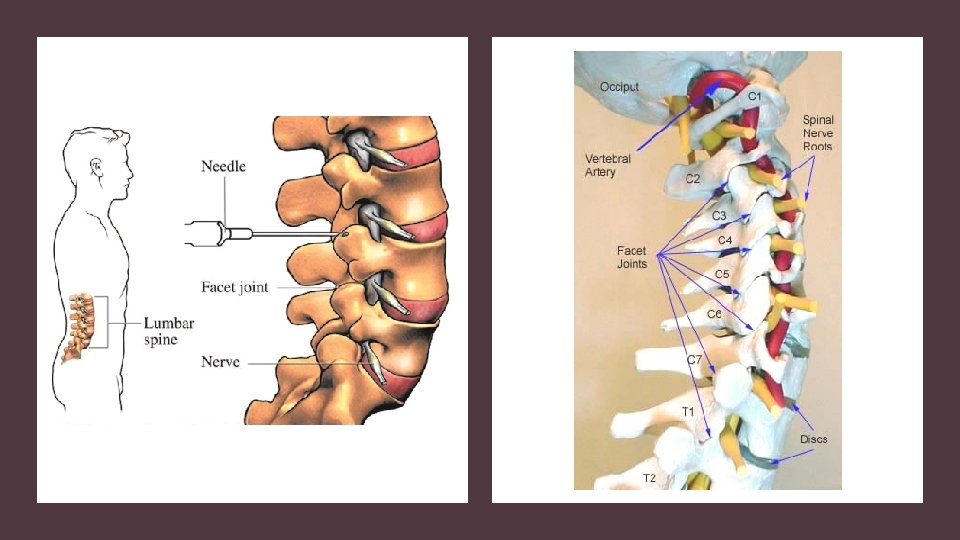
Facet Joint Injections
Documentation Issues • Which region of the spine is the procedure performed? • How many levels is the procedure performed on? • Is it performed bilaterally? • What type of imaging guidance is used?
Facet Joint Injections • Codes selected based on the region of the spine and per level. • Imaging and injection of contrast are included. • Use modifier 50 for bilateral procedures. • Codes 64492 and 64495 can only be reported once per day. • If imaging is not used, report 20552 -20553.
Facet Joint Injections • Cervical or thoracic with fluoroscopic or CT imaging guidance, report: • 64490 for the first level • 64491 for the second level • 64492 for the third any additional levels
Facet Joint Injections • Lumbar or sacral with fluoroscopic or CT imaging guidance, report: • 64493 for the first level • 64494 for the second level • 64495 for the third any additional levels
Facet Joint Injections • Cervical or thoracic with ultrasound imaging guidance, report • 0213 T for the first level • 0214 T for the second level • 0215 T for the third any additional levels
Facet Joint Injections • Lumbar or sacral with ultrasound imaging guidance, report • 0216 T for the first level • 0217 T for the second level • 0218 T for the third any additional levels
Example Case • The residual cervical facet joints at the right C 3 -C 4, C 4 -C 5, C 5 -C 6, C 6 -C 7, C 7 -T 1 distributions were identified under the multiplanar fluoroscopic imaging and guidance. A selective cervical facet block at each of the described levels was then completed with a total of 2 cc Marcaine, 0. 5%, with 2 mg Kenalog per cc, and 3 mg of Toradol per cc, 1. 5 cc intra-articular and 0. 5 cc peri-articular, to include appropriate dye dilution of the medial branch innervation at each level. The needles were removed. There was no evidence of hematoma. Sterile Band-Aids were placed, and ice was placed to reduce and postoperative swelling from the needle. • What CPT 4 code/modifier(s) are assigned?
Unlisted Codes
Unlisted Codes • A service or procedure may be provided that is not listed in this edition of the CPT® codebook. When reporting such a service, the appropriate “Unlisted Procedure” code may be used to indicate the service, identifying it by “Special Report” as discussed in the section below. • NOTE: Verify that a code from another section would not be used instead. • For example a procedure on the lips, the CPT® code appropriate for the case may be located in the digestive system chapter.
Vaccine Administration
Documentation Issues • Was counseling performed by a qualified health care provider? • If counseling was performed what is the patient’s age? • If counseling is performed for a patient up to age 18, how many vaccines administered and how many components does each vaccine include? • If counseling is not performed, what is the route and number administered?
Vaccine Administration • 90460 Immunization administration through 18 years of age via any route of administration, with counseling by physician or other qualified health care professional; first or only component of each vaccine or toxoid administered • 90461 each additional vaccine or toxoid component administered (List separately in addition to code for primary procedure) • Note: counseling, the age, any route, 90460 is reported for each administration and 90461 is coded for each additional component of the vaccination
Vaccine Administration • 90471 Immunization administration (includes percutaneous, intradermal, subcutaneous, or intramuscular injections); 1 vaccine (single or combination vaccine/toxoid) • 90472 each additional vaccine (single or combination vaccine/toxoid) (List separately in addition to code for primary procedure) • Note: it is not age specific, no counseling, the route, is only listed once and is the add-on for each additional vaccine, NO COMPONENT CODING
Vaccine Administration • 90473 Immunization administration by intranasal or oral route; 1 vaccine (single or combination vaccine/toxoid) • 90474 each additional vaccine (single or combination vaccine/toxoid) (List separately in addition to code for primary procedure) • Note: it is not age specific, no counseling, the route, is only listed once and is the add-on for each additional vaccine, NO COMPONENT CODING
Administration Example #1 • The following vaccine are administered to a 3 year old. The physician performs counseling: • 90743 Hepatitis B • 90680 Rotavirus • 90700 Diphtheria, Tetanus, Pertussis • 90648 Haemophilus influenza type b • 90669 Pneumococcal • 90713 Inactivated Poliovirus
Administration Example #2 • The following vaccine are administered to a 3 year old. The physician DOES NOT perform counseling: • 90743 Hepatitis B • 90680 Rotavirus • 90700 Diphtheria, Tetanus, Pertussis • 90648 Haemophilius influenza type b • 90669 Pneumococcal • 90713 Inactivated Poliovirus
Vaccine Administration • Do not report 99211 if the patient presents for vaccines only • If the vaccines are performed on the same date as a well visit, report the preventive E/M with the vaccines • Know the administration codes used by Medicare • G 0008 Administration of influenza virus vaccine • G 0009 Administration of pneumococcal vaccine • G 0010 Administration of hepatitis B vaccine • Report in addition to the vaccine
Modifiers
Modifier 91 • Only reported with lab codes (80000 series) • Not reported when there is a problem with the specimen • Not reported when a code includes multiple specimens • Example GTT includes three specimens
Modifier 91 Example • Example • Provider orders 2 arterial blood gases to be performed throughout the day. • 82803, 82803 -91
Modifier 76 • Repeat Procedure or Service by Same Physician or Other Qualified Health Care Professional • Can be reported with surgical, radiology and medicine codes
Modifier 76 • Example: • Provider orders 2 EKGs to be performed while in the patient is in the office. The physician performs the interpretations. • 93000, 93000 -76
ICD-10 -CM
ICD-10 -CM • The official guidelines for ICD-10 -CM are in the front of the ICD manual each year. With the change from ICD-9 to ICD-10 there are numerous things coders should be aware of. • Be sure you are not only familiar with these guidelines, but know where to find them if necessary during your testing.
ICD-10 -CM • The official guidelines for ICD-10 -CM are in the front of the ICD manual each year. With the change from ICD-9 to ICD-10 there are numerous things coders should be aware of. • These guidelines are also referred to and called “conventions. ” • Be sure you are not only familiar with these guidelines, but know where to find them if necessary during your testing.
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM
ICD-10 -CM | Burns • Categories T 20 -T 25 are for current burns and classified by: • Depth • Extent • Agent (X code) • Always code to the greatest depth of the burn in a given category/anatomical area. • Sequence first the diagnosis that reflects the highest degree of burn when multiple burns are present. • Classify burns of the same local site but of different degrees to the subcategory identifying the highest degree of burn.
ICD-10 -CM | Burns • Example • Patient suffers third degree burns to his right and left thighs (9%) and second degree burns to the abdomen (9%) • Answer • T 24312 A Burn of third degree of left thigh, initial encounter • T 24311 A Burn of third degree of right thigh, initial encounter • T 2122 XA Burn of second degree of abdominal wall, initial encounter • T 3110 Burns involving 10 -19% of body surface with 0% to 9% third degree burns
ICD-10 -CM | Burns
ICD-10 -CM | Burns
ICD-10 -CM | Burns
HIPAA
HIPPA • What does this acronym stand for? • Health Insurance Portability and Accountability Act of 1996 • How many parts are there in HIPAA? • Five Parts • Which part/title is most important to coders? • Title II – Preventing Healthcare Fraud & Abuse, Administration Simplification, and Medical Liability Reform
HIPPA • Administration Simplification addresses the need for increased technology for: • National standards for electronic health care transactions and code sets • National unique identifiers for providers, health plans, and employers • Privacy and Security of health data
HIPPA • A “covered entity” is defined by HIPAA as: • A healthcare provider, such as: • Doctors • Clinics • Psychologists • Dentists • Chiropractors • Nursing homes • Pharmacies
HIPPA • A “covered entity” is defined by HIPAA as: • A health plan, to include: • Health insurance companies • HMOs • Company health plans • Government programs that pay for healthcare, such as Medicare, Medicaid, and the military and veterans’ healthcare programs
HIPPA • A “covered entity” is defined by HIPAA as: • A health plan, to include: • Workers’ compensation or similar insurance • Automobile medical payment insurance • Credit-only insurance • Coverage for on-site medical clinics • Other similar insurance coverage, specified in regulations, under which benefits for medical care secondary or incidental to other insurance benefits
HIPPA • A “covered entity” is defined by HIPAA as: • A healthcare clearinghouse: • This includes entities that process nonstandard health information they receive from another entity into a standard format (such as a standard electronic format or data content), or vice versa
HIPPA • HIPAA sets standards for electronic healthcare transactions and code sets which include: • Health claims and equivalent encounter info • Enrollment and disenrollment in a health plan • Eligibility for a health plan • Healthcare payment and remittance advice • Health claim status • Referral certification and authorization • Coordination of benefits
HIPPA • Any covered entity performing one of those transactions electronically is required to follow the standards set for that transaction, and the standards and codes include: • HCPCS • CPT • ICD-10 -CM • NDC (National Drug Codes)
Medical Terminology
Medical Terminology • Use your code books to help you with terms you may not remember • Both ICD and CPT have lots of valuable information in them in this area and also there are illustrations in professional editions • When you unsure of a term or abbreviation, look it up in the index of the code books for assistance.
Thanks for attending