Covered Versus Uncovered Iliac Artery Stents J Fritz





















 is a statistical technique")


- Slides: 40
Covered Versus Uncovered Iliac Artery Stents J. Fritz Angle, M. D. University of Virginia Charlottesville, VA
Disclosures Research Support: Proteon Siemens Medical
Meta Analysis of Literature • • • 19 studies: 12 case series, 6 retrospective series, and 1 randomized controlled trial Some but not statistically significant difference in primary patency at 1, 2, and 3 to 5 years for covered stents compared with bare-metal stents: 91. 7% vs. 88. 5%, 85. 4% vs. 80. 9%, and 80. 7% vs. 72. 0%, respectively Several studies found a significant difference in TASC C and D but not with A/B lesions Aortic bifurcation lesions likely benefit from CS Authors point out difficulty with TASC being imprecise with lesion location and length and whether it is an occlusion or stenosis Bekken JA, Jongsma H, Fioole B. The use of covered stents in aortoiliac obstructions: a systematic review and meta-analysis. J Cardiovasc Surg 2018; 59: 14 -25.
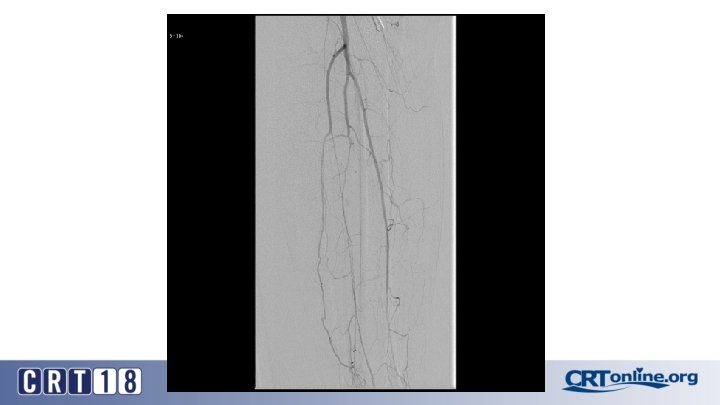
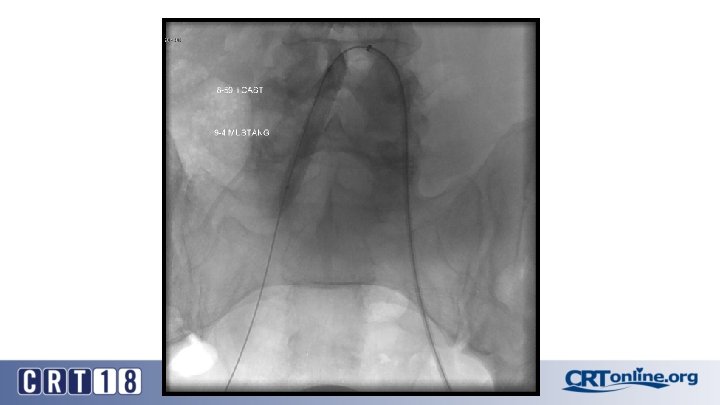
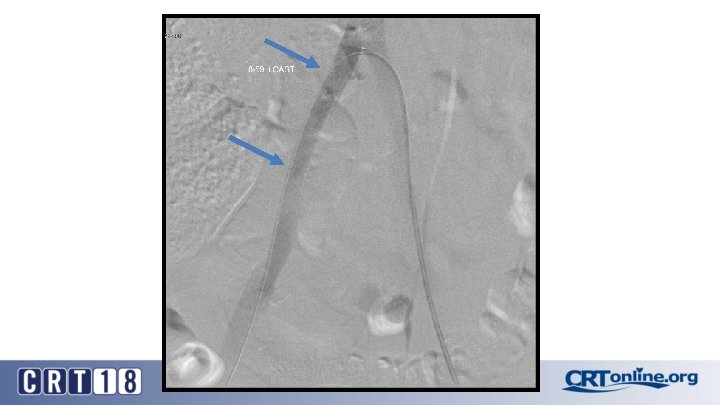
Blue Toe Syndrome
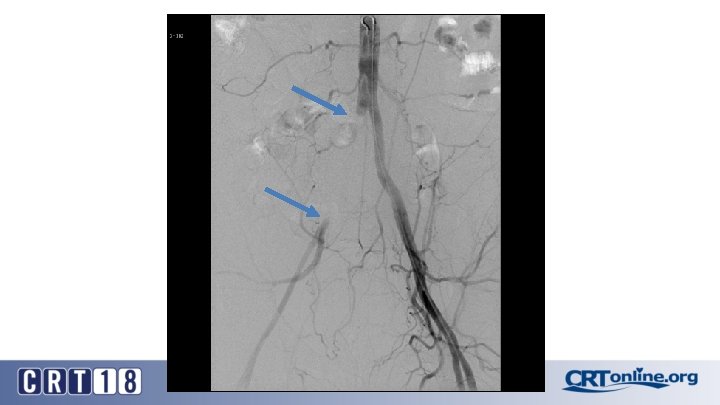
Returns Next day
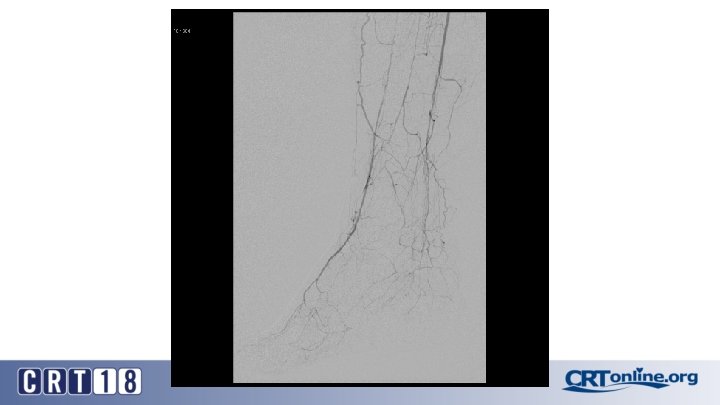
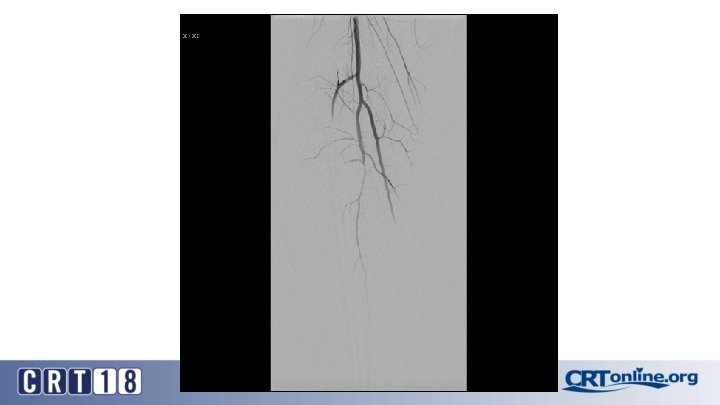
Failed recanalization: BKA
Case selection bias leads to wide ranging conclusions • Only one RCT of CS versus BMS (Mwipatayi, 2011): CS ultrasound based restenosis and TLR superior to BMS) • One large recent case series (Revuelta, 2014): BMS patency at 30 months markedly superior to CS for TASC C/D • Unlikely to see additional RCT given low failure rate of all iliac stents • All these studies have case selection bias • We need a way to dive into the sub-groups that preoccupy our thinking about stent selection without a prospective blinded trial Revuelta S, et al. Endovascular treatment of external iliac artery occlusive disease: midterm results. J Endovasc Ther. 2014; 21(2): 223 -9.
Propensity score analysis • • • Propensity score matching (PSM) is a statistical technique that attempts to better estimate the effect of a intervention by accounting for the covariates that predict who will get a particular treatment PSM attempts to reduce the bias due to confounding variables that could be hidden or ignored when simply comparing treatment outcomes It is a linear combination of known covariates into a single score It balances treatment and control groups on a number of covariates without losing a large number of observations. (i. e. if the treatment and control groups were balanced on a number of covariates one at a time, large numbers of observations would be needed) Caveat: it can only balance out measurable co-variables and cannot balance hidden factors in device selection Vikatmaa P. Commentary on "Outcomes of Self Expanding Polytetrafluoroethylene Covered Stent versus Bare Metal Stent for Chronic Iliac Artery Occlusion in Matched Cohorts Using Propensity Score Modeling". Eur J Vasc Endovasc Surg. 2017; 54: 186.
CS Compared to BMS in iliac occlusion • 2009 and December 2015, 128 iliac artery occlusions were stented • A CS was implanted in 78 iliac arteries (61%) and a BMS in 50 (49%) • After propensity score matching (lesion site and length separated and associated femoropopliteal disease included) (47 for each group). • Technical success was 98% • Complication rates same: 12% vs. 12%, p = 1. 0 • 30 day mortality rates same: 2% vs. 2%, p = 1. 0 Piazza M, et al. Outcomes of polytetrafluoroethylene-covered stent versus bare-metal stent in the primary treatment of severe iliac artery obstructive lesions. J Vasc Surg. 2015; 62(5): 1210 -8.
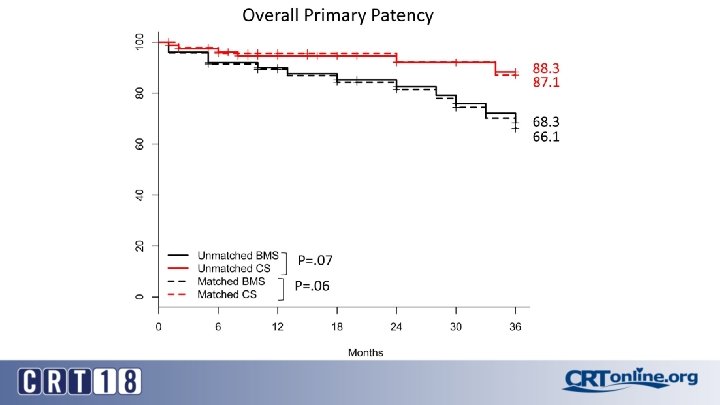
CS superior to BMS, in the right setting • At 36 months (average 23 ± 17) overall primary patency only approached significance: 87% vs. 66%, p =. 06 • For TASC D, CS: 88% vs. BMS: 54% (p =. 03) • Patency was in favor of CSs for occlusions > 3. 5 cm in length (p =. 04), total lesion length > 6 cm (p =. 04), and occlusion with calcification > 75% of the arterial wall circumference (p =. 01) • Kissing stent patency also superior with CS