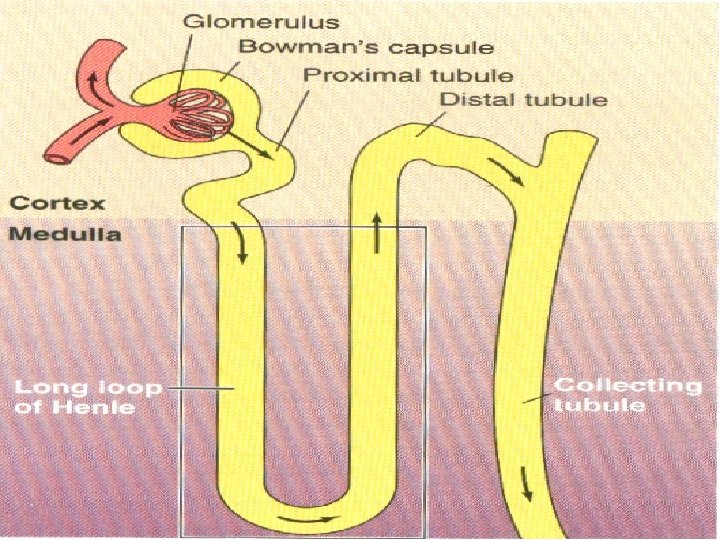
Counter Current system2 Before the vertical osmotic gradient

Counter Current system-2

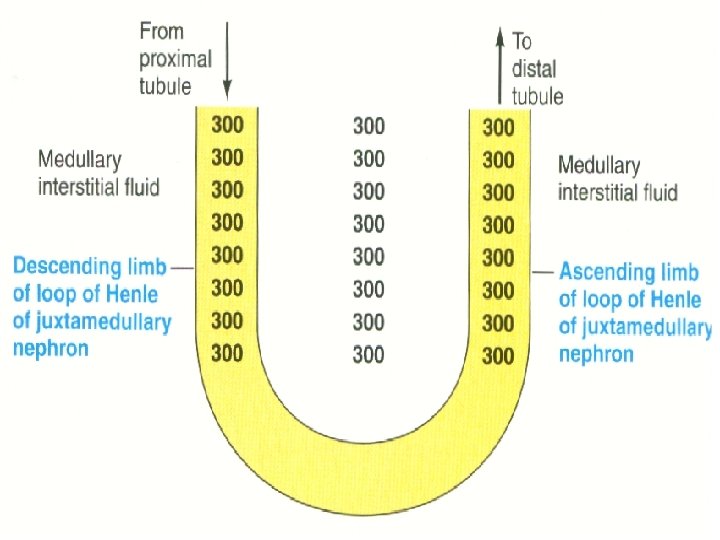
• Before the vertical osmotic gradient is established, the medullary interstitial fluid concentration is uniformly 300 m Osm/L as in the remainder of the body fluids

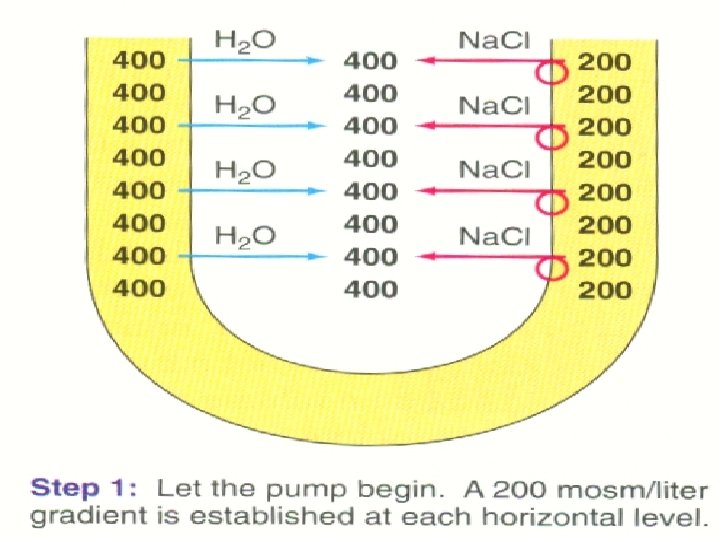
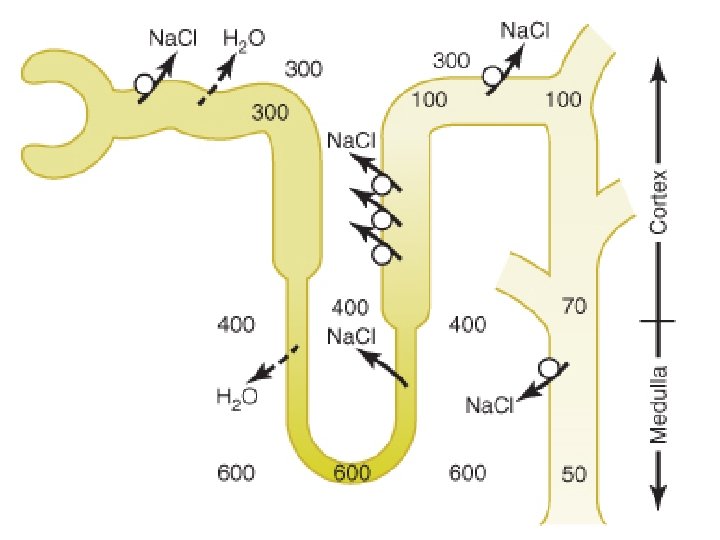
Step- 1 • The active salt pump in the thick ascending limb is able to transport Na. Cl out of the lumen until the surrounding interstitial fluid is 200 m. Osm/l more concentrated than the tubular fluid in this limb
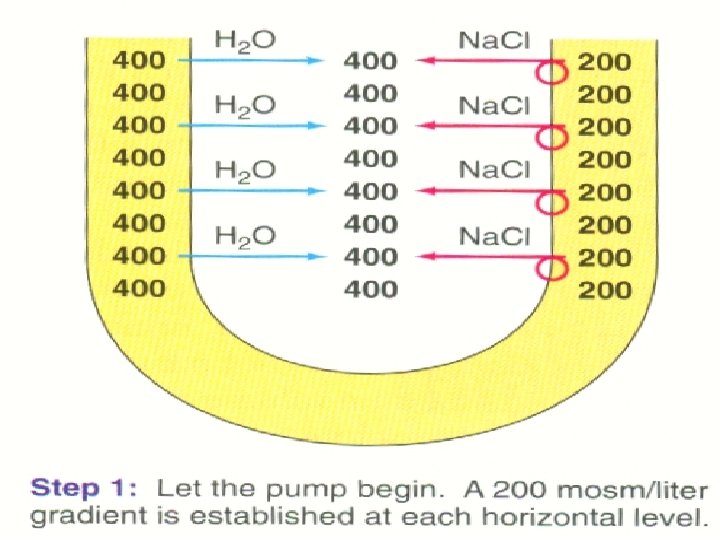

• When the thick ascending limb pump starts actively extruding salt the medullary interstitial fluid becomes hypertonic • Passive diffusion of sodium chloride from the thin ascending limb (impermeable to water) also adds to the increase solute conc

• Descending limb is highly permeable to water, net diffusion of water by osmosis from descending limb into the more concentrated interstitial fluid • Passive movement of water continues until the osmolarities of the fluid in the descending limb and interstitial fluid become equilibrated
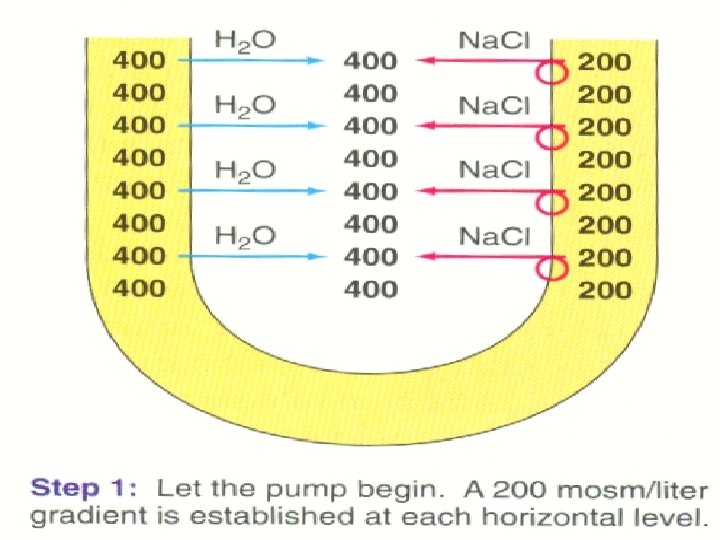

• Tubular fluid entering the loop of Henle immediately starts to become more concentrated as it loses water • At equilibirum, the osmolarity of the ascending limb fluid is 200 m. Osm/L and the osmolarities of the interstitial fluid and descending limb fluid are equal at 400 m. Osm/liter

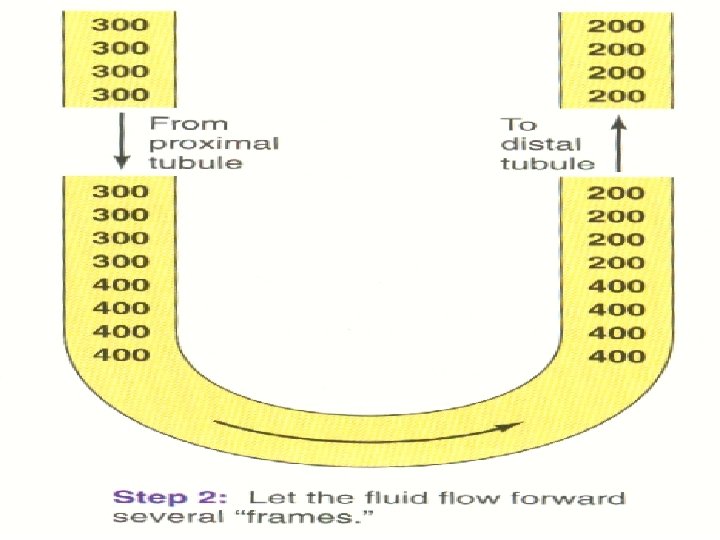
Step- 2 • 200 m. Osm/L fluid exits from the top of the ascending limb into the distal tubule • New mass of isotonic fluid at 300 m. Osm/L enters the top of the descending limb from the proximal tubule

• At the bottom of the loop, mass of 400 m. Osm/L fluid from the descending limb moves forward around the tip into the ascending limb • The 200 m. Osm/L concentration difference has been lost at both the top and the bottom of the loop

Step - 3 • The ascending limb pumps again Na. Cl out while water passively leaves the descending limb until a 200 m. Osm/liter difference is reestablished between the ascending limb and both the interstitial fluid and descending limb at each horizontal level
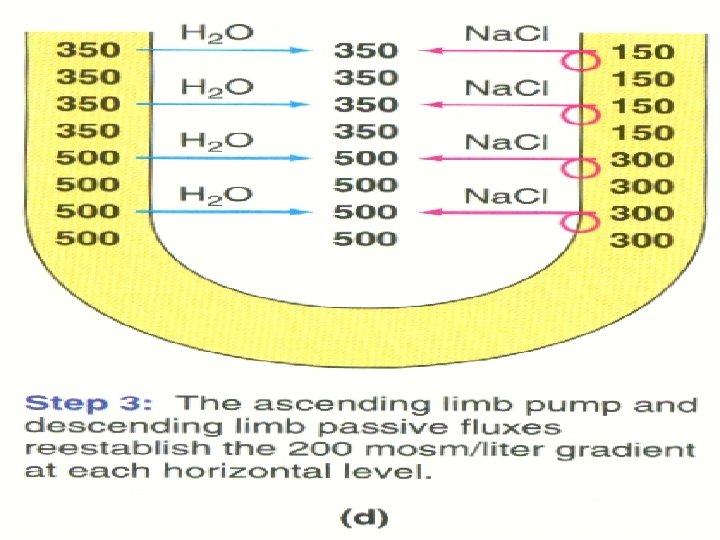

• The concentration of tubular fluid is progressively increasing in the descending limb and progressively decreasing in the ascending limb

Step- 4 • As the tubular fluid advances still further, the 200 m. Osm/L concentration gradient is disrupted once again at all horizontal levels
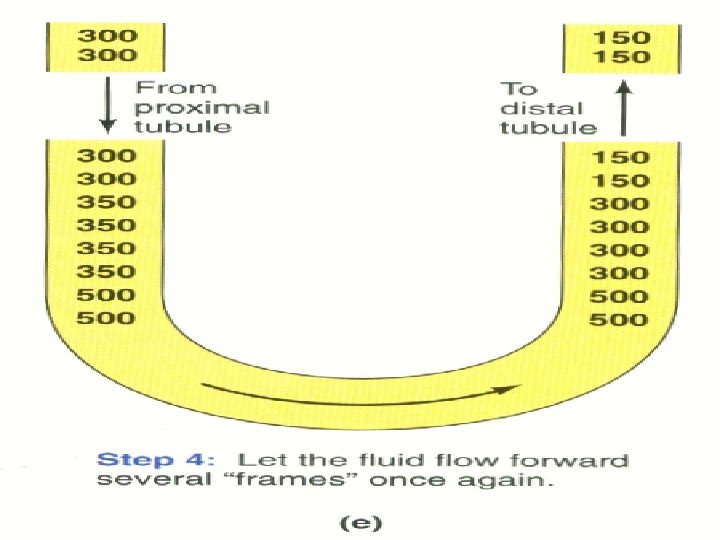

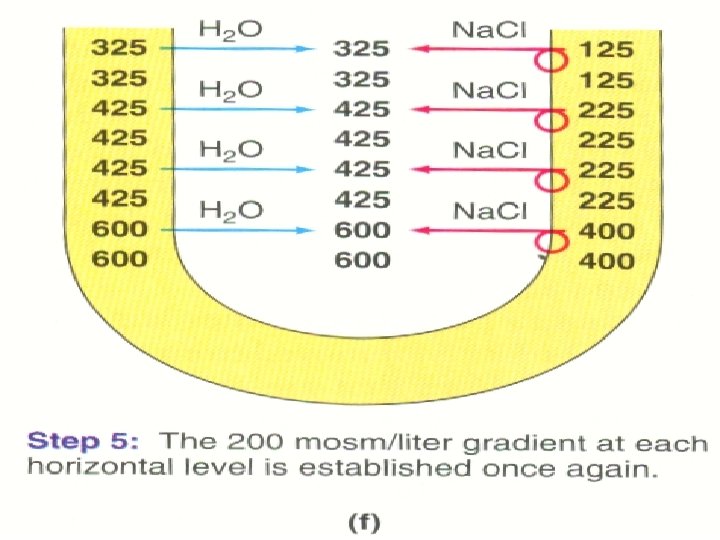
Step- 5 • Again active extrusion of Na. Cl from the ascending limb coupled with the net diffusion of water out of the descending limb reestablishes the 200 m. Osm/L gradient at each horizontal level

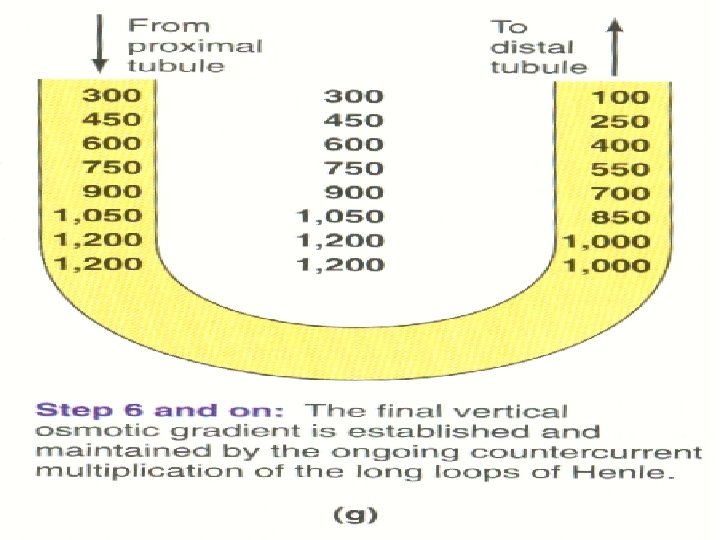
Step- 6 • Tubular fluid flows slightly forward again and the stepwise process continues • Fluid in the descending limb becomes progressively more hypertonic until it reaches a maximum concentration of 1, 200 m. Osm/L at the bottom of the loop
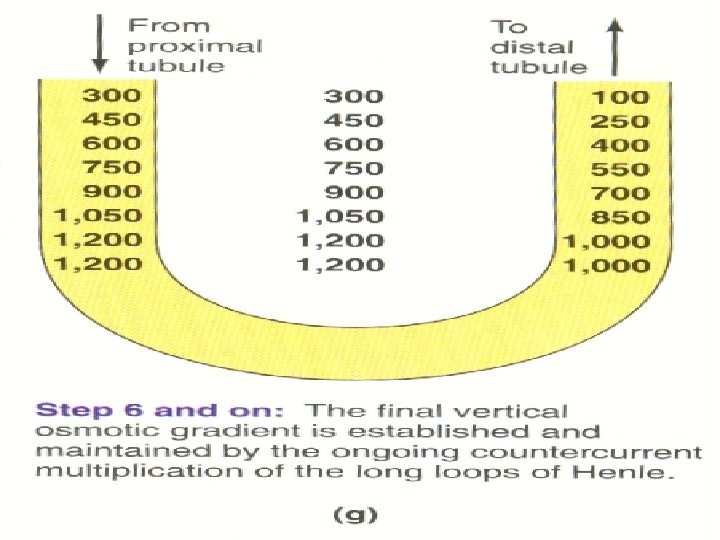

• Because the interstitial fluid always achieves equilibrium with the descending limb vertical concentration gradient ranging from 300 to 1, 200 m. Osm/L is established in the medullary interstitial fluid

• Concentration of the tubular fluid progressively decreases in the ascending limb as salt is pumped out • Tubular fluid even becomes hypotonic as it leaves the ascending limb to enter the distal tubule at a concentration of 100 m. Osm/L

• Sodium ions are repeatedly recycled within the medullary interstitium.


• The loop of Henle multiplies the sodium concentration within medulla by retaining the new sodium ions coming from the glomerular filtrate. It is called Counter Current Multiplier

Role Of Distal Tubule • Fluid leaves the loop of Henle and enters the distal convoluted tubule in the renal cortex • This fluid has an osmolarity of 100 m. Osm/L. • Na. Cl is transported out of the tubule but this part is relatively impermeable to water.

• End Of Todays Lecture!!
- Slides: 32