Coronary Revascularization Percutaneous Coronary Intervention Rita Coram MD




. Sotiris C. Stamou")











 and angiographic diameter")



- Slides: 30
Coronary Revascularization : Percutaneous Coronary Intervention Rita Coram, MD FACC Director, Women’s Cardiovascular Health Program Director, CCU and Chest Pain Center, ULH
From: A Global Risk Approach to Identify Patients With Left Main or 3 -Vessel Disease Who Could Safely and Efficaciously Be Treated With Percutaneous Coronary Intervention: The SYNTAX Trial at 3 Years J Am Coll Cardiol Intv. 2012; 5(6): 606 -617. doi: 10. 1016/j. jcin. 2012. 03. 016 Figure Legend: The Proposed Global Risk The Global Risk demonstrating recategorization of established tertiles of risk for the SYNTAX Score and additive Euro. SCORE to form low (GRCLOW), intermediate (GRCINT), and high (GRCHIGH) Global Risk groups. Highlighted (dashed) boxes indicate patients moved (reclassified) into or out of the low SYNTAX Score group to form the low Global Risk group (GRCLOW). Date of download: 5/14/2015 Copyright © The American College of Cardiology. All rights reserved.
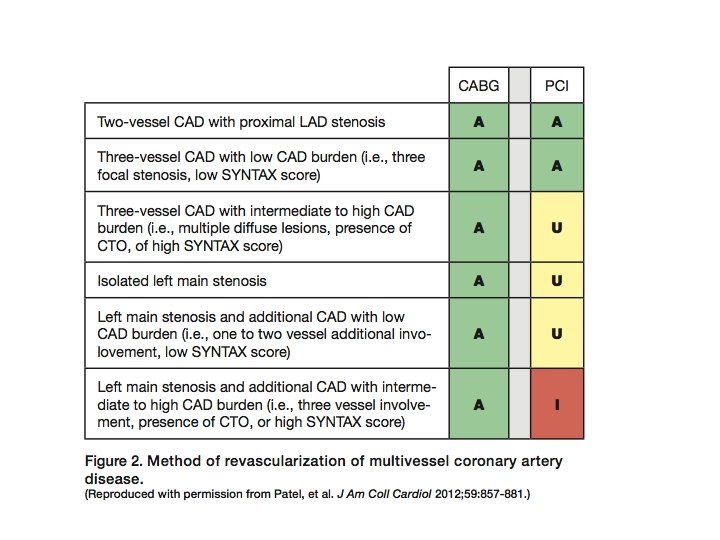
Our Patient • • • Not diabetic 2 Vessel CAD sparing the Left Main Syntax score NOT in the highest tertile Female Elderly Calcified aorta
AGE- Older than 75 Among patients older than 75 years of age, the early invasive strategy conferred an absolute reduction of 10. 8 percentage points (to 10. 8% from 21. 6%; P=0. 016) and a relative reduction of 56% in death or MI at 6 months; however, benefits came with an increased risk of major bleeding events (16. 6% vs 6. 5%; P=0. 009). A recent retrospective review of 662 033 patients who underwent cardiac surgical procedures performed using the STS National Cardiac Database 962 found a CABG operative mortality of 2. 8% for patients 50 to 79 years of age, 7. 1% for patients 80 to 89 years of age, and 11. 8% for patients aged 90 years or more.
Independent predictors of postoperative stroke after CABG (multivariate logistic regression analysis). Sotiris C. Stamou et al. Stroke. 2001; 32: 1508 -1513 Copyright © American Heart Association, Inc. All rights reserved.
EDWARDS et al Ann Thorac Surg. 1998; 66: 125– 31
The American Heart Association and the American College of Cardiology, in collaboration with the American Association for Thoracic Surgery and the Society of Thoracic Surgeons, note that in-hospital CABG mortality is on average greater in women than in men, and sometimes, but not always, this disparity was reduced after adjustment for use of IMA grafts, age, and BSA.
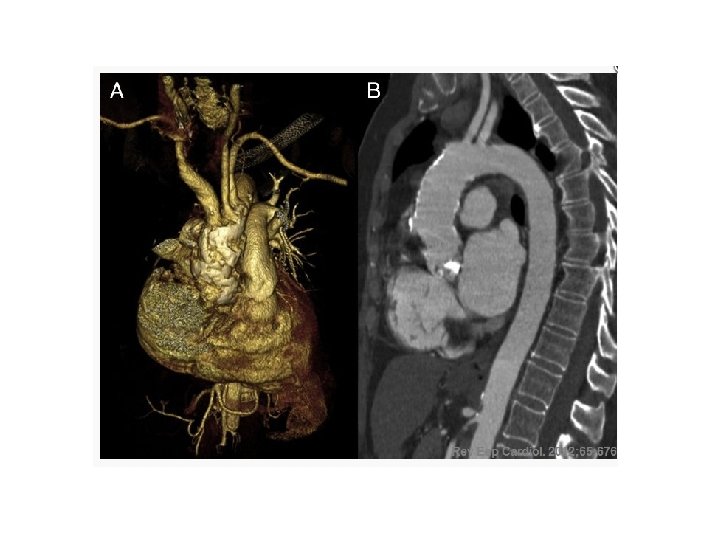
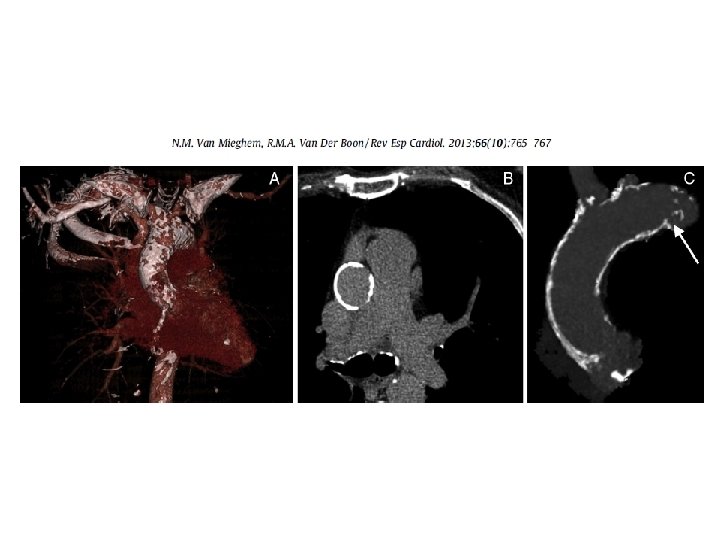
Porcelain Aorta Kang M, Ha J. N Engl J Med 2012; 366: e 40.
Single aortic clamping in coronary artery bypass surgery reduces cerebral embolism and improves neurocognitive outcomes Hrvoje Gasparovic, Vascular Medicine 18(5) 275– 281
Blauth Cl, Cosgrove DM, Lytle BW, Loop FD Department of Thoracic and Cardiovascular Surgery, Cleveland Clinic Foundation, OH The Journal of Thoracic and Cardiovascular Surgery [1992, 103(6): 1104 -11; discussion 1111 -2] As the ages of patients undergoing cardiac operations have increased, noncardiac causes of death have increased. To identify these causes of death, we analyzed the autopsy findings in 221 patients undergoing myocardial revascularization or valve operations between 1982 and 1989. Mean age was 65. 6 +/- 9. 5 years and the range was from 32 to 94 years; 130 patients (58. 8%) were male. Autopsies were complete in 129 patients (58. 4%) and limited to the chest and abdomen in the remainder. Embolic disease was identified in 69 patients (31. 2%). Atheroemboli or abnormalities consistent with atheroemboli were identified in 48 patients (21. 7%). Fourteen patients had thromboembolism and 7 had disseminated intravascular coagulation. The prevalence of atheroembolic disease increased dramatically from 4. 5% in 1982 to 48. 3% in 1989 (p = 0. 001). Atheroembolic disease was found in the brain in 16. 3% of patients, spleen in 10. 9%, kidney in 10. 4%, and pancreas in 6. 8%. Thirty (62. 5%) of the 48 patients had multiple atheroembolic sites. Atheroemboli were more common in patients undergoing coronary artery procedures (43/165; 26. 1%) than in those undergoing valve procedures (5/56; 8. 9%) (p = 0. 008). There was a high correlation of atheroemboli with severe atherosclerosis of the ascending aorta. Atheroembolic events occurred in 46 of 123 patients (37. 4%) with severe disease of the ascending aorta but in only 2 of 98 patients (2%) without significant ascending aortic disease (p less than 0. 0001). Fortysix of 48 patients (95. 8%) who had evidence of atheroemboli had severe atherosclerosis of the ascending aorta. There was a direct correlation between age, severe atherosclerosis of the ascending aorta, and atheroemboli. Incremental risk factors for atheroembolic are peripheral vascular disease and severe atherosclerosis of the ascending aorta.
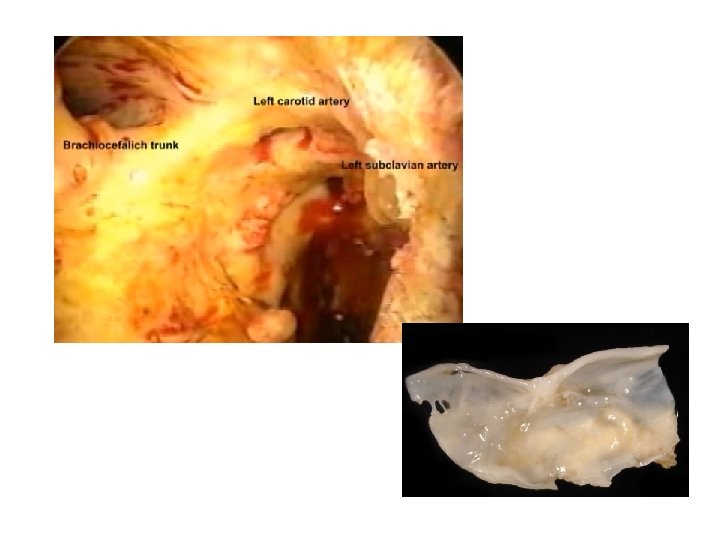
Emboli capture using the Embol-X intraaortic filter in cardiac surgery: a multicentered randomized trial of 1, 289 patients Michael K Banbury , Nicholas T Kouchoukos , Keith B Allen , Mark S Slaughter , Neil J Weissman , Gerald J Berry , . . . The Annals of Thoracic Surgery, Volume 76, Issue 2, 2003, 508 - 515 Fig 2 Captured particulate emboli. (A) Filter with captured particulate emboli. (B) Photomicrograph of captured fibrous atheroma (10 ×, 3 -mm grid). (C) Organized thrombus captured by the filter.
Emboli capture using the Embol-X intraaortic filter in cardiac surgery: a multicentered randomized trial of 1, 289 patients Michael K Banbury , Nicholas T Kouchoukos , Keith B Allen , Mark S Slaughter , Neil J Weissman , Gerald J Berry , . . . The Annals of Thoracic Surgery, Volume 76, Issue 2, 2003, 508 - 515
Brain Injury from Cardiac Surgery is a Spectrum of Disorders
Figure 3 Cardiopulmonary Bypass Management and Neurologic Outcomes: An Evidence. Based Appraisal of Current Practices Hogue, Charles W. Jr; Palin, Christopher A. ; Arrowsmith, Joseph E. Anesthesia & Analgesia. 103(1): 21 -37, July 2006. doi: 10. 1213/01. ANE. 0000220035. 82989. 79 Figure 3. Epiaortic ultrasound images and pathologic specimen depicting atherosclerosis of the ascending aorta. Transverse (panel A) and longitudinal (panel C) ultrasound scans demonstrate circumferential intimal thickening particularly anteriorly (arrows). Pathologic specimen (panel B) confirms the diagnosis. Transverse (panel D) and longitudinal (panel F) images from a second patient demonstrate intimal thickening (small arrows) and large sessile atheroma confirmed with the pathologic specimen (panel E). The pathologic specimens were made available when the patients underwent replacement of the ascending aorta. Reprinted with permission from Dávila-Román et al. (73). Copyright © 2015 International Anesthesia Research Society. Published by Lippincott Williams & Wilkins. 19
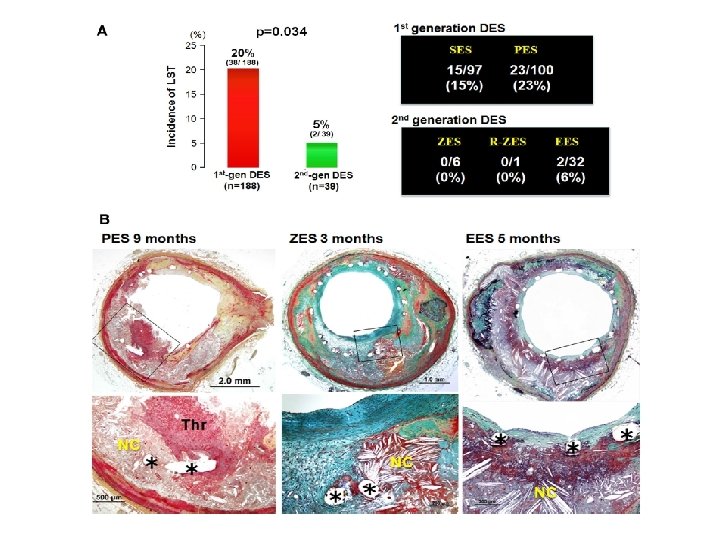
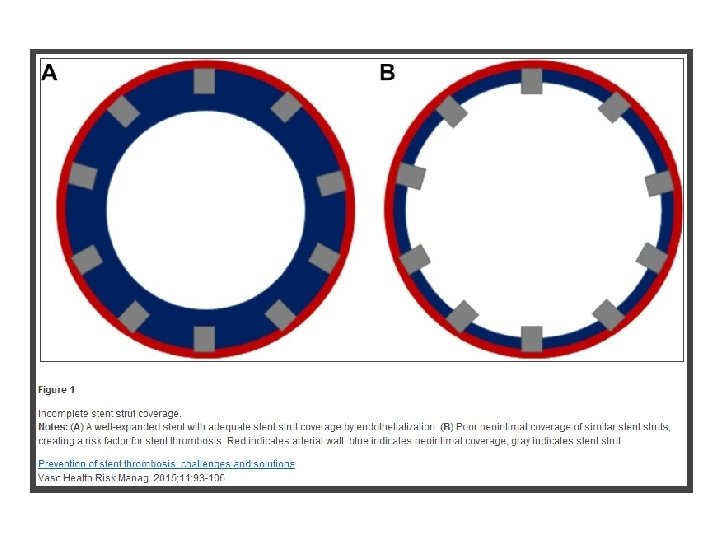
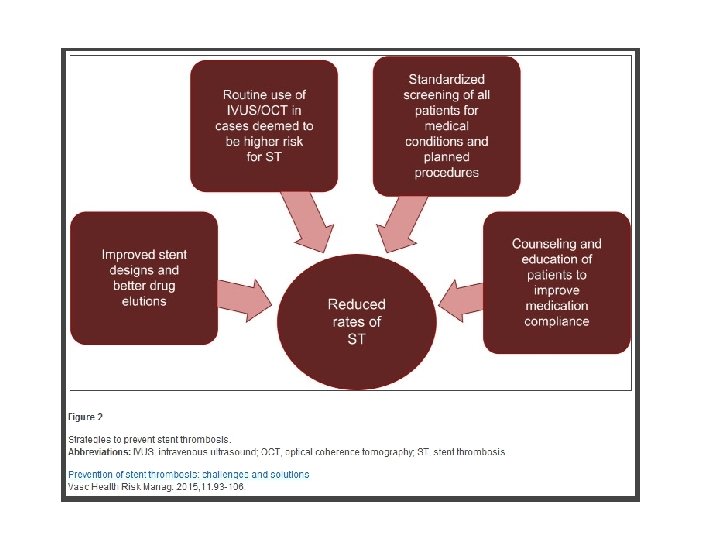
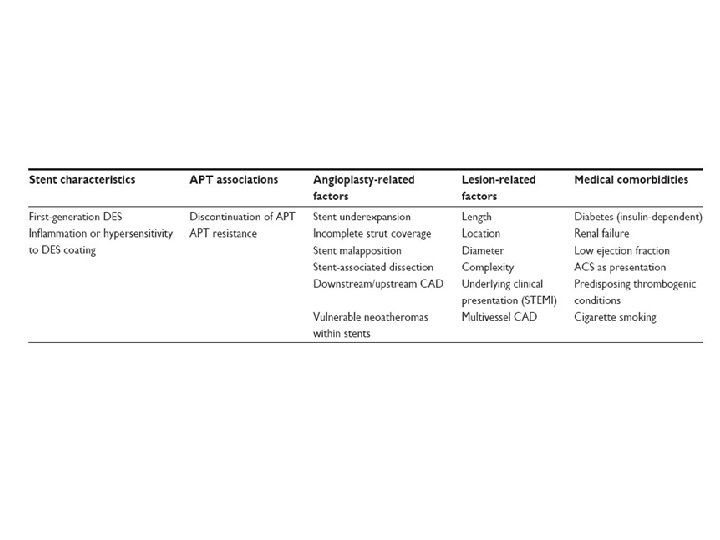
PCI Procedural Risks • Bleeding • Stent thrombosis
From: A Randomized Controlled Trial in Second-Generation Zotarolimus-Eluting Resolute Stents Versus Everolimus-Eluting Xience V Stents in Real-World Patients: The TWENTE Trial J Am Coll Cardiol. 2012; 59(15): 1350 -1361. doi: 10. 1016/j. jacc. 2012. 01. 008 Figure Legend: Cumulative Incidence of Definite or Probable Stent Thrombosis *Cardiac death; patient enrolled for stenting of residual lesions in right and left anterior descending arteries 7 days after a non–STsegment elevation myocardial infarction, treated with a bare-metal stent in circumflex artery. †Target vessel revascularization; patient was not receiving dual antiplatelet therapy because of intolerance to acetylsalicylic acid (patient used clopidogrel and oral anticoagulation). ‡Cardiac death; patient did not adhere to prescribed dual antiplatelet therapy (used acetylsalicylic acid only). §Non Date of download: © The American Collegetherapy of Cardiology. –Q-wave myocardial infarction; patient Copyright was not receiving dual antiplatelet (used clopidogrel and oral anticoagulation). 5/15/2015 All rights reserved.
FIGURE 3. The scattered plot for the fractional flow reserve (FFR) and angiographic diameter stenosis (a) [unpublished data] and the FFR and minimal lumen area assessed by intravascular ultrasound (b) [32[black small square]]. Should we be using fractional flow reserve more routinely to select stable coronary patients for percutaneous coronary intervention? . Park, Seung-Jung; Ahn, Jung-Min Current Opinion in Cardiology. 27(6): 675 -681, November 2012. DOI: 10. 1097/HCO. 0 b 013 e 328358 f 587 © 2012 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
From: Percutaneous Coronary Intervention Versus Coronary Artery Bypass Graft Surgery in Left Main Coronary Artery Disease: A Meta-Analysis of Randomized Clinical Data J Am Coll Cardiol. 2011; 58(14): 1426 -1432. doi: 10. 1016/j. jacc. 2011. 07. 005 Figure Legend: Effect of PCI on Death, MI, Stroke, and Repeat Revascularization Pooled odds ratios are from fixed and random models. Abbreviations as in Figures 1 and 2. Date of download: 5/15/2015 Copyright © The American College of Cardiology. All rights reserved.
Rates of Outcomes among the Study Patients, According to Treatment Group. The SYNTAX Trial Serruys PW et al. N Engl J Med 2009; 360: 961 -972.
• The risk of repeat revascularization after PCI needs to be balanced against the invasiveness of CABG and the risk of stroke, as previously reported in a meta-analysis of 23 studies comparing CABG and PCI, in which procedure-related strokes were found to be more common after CABG (in 1. 2% of patients, vs. 0. 6% of those undergoing PCI; P<0. 001), without a concomitant decrease in survival • Aortic manipulation releases embolic material, thereby enhancing the probability of adverse neurologic outcomes following coronary artery bypass grafting (CABG). Single aortic clamping in coronary artery bypass surgery reduces cerebral embolism and improves neurocognitive outcomes Hrvoje Gasparovic, Vascular Medicine 18(5) 275– 281