Coronary Perforation in CTO Revascularization Management Issues David



 Technique • Prolonged")
















- Slides: 65
Coronary Perforation in CTO Revascularization Management Issues David E. Kandzari, MD, FACC, FSCAI david. kandzari@piedmont. org Director, Interventional Cardiology, Piedmont Heart Institute Chief Scientific Officer, Piedmont Heart Institute Atlanta, Georgia
Disclosure Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below Affiliation/Financial Relationship Company Grant/Research Support Abbott Vascular, Cordis Corporation, Medtronic Cardio. Vascular Consulting Fees/Honoraria Abbott Vascular, Cordis Corporation, Medtronic Cardio. Vascular, Micell Technologies Major Stock Shareholder/Equity None Royalty Income None Ownership/Founder None Intellectual Property Rights None Other Financial Benefit None
Coronary Perforation In CTO Revascularization Often does not occur at the occluded segment nor is related to the guidewire… 12% CTO-related perforations due to balloon inflation, stent implantation, or atherectomy 1 Is not always manifest during the procedure… 45% events diagnosed after leaving the catheterization laboratory (mean time from PCI 4. 4 hrs)2 Is associated with substantial morbidity and mortality… Death (42%), emergency surgery (39%), MI (29%), transfusion (65%)2 1 Nakamura et al. AHA 2002, 2 Fejka, O’Neill et al. AJC 2002
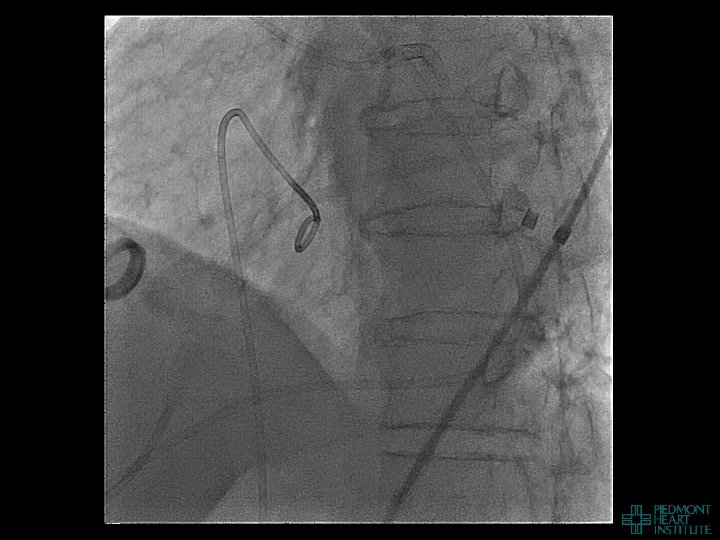
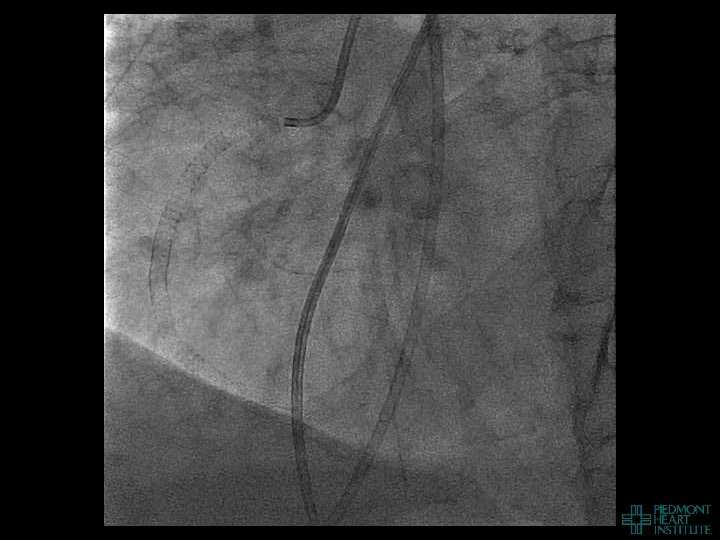
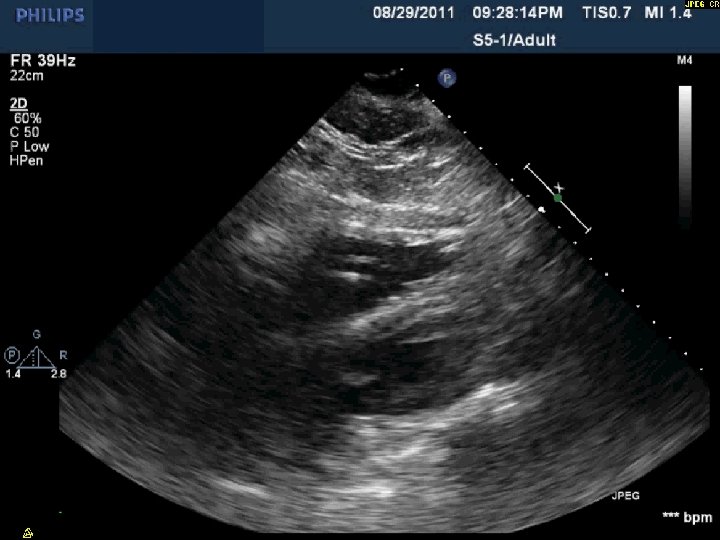
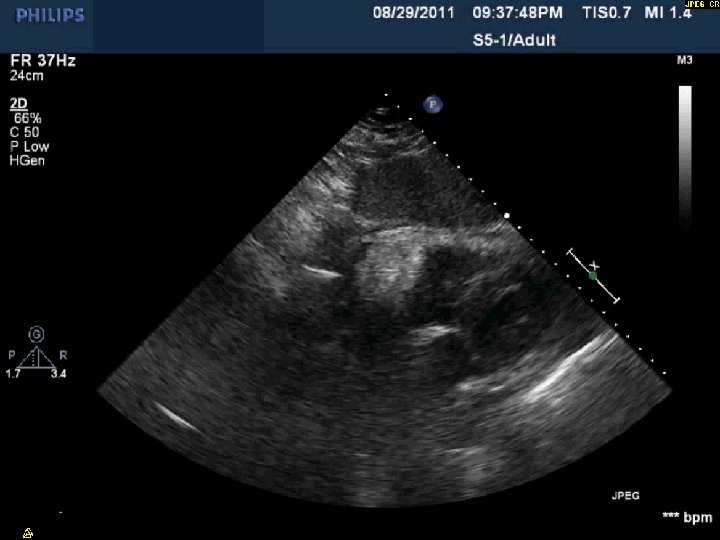
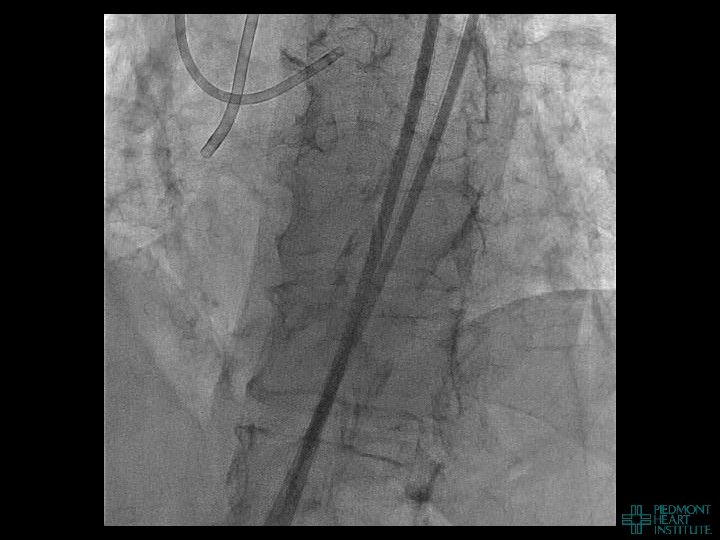
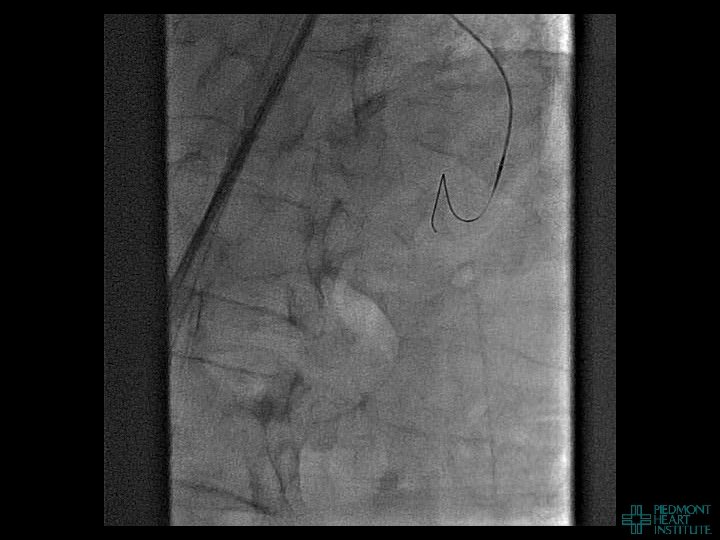
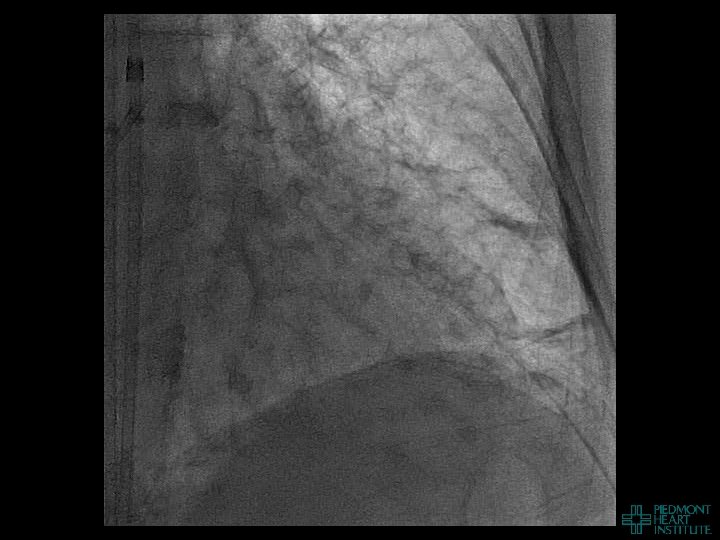
Coronary Perforation Methods of Patient Management • Dual Catheter (‘Ping Pong’) Technique • Prolonged balloon inflation and covered stents • Reversal of anticoagulation — Know contradictions to protamine sulfate for UFH; Avoid bivalirudin, LMWH — Reserve GP 2 b 3 a inhibition until successful crossing and wire change-out Embolization • — Coil, gelfoam, methacrylate, autologous blood/fat • Microcatheter Occlusion • Confirmation of successful management — Contralateral injection — Right heart catheterization — Echocardiogram — Contrast echocardiography
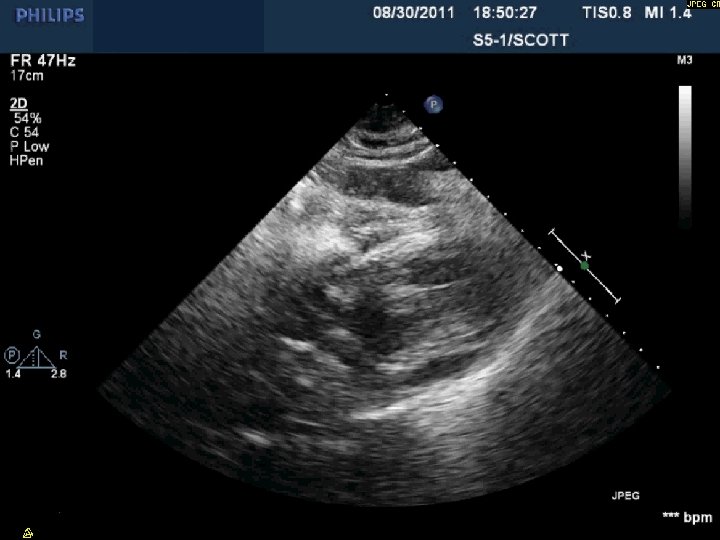
Day 2 No further pericardial drainage, echo without effusion…pericardial catheter pulled Day 3 Enoxaparin for DVT prophylaxis initiated 8 hours later, PEA arrest Echo shows recurrence of effusion and tamponade physiology
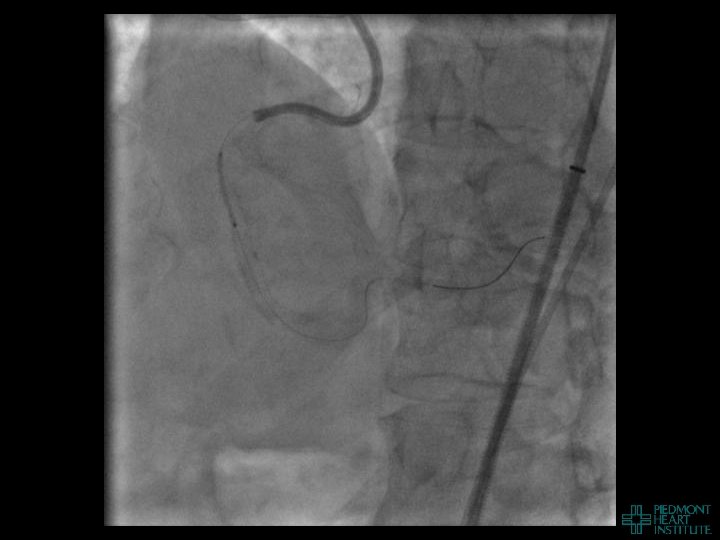
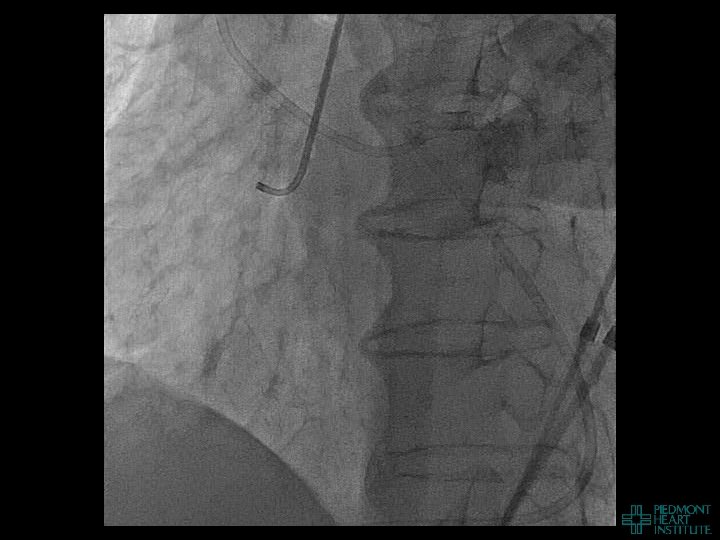
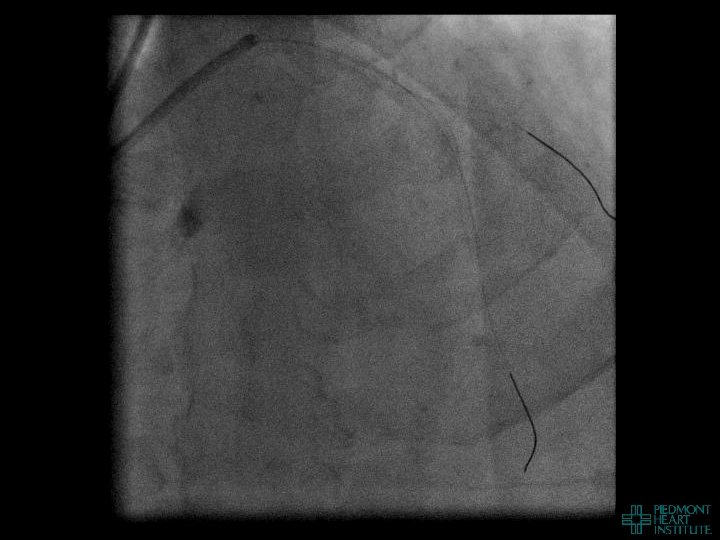
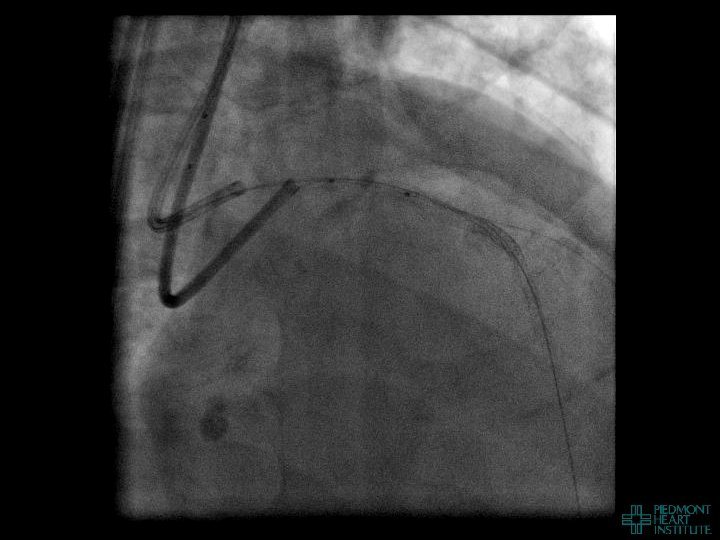
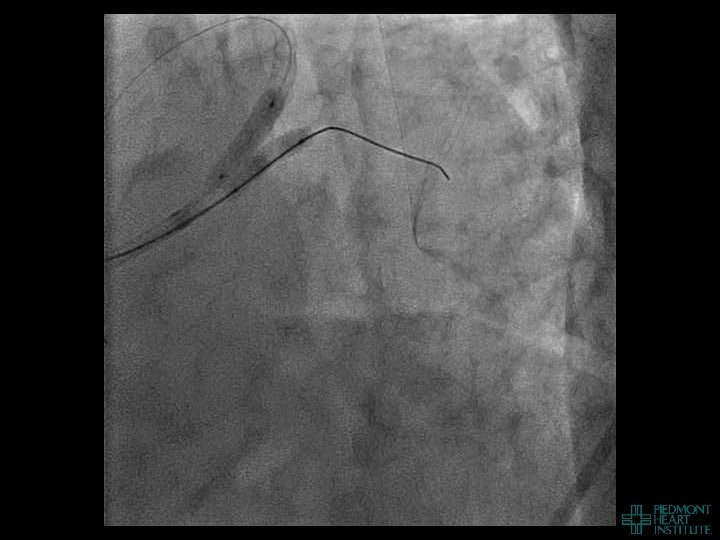
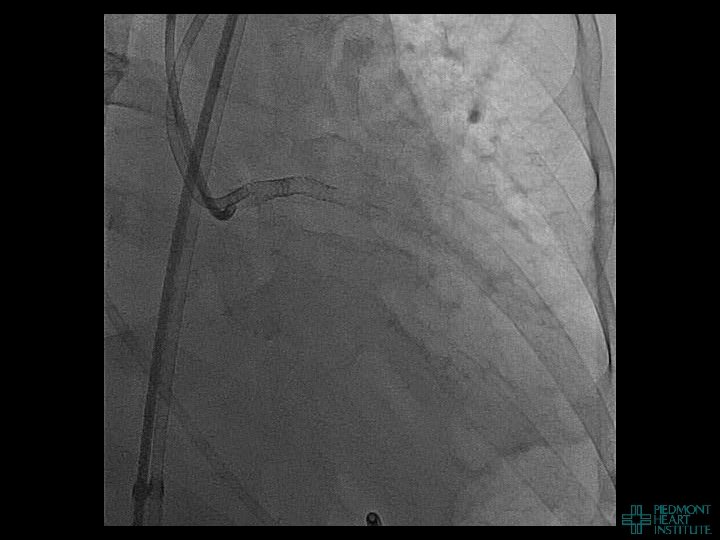
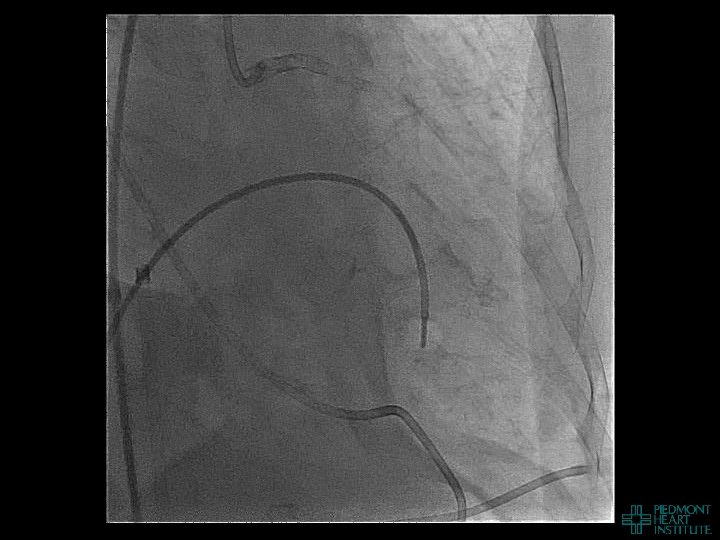
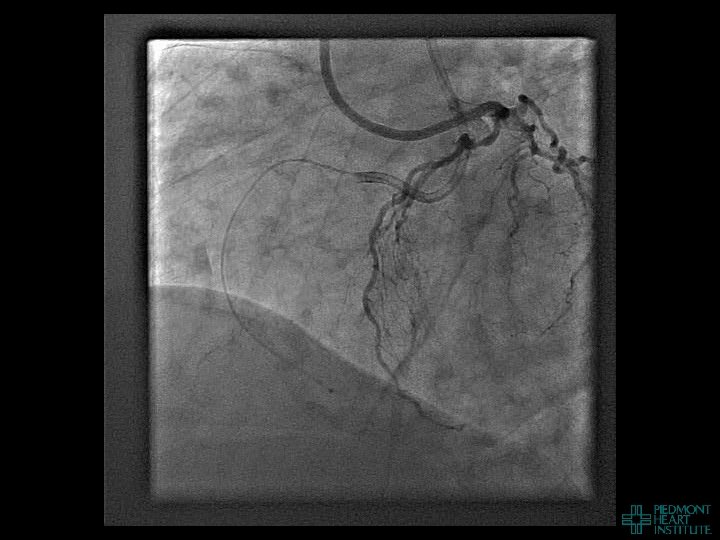
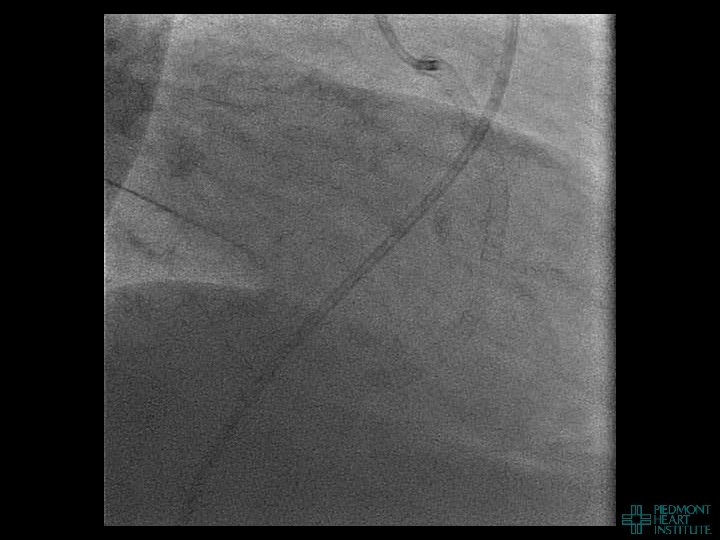
Case Example 2
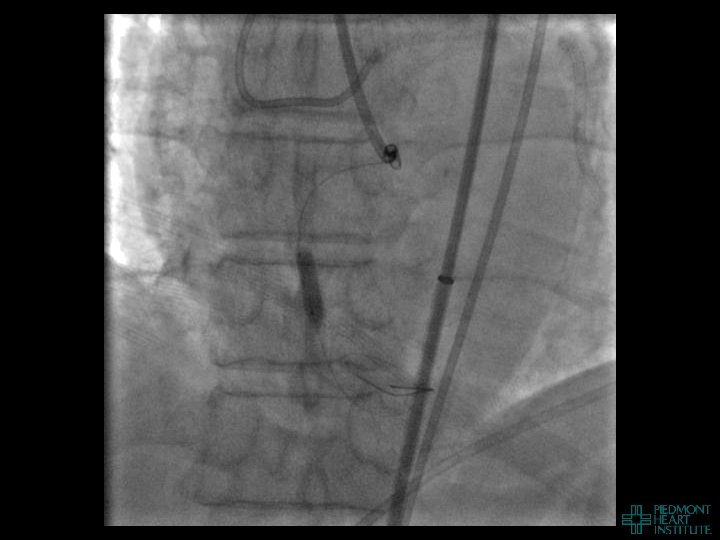
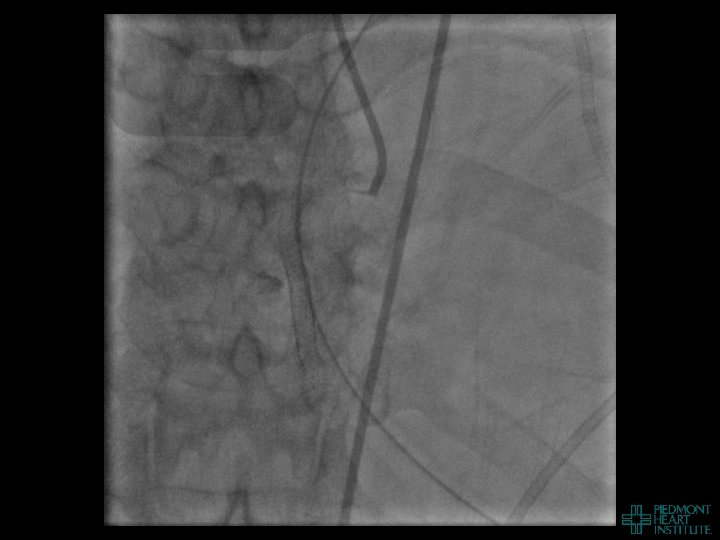
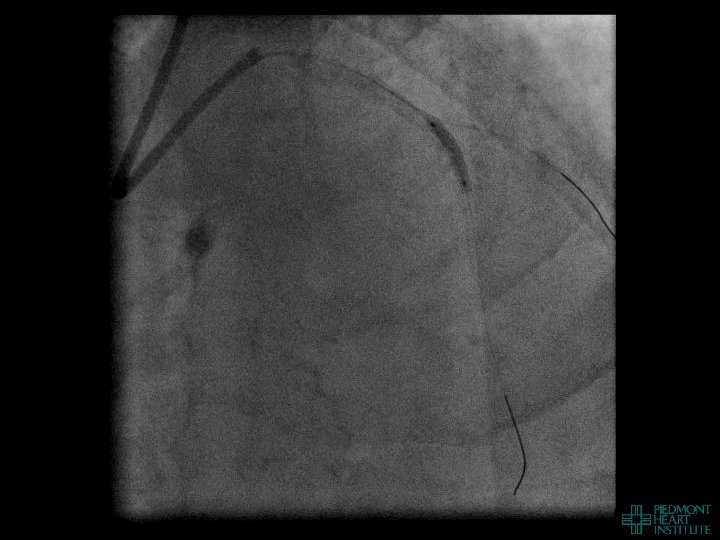
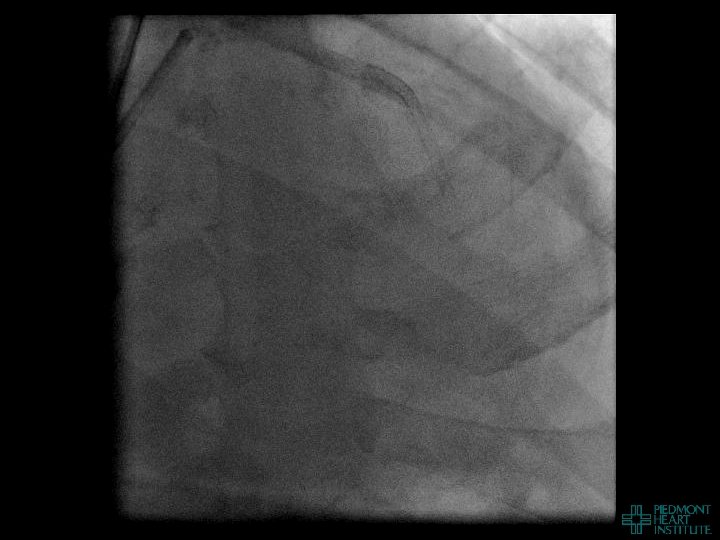
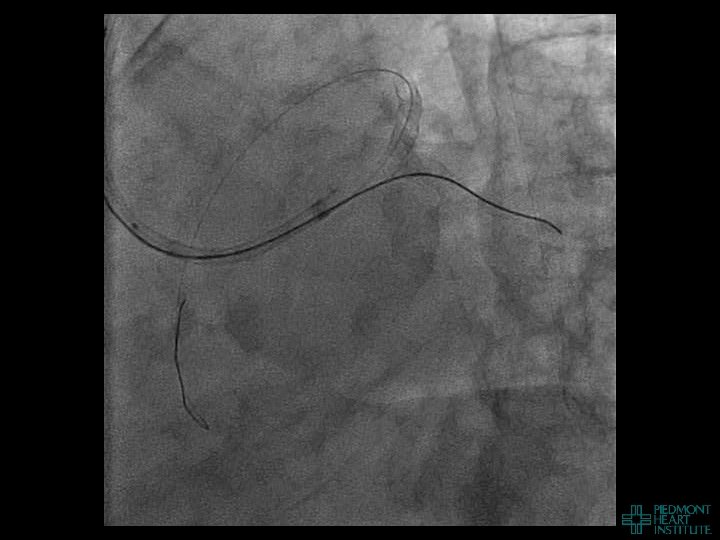
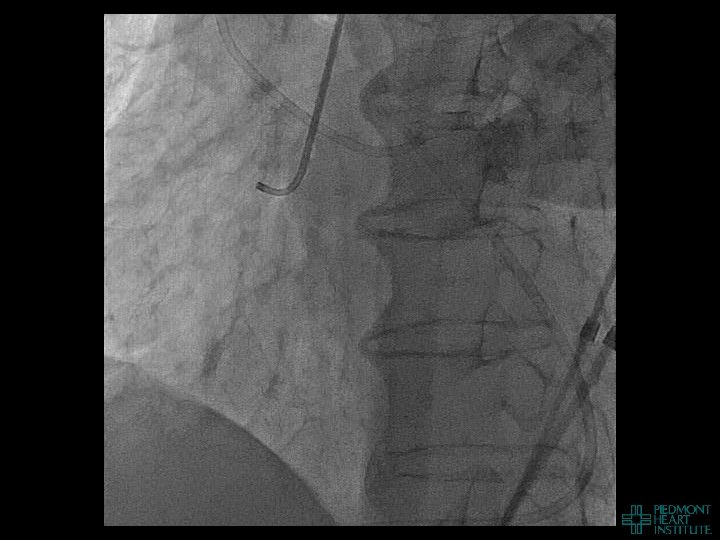
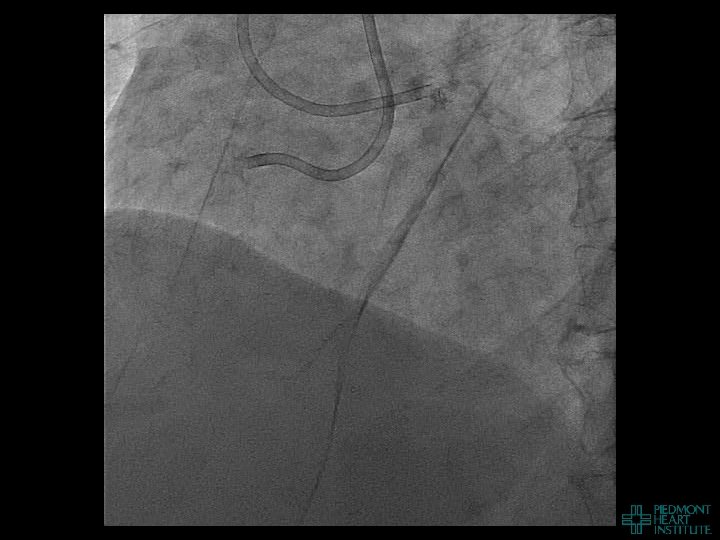
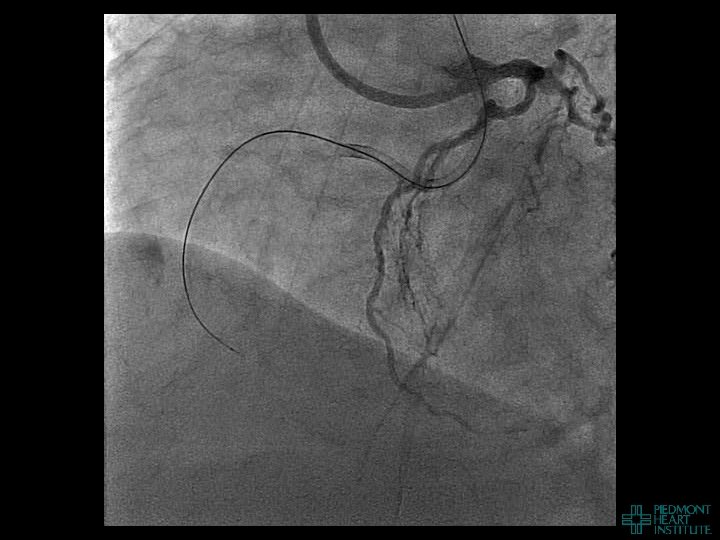
Case Example 3
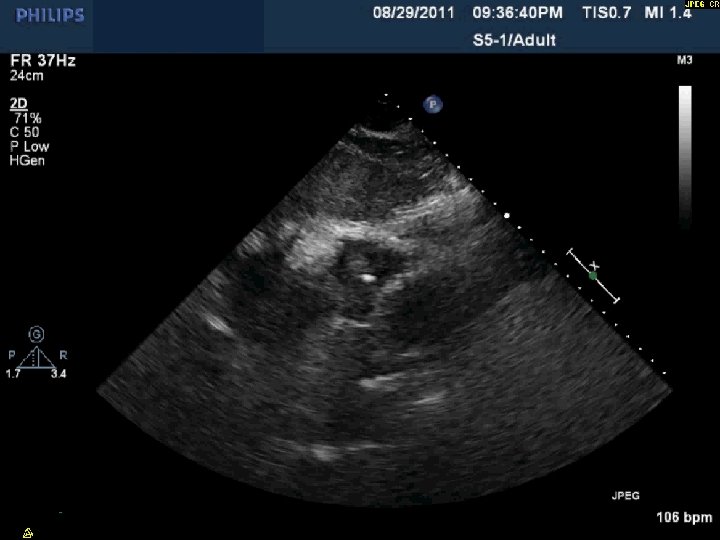
Day 2 Stable overnight No further pericardial drainage Echo shows no recurrence of effusion In ICU, pericardial pigtail catheter pulled…. . Within 5 minutes, systolic blood pressure drops to <80 and bedside echo confirms recurrence of effusion Emergency pericardiocentesis draws off 650 cc immediately followed by continuous drainage of blood
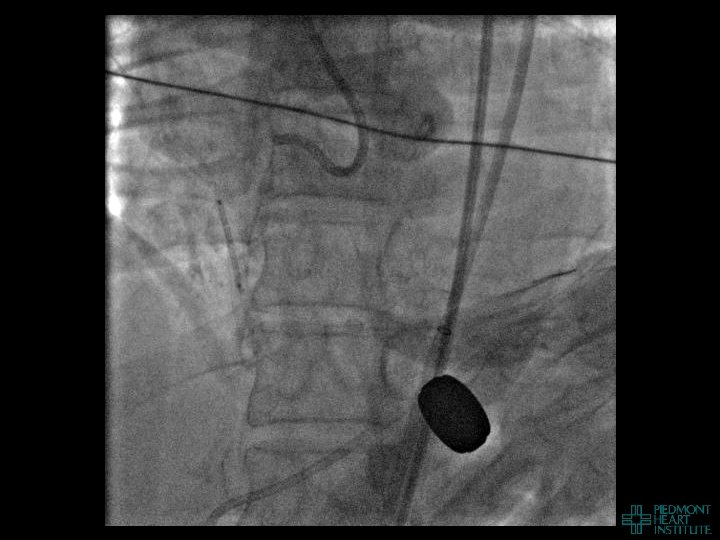
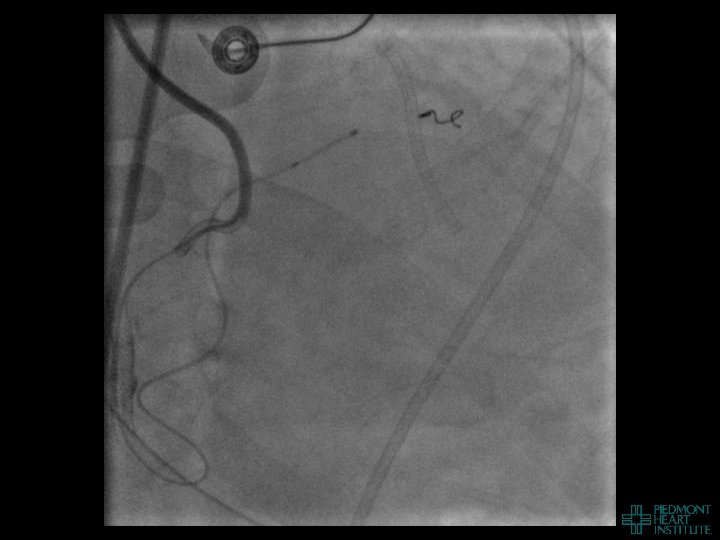
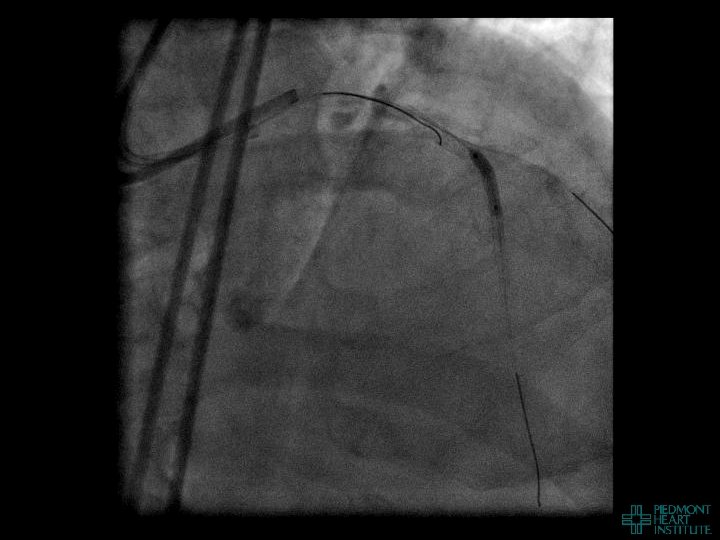
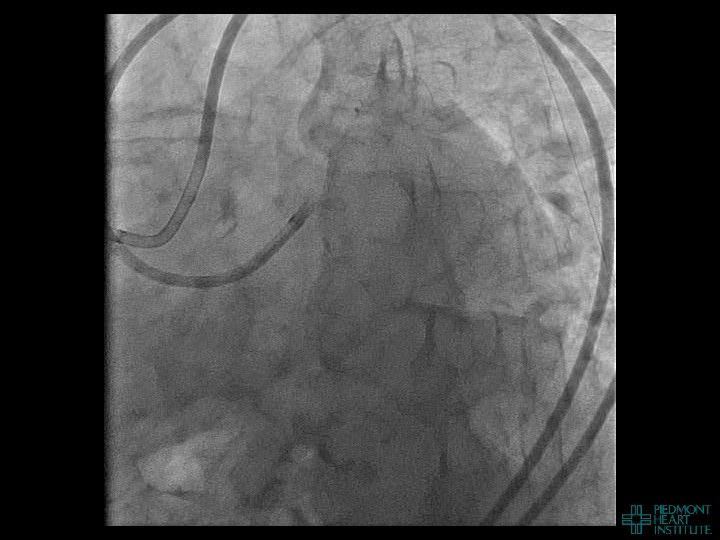
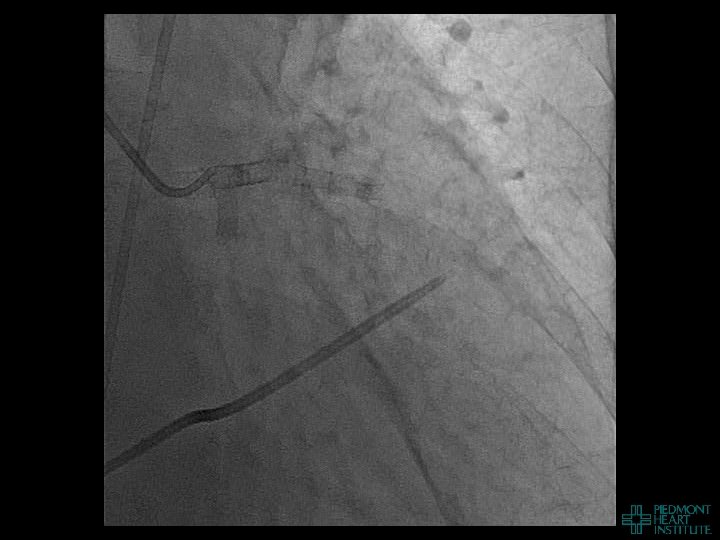
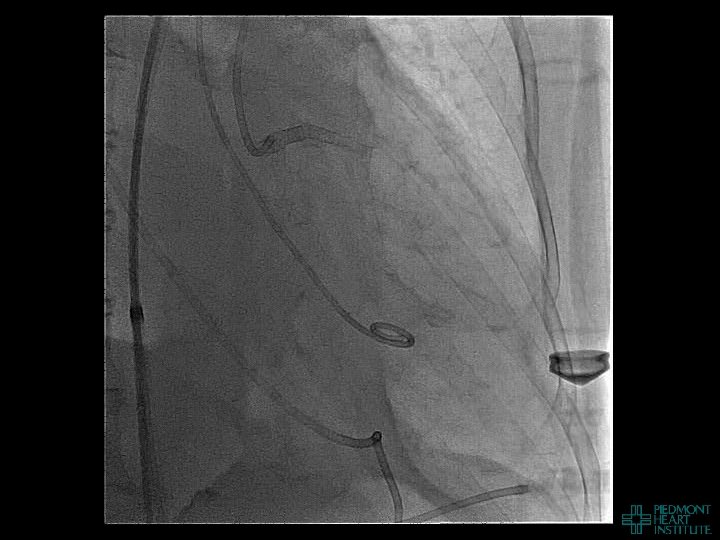
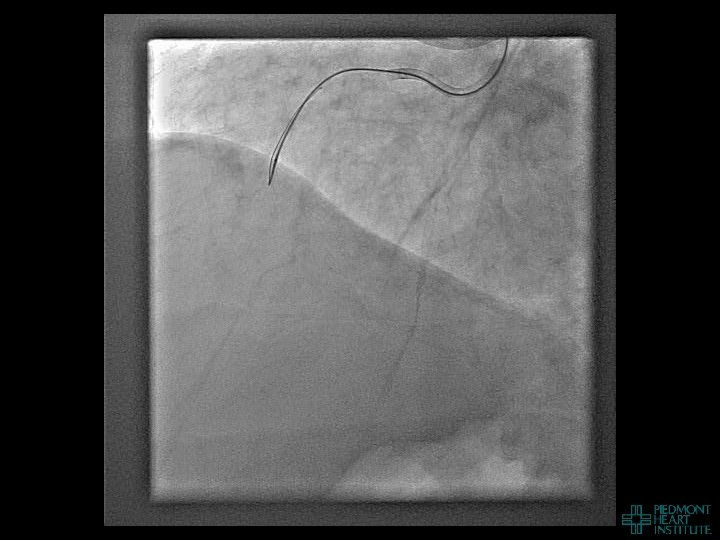
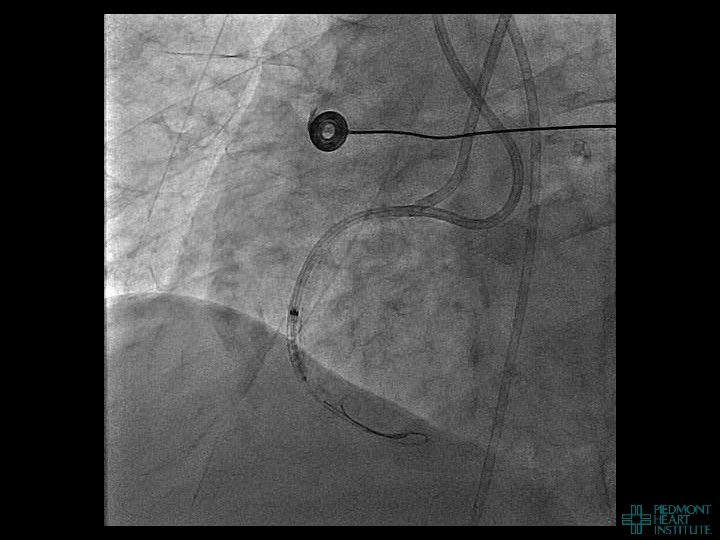
Case Example 4
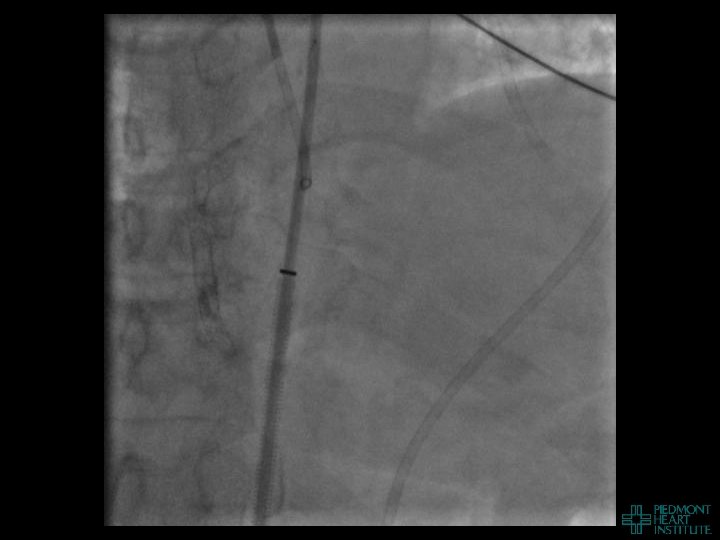
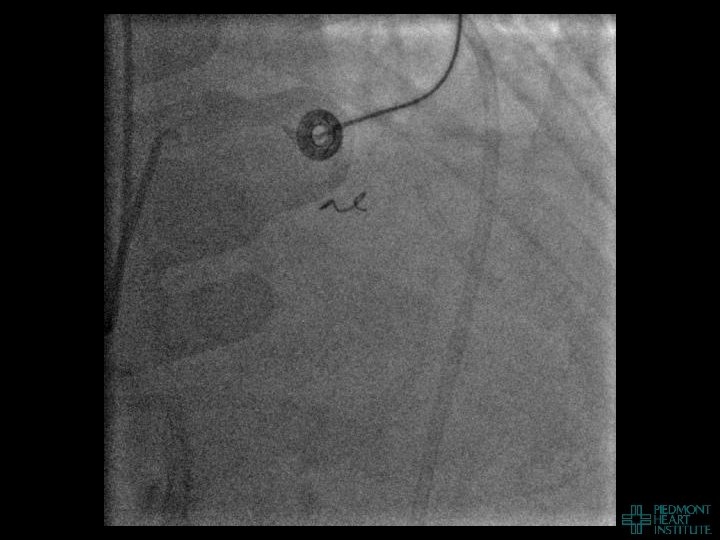
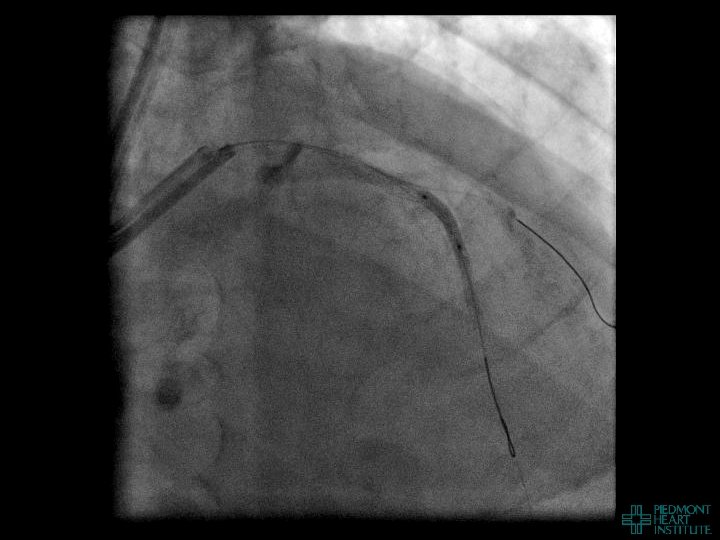
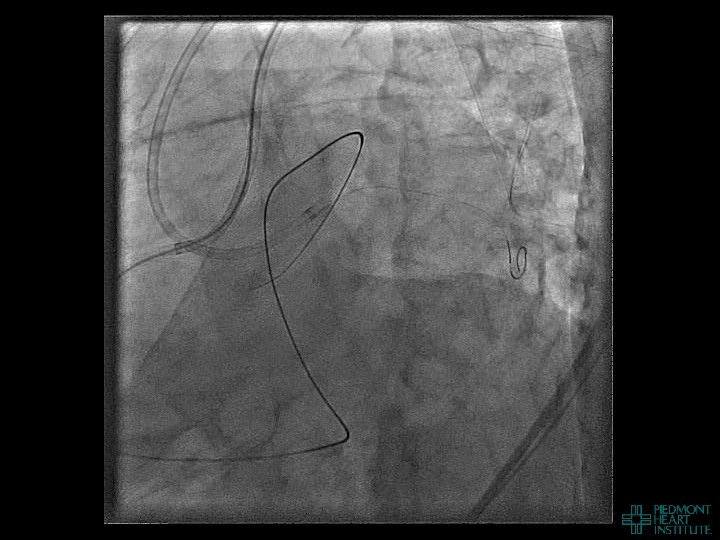
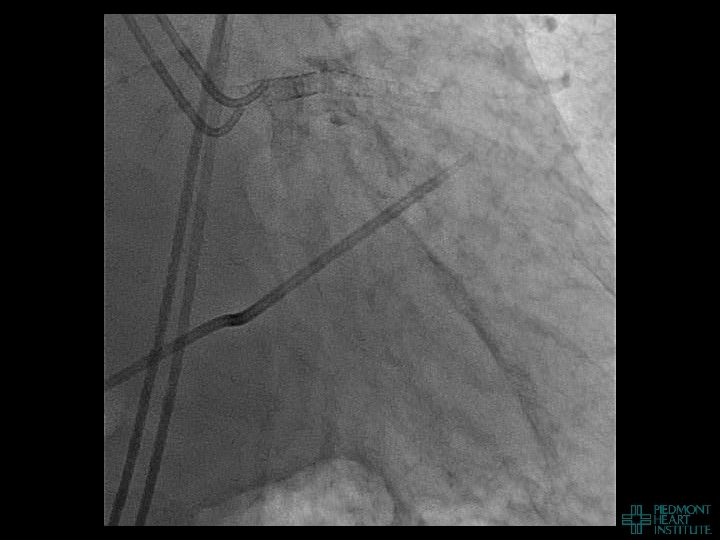
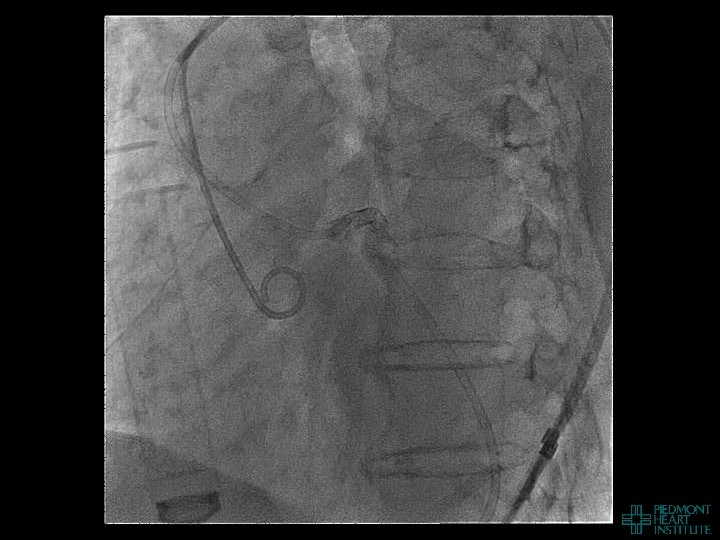
Case Example 5