Coronary Artery Bypass Grafting in Cardiac Failure Dr

Coronary Artery Bypass Grafting in Cardiac Failure Dr. Johan van der Merwe Registrar University of Pretoria

Introduction

n USA statistics 385 000 new cases per year 159 percent increase in hospitalization rate since 1993 ¨ Severe economic implication (1997 report) th er ca us e s ¨ ¨ O n n n 40 -70% = Ischemic CMO n Terminal disease ¨ ¨ ¨ n Causes of cardiomyopathy $5, 501 was spent for every hospital-discharge diagnosis $1, 742 per month was required to care for each patient after discharge Annual total cost of $4. 5 billion 1 year mortality 20% 5 year mortality 45 -60% 10 year survival rare 45% of transplant recipients

Relevant coronary anatomy n Left system n Right system

Natural progression of ischemic cardiomyopathy
 n 0 -30 minutes = reversible Mitochondrial swelling and cristae distortion")
Initial infarct (immediate) n 0 -30 minutes = reversible Mitochondrial swelling and cristae distortion ¨ Relaxation of myofibrils ¨ n After 60 minutes = irreversible Sarcolemma disrupts ¨ Margination of chromatin ¨ Mitochondrial degeneration ¨
 n n n 4 -12 hours: coagulative necrosis")
Expansion of infarct (hours to days) n n n 4 -12 hours: coagulative necrosis and inflammatory process 3 -10 days: disintegration and resorbtion of myofibrils and fibrovascular response Acute loss of myocardial cells results in abnormal loading conditions that involve not only the border zone of the infarction, but also remote myocardium.
 n n 7 th week:")
Scarring and Global remodelling (7 th week to months) n n 7 th week: scarring complete and remodelling continues for months after the initial insult Laplace’s law ¨ n Wall tension = Pressure x radius / 2 x wall thickness These abnormal loading conditions induce hypertrophy, then dilatation and spherical shape change of the ventricle

Typical patient presentation CHF with multi-organ ¨ dysfunction ¨ Abnormal left ventricular function n n n ¨ Abnormal septal function n n ¨ Decreased contractility Lvedd > 5. 1 cm LVesd > 4 cm EF < 35% LVPW < 0. 9 cm Aneurysm IVSd < 0. 9 Septal defect Abnormal Right Ventricular function

Goals and objectives for revascularization in ischemic cardiomyopathy

Revascularize anatomically graftable vessels n Reperfuse stunned or hibernating myocardium that will recover n Prevent progression of disease n Balance high risk and mortality with a too conservative approach passing over patients who can benefit from surgery n

Patient Selection Criteria Is the pathology operable?
 Coronary")
Anatomical Indications n n Veteran’s Affairs Cooperative Study of coronary bypass surgery (VACS) Coronary Artery Surgery Study (CASS)

Contractility assessment n n Segmental analysis 3 descriptions of myocardial movement ¨ Hypokinesia n ¨ Akinesia n ¨ Functional segment, but contractility decreased Non-functional segment, no contractility Dyskinesia n Non-functional segment, movement paradoxically

Hypokinetic or akinetic ischemic myocardium n Stunned myocardium ¨ myocardial contractile dysfunction that follows a period of transient ischemia (coronary occlusion), even after flow has been restored to an area that has no irreversible damage ¨ represents a flow-contraction mismatch ¨ appear perfused on nuclear imaging exams, but will demonstrate wall motion abnormalities ¨ may persist for a few days to 8 weeks after revascularization without further intervention n Hibernating myocardium ¨ viable myocardium with depressed resting flow and reduced resting function ¨ Chronic decrease in blood supply (chronic ischemia) ¨ adaptive response to ischemia but with progressive cellular degeneration over time n Scar Tissue ¨ Transmural ¨ Non-transmural

Chronic stable angina n n Class 1 ¨ Left mainstem > 50% stenosis ¨ Left main equivalent ¨ 3 vessel disease with EF <50% ¨ 2 vessel with proximal LAD with EF < 50% and objective ischemic changes ¨ 1 or 2 vessel disease with large area of myocardium at risk ¨ Disabling angina despite optimal medical therapy when surgery can be performed at low risk Class 2 a ¨ Proximal LAD without large area at risk ¨ 1 or 2 vessel disease (not LAD) with moderate area at risk Class 2 b ¨ Borderline stenosis (50 -60% other than LAD) with demonstrable ischemia despite optimal medical therapy Class 3 ¨ Other than LAD with small area at risk ¨ Stenos 50 -60% in other that left mainstem without ischemia ¨ Stenosis > 50% SAME INDICATIONS FOR ASYMPTOMATIC CAD

Acute coronary syndrome n Non Q-wave ¨ Acute < 12 hours n ¨ Sub-acute n n Class 1 = Ongoing ischemia despite optimal medical therapy Class 1 = Same as for chronic stable angina Q-wave ¨ Acute <12 hours n n ¨ Class 1 = None Class 2 = Ongoing ischemia, cardiogenic shock after failed thrombolysis / PCI Sub-acute n Same as for chronic stable angina n Progressive failure with stenosis compromising viable myocardium outside the initial infarct n Class 3 ¨ CABG without attempts at maximal medical therapy

Complications of PCI n Class 1 Ongoing ischemia with significant myocardium at risk ¨ Hemodynamic compromise ¨ Rupture with impending tamponade ¨ n Class 2 a Foreign body in in crucial anatomical position ¨ Hemodynamic compromise with coagulation impairment and without previous sternotomy ¨ n Class 2 b ¨ n Hemodynamic compromise with coagulation impairment and with previous sternotomy Class 3 ¨ Stable with unsuitable anatomy

Trauma n n n Class 2 a ¨ Demonstrable proximal injury with demonstrable ischemia Class 2 b ¨ No evidence of ischemia ¨ Distal injury with ischemia Class 3 ¨ Distal injury with no ischemia Kawasaki n n n Class 2 a ¨ Demonstrable ischemia + stenosis + viable myocardium + graftable arteries Class 2 b ¨ Asymptomatic giant coronary artery aneurysms subtending a large area at risk (>8 mm) Class 3 ¨ Small (<8 mm) asymptomatic aneurysms without stenosis

Physiological Indication n Determining myocardial viability ¨ Wijns, Vatner, Camici. I (NEJM, Volume 339 nr 3) n n n Post-operative improvement in LVEF (also symptoms) is related to the preoperative identification of viable myocardial tissue Viability involving 18% or more of the LV myocardium have been shown to have the greatest improvement in functional status In a meta-analysis ¨ ¨ Patients with predominantly viable myocardium who underwent revascularization had an 80% lower mortality rate and a cardiac event rate than those treated medically No difference in cardiac death rate was seen in patients with predominantly non-viable myocardium who underwent revascularization versus medical therapy (7. 7% versus 6. 2%, respectively).

TECHNIQUES TO PREDICT FUNCTIONAL RECOVERY AFTER REVASCULARIZATION IN PATIENTS WITH LEFT VENTRICULAR DYSFUNCTION DUE TO CHRONIC CORONARY ARTERY DISEASE. TECHNIQUE SENSITIVITY SPECIFICITY PATIENTS STUDIES Technetium 99 m Sestamibi Imaging 83 (78– 87) 69 (63– 74) 207 10 Dobutamine echocardiography 84 (82– 86) 81 (79– 84) 448 16 Thallium-201 stress– redistribution imaging 86 (83– 89) 81 (79– 84) 209 7 18 F fluorodeoxyglucose PET imaging 88 (84– 91) 81 (79– 84) 327 12 Thallium-201 rest Redistribution imaging 90 (87– 93) 81 (79– 84) 145 8
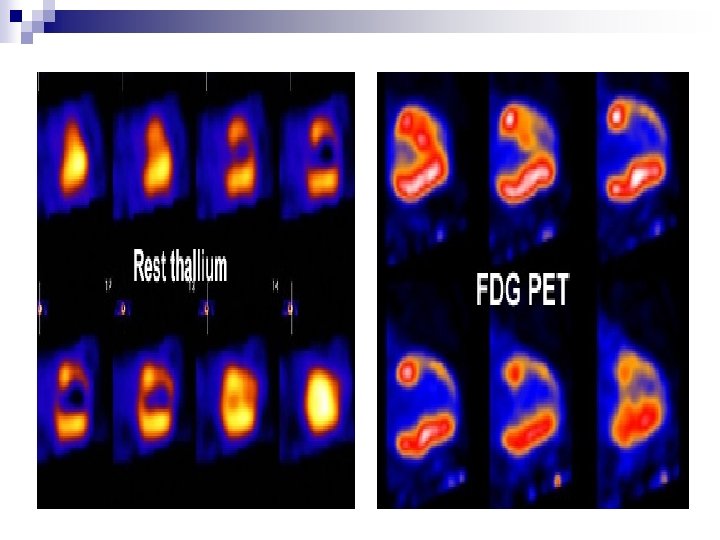

Thallium Cardiac Imaging n Clinical Applications ¨ Detection of coronary artery disease n Angiographically defined coronary artery disease does not necessarily correlate with necropsy data n Thallium imaging provides physiologic information regarding the impact a specific stenosis has on tissue perfusion ¨ Evaluation of the extent and severity of coronary stenosis

Technetium Labelled Cardiac Imaging
 study ¨ Compared difference in cost in 11372 patients")
Economics of Non-invasive Diagnostics (END) study ¨ Compared difference in cost in 11372 patients referred for either stress MPI (myocardial perfusion imaging) or cardiac catheterization as initial approach ¨ Conclusions Rates of subsequent infarction similar n MPI much cheaper, less subsequent surgical interventions n ¨ Revision of protocols to be expected
")
MR Imaging for Hibernating Myocardium n Main application is hyper-enhancement studies (demonstrates scar tissue) to predict functional recovery ¨ Gadolinium is retained by scar tissue ¨ Segments demonstrating 51 -75% scar tissue = only 10% will demonstrate functional recovery with revascularization ¨ Segments < 25% of the wall thickness = more likely to recover function following revascularization n Sensitivity 55% in predicting improvement in function in a myocardial segment after revascularization

Patient Selection Criteria Is the patient operable?

Full multi-disciplinary work-up n Risk factor identification n Medical optimization n

Patient Selection Criteria Will the patient benefit?

The bad news…. . n Known increase in morbidity and mortality following CABG with LV-dysfunction ¨ CABG patch trail ¨ Should we revascularize occluded coronary arteries in cardiovascular shock trail (SHOCK) n EF < 20% compared to normal EF ¨ 4 x increase risk for cardiogenic shock post surgery ¨ 50% higher mortality

The good news…. . n n Veteran’s Affairs Cooperative Study of coronary bypass surgery (VACS) Coronary Artery Surgery Study (CASS) Studies of Left Ventricular Dysfunction (SOLVD) Findings ¨ Clear survival benefit for patients with impaired LVfunction undergoing surgery versus optimal medical management ¨ Decrease risk of sudden death
 Main authors 19651975")
The evidence summarized…. Year Number of Studies Patient Numbers EF (%) Main authors 19651975 6 386 <25% Vlietsra, Manley, Yatteau, Oldham, Zubaite, Faulkner 19751980 7 384 <20% Fox, Jones, Alderman, Mochtar, Zubiate, Hochberg, Sanchez 19801990 13 1819 <20% Kron, Blakeman, Wong, Christaki, Hammermeister, Louie, Milano, Shapira, Anderson, Hausman, Kaul, Mickleborough, 19901995 9 1507 <35% Langeberg, Elefteraides, Kawachi, Moshkovitz, Baumgartner, Cimochowski, De. Carlo, Luciani

Peri-operative mortality 3 -5 year mortality

Improvement in EF after revascularization n 5 studies ¨ n n Average interval of 6 months Increase in EF by 8 – 12% 60 -70% of patients with good result P-value < 0. 001 – 0. 05 Improvement in regional wall motion seen after 2 to 3 weeks

Timing of revascularization
 ¨ Performed a")
n Daniel C. Lee (J Thorac Cardiovasc Surg 2003; 125: 11520) ¨ Performed a retrospective multicenter analysis ¨ 32, 099 patients who underwent coronary artery bypass grafting as the sole procedure after transmural myocardial infarction between 1991 and 1996 ¨ 179 surgeons at 33 hospitals in New York State. ¨ Overall hospital mortality for all patients was 3. 3%. ¨ Hospital mortality decreased with increasing time interval between revascularization and transmural acute myocardial infarction n Less than 6 hours = 14. 2% mortality n 6 -24 hours = 13. 8% n 24 -72 hours = 7. 9%, n 4 – 7 days = 3. 8%, n 7 to 14 days = 2. 9%, n After 15 days = 2. 7%

Conclusion n In the absence of absolute indications for emergency surgical intervention, such as structural complications and ongoing ischemia n 3 -day waiting period as a minimum before surgical revascularization should be considered n Less than 3% mortality after 2 weeks

Additional challenges……. . n n REDO-CABG with CHF CABG in concomitant ischemic mitral regurgitation CABG in concomitant post infarction VSD CABG + Ventricular reconstruction

REDO-CABG with CHF

Mortality rate 4. 7 to 7. 2% n Careful planning essential n ¨ Sternal entry ¨ Aortic atherosclerosis ¨ Atherosclerotic vein grafts ¨ Diffuse native vessel disease ¨ Lack of conduits ¨ Myocardial protection

CABG in concomitant ischemic mitral regurgitation Presence of MR increases operative mortality for CABG alone by 3 -12% ¨ CABG + MR: > 10% operative mortality ¨
 n n ¨ Moderate (3+) n ¨ CABG")
Overall recommendations ¨ Severe MR (4+) n n ¨ Moderate (3+) n ¨ CABG + Repair Replace if intra-operative failure CABG + Repair unless ¨ Additional operative morbidity / mortality would be prohibitive ¨ OPCAB Mild (2+) n Repair if ¨ Morbidity / mortality low ¨ Investigations show periods of more severe MR ¨ Confirmation during intra-operative TEE

n n n CABG alone ¨ Balu, Christenson, Tolis ¨ Can decrease MR severity (especially mild with poor LVF) ¨ Weak impact on moderate MR leaving many patients with 2+ or greater RMR ¨ Emory group n Moderate RMR no effect on long term functional status or survival CABG + mitral surgery ¨ Prifti, Harris ¨ CABG + MV-repair improve late outcome (especially LVF) Residual MR after CABG/Repair ¨ Oppell, Czer ¨ 65% 3 year survival ¨ Suture annuloplasty: Failure to decrease MR-severity in 33% of patients ¨ Ring/band annuloplasty: 2+ grade decrease in 97% of patients

CABG in concomitant post infarction VSD

n n n Alvarez, Dagget, Deville ¨ CABG may increase early and longterm survival ¨ Recommendation n If stable enough => Catheterization + CABG n If not => selective left heart catheterization and proceed with septal repair Value of pre-operative angiogram and revascularization is controversial ¨ No additional benefit ¨ Time-consuming ¨ Dangerous Possible role of CT-Angiography?

CABG + Ventricular reconstruction

n Cleveland ¨ 85% concomitant CABG and 43% concomitant MVR in reconstruction procedures ¨ Survival at 30 days, 1, 2 and 3 years was 98%, 92%, 90%, and 86% n Goal ¨ Incision into anterior wall scar tissue (LAD distribution) to exclude pathological segment and to reduce LVcavity size n Indications ¨ Dyskinetic segment ¨ Electrophysiologically proven source of arryhtmia ¨ Thrombus

What about therapeutic angiogenesis and laser revascularization? n. Stimulate angiogenesis through inflammation induction n. Limited roll at present

Conclusion

n n n CABG remains the definitive management for ischemic cardiomyopathy in conjunction with optimal medical management Although these patients are at higher risk, outcome have improved and is now acceptable ¨ Clear survival benefit ¨ Clear improvement in quality of live Myocardial viability assessment forms the cornerstone of surgical decision making and new studies challenge current protocols which require revision

Summary…… Minimum criteria for CABG in ischemic CMO ¨ Anatomically graftable vessels and standard CABG indications ¨ Viability involving 18% or more of the LV myocardium irrespective of EF ¨ Operable patient If not ======> Palliative and transplant consideration

Thank you
- Slides: 52