CORNEA Dr Sarika Gadekar Transparent anterior 16 th


 Horizontal Radius of curvature Vertical Anterior 11. 7 10. 6 7.")






































 1 hrly for 48 hrs decrease")
 or trichloroacetic acid (10% - 20%) – caustic and")



























, corneal topography")




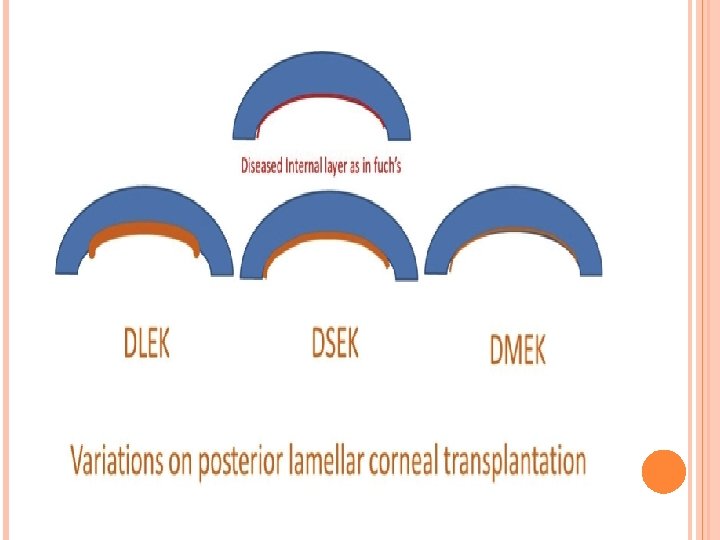
 PENETRATING KERATOPLASTY. (C) ANTERIOR LAMELLAR KERATOPLASTY . (D) DEEP LAMELLAR ENDOTHELIAL KERATOPLASTY. (E)")







- Slides: 98
CORNEA Dr Sarika Gadekar
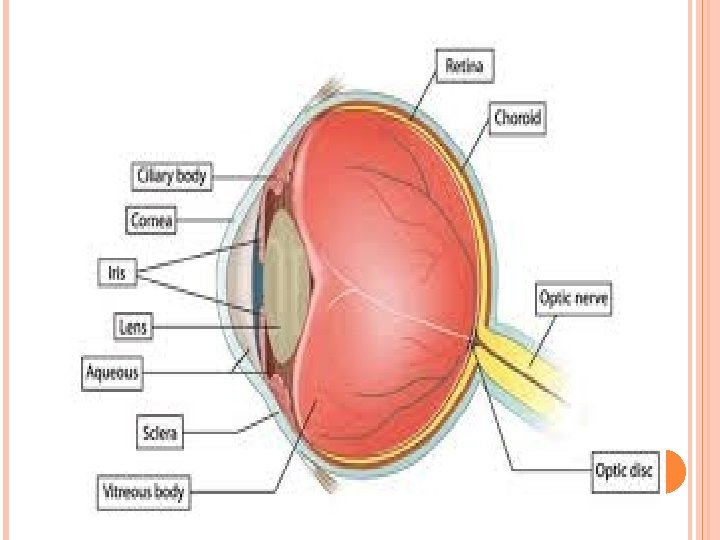
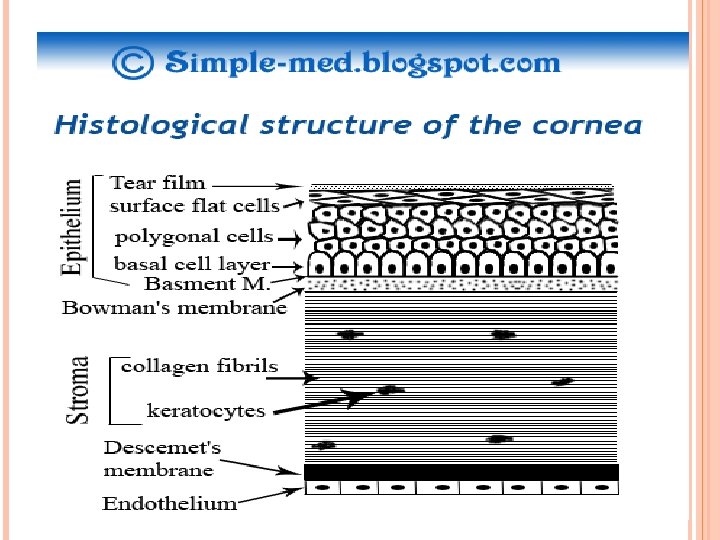
Transparent anterior 1/6 th of the eyeball Curvature of cornea is more than that of rest of the eyeball Limbus – is the junction of sclera and cornea Refractive index is 1. 376
Corneal Diameter (mm) Horizontal Radius of curvature Vertical Anterior 11. 7 10. 6 7. 8 Posterior 11. 7 6. 5 Central Corneal Thickness (mm) 0. 5 -0. 6 Peripheral 1. 2
Avascular Nourished by aqueous, limbal capillaries and oxygen in the tear film Nerve supply– Ophthalmic division of the 5 th cranial nerve (long ciliary nerves) Unmyelinated located in the stroma subepithelial corneal plexus intraepithelial corneal plexus Dense nerve supply sensitve to pain and temperature No sense of propioception
HEALTHY NORMAL ENVIRONMENT
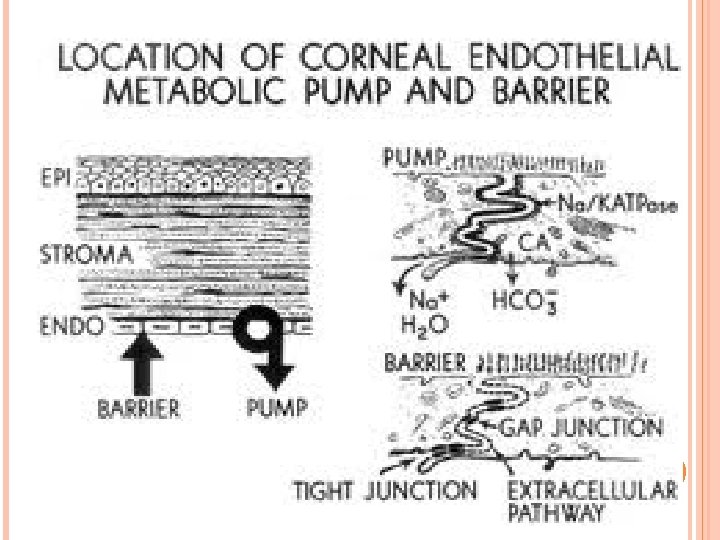
CORNEAL TRANSPARENCY State of Relative Dehydration Reasons – Hydrophobic epithelium and endothelium Endothelial pump Relative hypertonicity of tears and aqueous Absence of blood vessels, pigment Presence of unmyelinated nerve fibres Uniform RI of all layers Uniform spacing of the collagen fibrils in the stroma
ENDOTHELIAL PUMP ANOMALIES
Loss of transparency. Corneal edema
Loss of transparencyvascularization
Ghost vessels
FUNCTIONS Allow transmission of light Refraction Maintainence of structural integrity Protecting eye from infective organisms, noxious substances , UV radiation
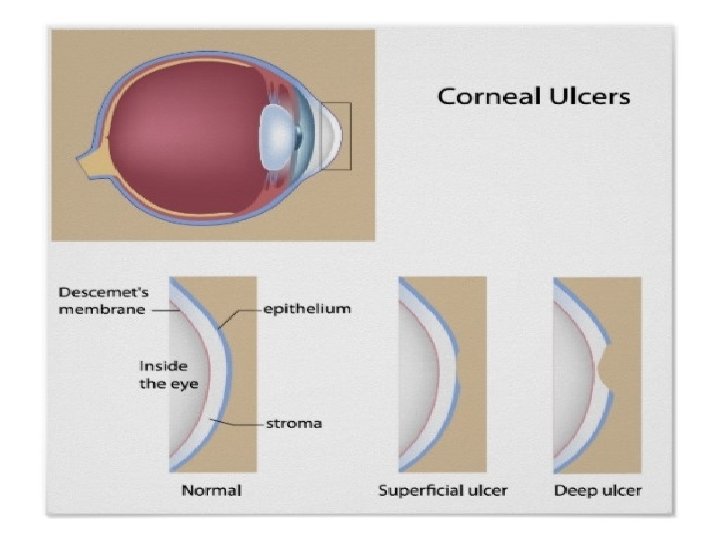
PATHOLOGY Keratitis – Corneal inflammation Superficial Keratitis – Involving epithelium and Bowman’s membrane Superficial Punctate Keratitis – Involving epithelium and Bowman’s membrane in discrete patches Deep Keratitis – Inflammation in the stroma Punctate Epithelial Erosions – non specific tiny slightly depressed epithelial defects which stain with fl
SUPERFICIAL PUNCTATE KERATITIS
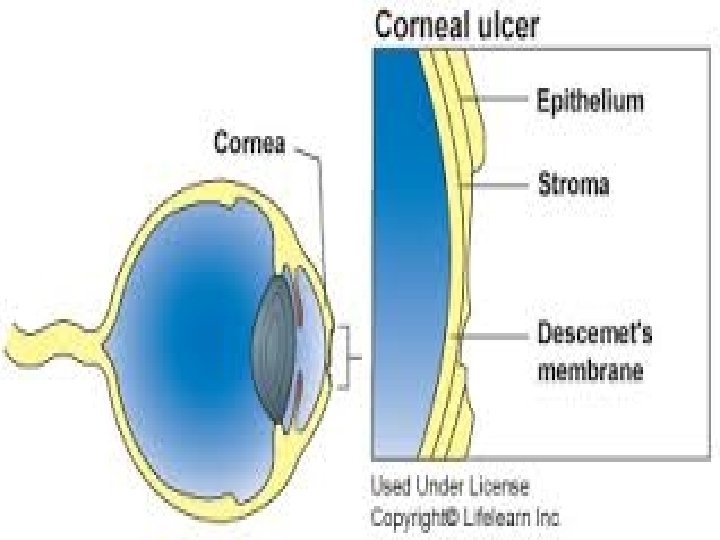
PATHOLOGY Epithelial Defect – Loss of epithelium Abrasion / Erosion – Loss of epithelium without inflammation. Heals within 12 -24 hours. Corneal Ulcer – Loss of epithelium with inflammation in the surrounding cornea Inflammation Infiltration
Epithelial defect Corneal ulcer
CORNEAL OPACITY / SCAR Final outcome of any corneal inflammation / When the clarity of the cornea is disturbed For a opacity to form the Bowman’s layer has to be breached In younger patients tends to clear Eg Post PRK even after Bowman’s layer has been breached Aetiology Acquired after a healed corneal ulcer (Scar) Hereditary in corneal dystrophies (Opacity)
CORNEAL OPACITY Nebular Slight opacification of the cornea Details of iris seen Involves anterior 1/3 ofstroma
CORNEAL OPACITY Macular More dense Details of iris cannot be seen but iris and pupillary margin are visible Involves upto 2/3 of stroma
CORNEAL OPACITY Leucoma Dense white, totally obscuring the view of the iris details and pupil Nearly complete stroma is involved
CORNEAL OPACITY Adherent Leucoma If the iris is adherent to the back of the leucoma After a perforating corneal ulcer Corneo-iridic Scar If the iris tissue is incarcerated in the scar tissue
EFFECT OF CORNEAL Nebula OPACITY in the pupillary area interferes with vision more than an eccentrically located leucoma Loss of brightness of image in small central / paracentral opacities Superimposition of entoptic image of opacity upon clear image of external object
TREATMENT OF CORNEAL OPACITY Nebular – Use Contact lenses Leucoma’s with visual potential – Keratoplasty Leucoma’s without visual potential – - Cometic contact lenses - Tattooing with India Ink, Gold
Corneal edema
ENDOTHELIAL PUMP ANOMALIES
Bullous keratopathy treatment Rx the cause Bandage contact lens Topical Conc. Saline soln/ 15%Na. Cl ointment Strip off epithelium, cover with conjunctiva Full thickness keratoplasty
FILAMENTARY KERATOPATHY Club shaped epithelial threads. Long standing corneal edema, viral keratitis, dry eyes, collagen vascular diseases
Prominent nerves Keratic precipitates
hypopyon
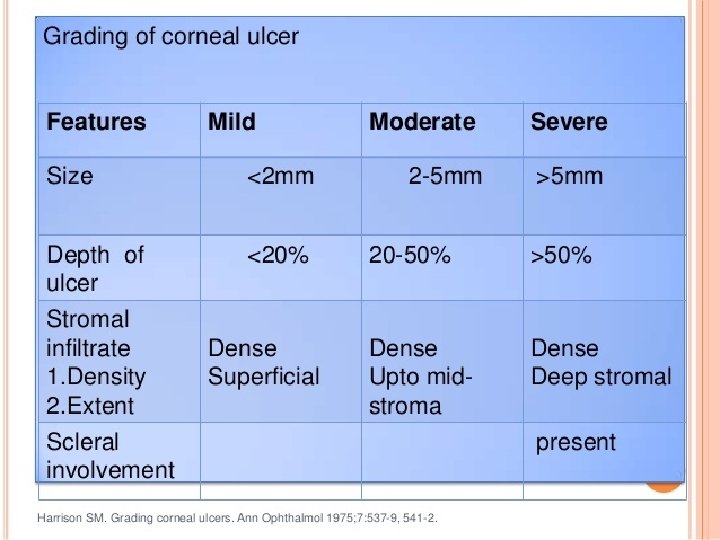
Clinical features of corneal involvement vision Photophobia Lacrimation CCC Foreign body sensation Pain Whiteness of cornea
Corneal surface evaluation – placido’s disc
keratometry
pachymetry
Specular microscopy
CORNEAL INFLAMMATIONS ARE BASED ON location Superficial Deep Suppurative Non- suppurative etiology Infectious Hypersensitivity/ auto-immune marginal keratitis/ ulcer Immune-mediated phlyctenular conjunctivitis d/t Tb interstitial keratitis d/t syphilis Dystrophic Degenerative Neoplastic traumatic
Superficial purulent keratitis- Epithelial defect with stromal infiltration Superficial non-purulent keratitis – viral, acanthamoebic, microsporiodiosis, onchocerciasis Deep stromal keratitis – Systemic infections with limbal spread – Tb, Syphylis Immune mediated – disciform keratitis Scleral inflammation – sclerosing keratitis • • •
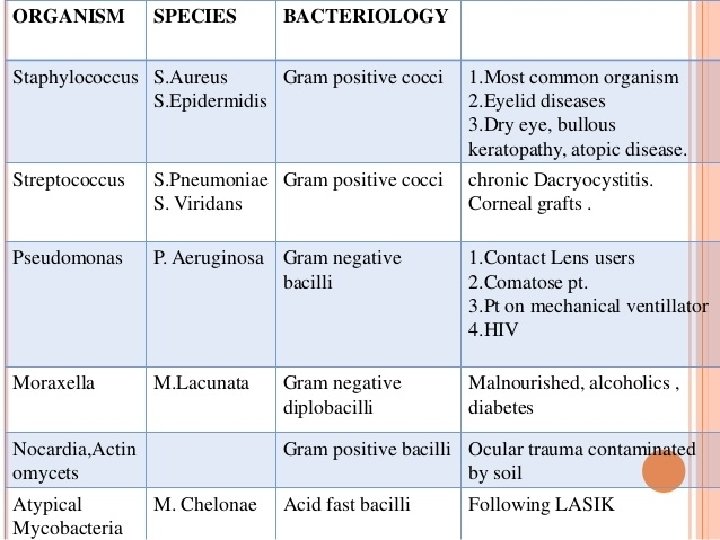
BACTERIAL CORNEAL ULCER / PURULENT KERATITIS Etiology Eoxgenous – pseudomonas, staph. Aureus and albus, pneumococcus, N. gonorrhoea, E. coli N. gonorrhoea and C. diphtheriae invade normal epithelium
STAGES OF CORNEAL ULCER Progressive stage ulcer is saucer- shaped over-hanging edges floor has necrotic material grey zone of infiltration surrounding edema
Regressive stage line of demarcation of PMN’s infiltration and swelling reduces necrotic material shed off – transparent ulcer Stage of healing vascularization (fascicular ulcer) corneal opacity irregular surface - facet
Sequelae
SEQUELAE Keratectasia/ ectatic cicatrix Keratocele / descmetocele Perforation – advantages – corneal nutrition, pain, rapid cicatrization Pseudocornea with anterior synechia Iris prolapse Secondary glaucoma Anterior staphyloma Corneoiridic scar Anterior capsular cataract Corneal fistula Total iris prolapse with pseudocornea Spontaneous expulsion of lens Intraocular h’hage Expulsive h’hage Endophthalmitis panophthalmitis
TREATMENT OF UNCOMPLICATED CORNEAL ULCER Control infection – broad spectrum antibiotics Symptomatic relief - painkillers Cleanliness Heat – prevent stasis and encourage repair Rest - cycloplegics Protection Corneal scrapings – floor and edges – gram and geimsa stain; culture on blood agar, chocolate agar, sabourads dextrose agar and non- nutrient agar with e-coli overlay for acanthamoeba
Antibiotic Concn. frequency Fort. Cephazolin 5% (50 mg/ml) 1 hrly for 48 hrs decrease Fort. Tobramycin 1. 3% (13. 6 mg/ml) “ Fort. Gentamycin 14 mg/ml “ Fort. Vancomycin 0. 3% “ fluroquinolones Eye drops “
Cauterization with carbolic acid (100%) or trichloroacetic acid (10% - 20%) – caustic and antiseptic Corneal opacity – rigid gas-permeable CLs, lamellar keratoplasty, full thickness PK, cosmetic CLs
TREATMENT OF PERFORATED ULCER Small perf. In pupillary area – rest, BCL Tissue adhesive – cyanoacrylate glue Treat secondary glaucoma
HYPOPYON ULCER Ø Ø Ø Staph, strep, gonococci produce hypopyon ulcer Pseudomonas and pneumococci Common in old, debilitated, alcoholics After measles or scarlet fever Pneumococci – ulcus serpens Greyich white/ yellowish disc like lesion Opacity greater at edges, lustreless cornea with hypopyon Ulcer spreads on side of densest infiltration with simultaneous cicatrization Infiltration just anterior to descmet’s membrane – inflammatory process going on both sides – perforation Rx - same
FUNGAL CORNEAL ULCER Aspergillus, fusarium, candida albicans H/o injury with vegetative matter Less symptomatic Dry ulcer, feathery margins, yellow demarcation line Wessely ring
Conjunctival cong , CCC Hypopyon thick , immobile Rx – local natamycin, amphotericin B drops and miconazole ointment for aspergillus and fusarium. topical nystatin for candida severe cases – oral antifungals endophthalmitis – intravitreal antibiotic with antifungal therapeutic PK
VIRAL KERATITIS Herpes zoster, adenoviruses, measles, vaccinia, molluscum contagiosum etc May present as Punctate epithelial erosion Punctate epithelial keratitis
Punctate epithelial erosions Punctate epithelial keratitis Recurrent epithelial erosions Fluorescein +ve Assoc. with conjunctivitis Rx lubricants non- epitheliotoxic antibiotics Steroids contraindicated Deeper epithelial layers Assoc with opacities in BM and stroma Fluorescein –ve Stain with rose bengal Rx lubricants steroids
HERPES SIMPLEX KERATITIS HSV 1 Periodic attacks – carrier Ocular manifestations – blepharitis, conjunctivitis, keratitis and iridocyclitis Starts as superficial punctate keratitis Minute white plaques – in groups - desquamate
Epithelial – dendritic/ geographic Stromal – necrotizing/ nonnecrotizing endothelial
EPITHELIAL KERATITIS Whitish epithelial plaques in groups Desquamate form erosions – superficial punctate keratitis Coalesce form geographic/ dendritic ulcer
DENDRITIC ULCER - PATHOGNOMONIC Chronic ulcer, exacerbation for weeks to months High recurrence rate Corneal sensations
Diagnosis – immunofluorescence, culture of epithelial scrapings Rx Epithelial keratitis- topical antivirals 2 – 3 weeks 5%IDU drops 5 times a day 1%trifluridine 4 times a day 3% acyclovir ointment 5 times a day 3% vidarabine ointment 5 times a day prophylactic antibiotics lubricants Stromal keratitis – topical steroids, topical antivirals and cycloplegics Oral acyclovir 400 mg 5 times a day for herpetic iridocyclitis Oral acyclovir 400 mg BD for 6 months – 1 year reduces recurrence
HERPES ZOSTER KERATITIS/ ZOSTER OPHTHALMICUS Hutchinson sign Nummular keratitis
Varicella zoster virus Presentation – elderly, depressed immunity Focus – Gasserian ganglion – ophthalmic division of trigeminal nerve Supra-orbital, supra and infra trochlear, nasal, rarely infra-orbital Unilateral, does not cross mid line Bilateral in immunocompromised patients Fever, malaise, severe neuralgic pain – eruption Lids red and edematous Ocular complications arise as eruption is subsiding Associated with involvement of nasociliary nerve
Numerous round spots are seen in epithelium, involve stroma to form a coarse subepithelial punctate/ nummular keratitis Anesthetic cornea Associated with iritis, scleral nodules, secondary glaucoma, acute retinal necrosis, 3 rd, 6 th and 7 th cranial nerve paralysis Rx 800 mg acyclovir 5 times a day for 10 days opioid analgesics skin lesions – topical antivirals ocular involvement – topical antibiotic iritis, scleritis – topical steroids with antivirals optic neuritis, 3 rd nerve palsy – systemic steroids lubricants neurotrophic ulcers – tarsorraphy penetrating keratoplasty
IMMUNOLOGICALLY MEDIATED DISEASES
Phlyctenular keratitis • Allergic reaction to tuberculo protein • Grey raised nodule • Nodule breaks down into yellow ulcer • Pain, photophobia • Rx topical steroids antibiotics cycloplegics
Marginal ulcer/catarrhal ulcer
Mooren’s ulcer/ chronic serpiginous ulcer/ rodent ulcer Commonly seen in elderly Rare, degenarative, superficial ulcer starts at margin – spreads circumferentially Erosion initiated by autoimmune lysis of epithelium – release of collagenolytic enzymes (collagenase, proteoglycanase)
Starts as grey infiltrates – break down to form ulcercoalesce Ulcer spreads circumferentially and axially Overhanging edge, vascularised base Severe persistent neuralgic pain, lacrimation Rarely perforates Malignant progression in young adults Diagnosis is by exclusion Rx 4 -7 mm conjunctival strip excision perforation – cyanoacrylate glue with BCL lamellar keratoplasty with IV methotrexate may halt process
INTERSTITIAL KERATITIS Infective/ allergic in origin Children 5 -15 years of age with inherited syphylis Delayed interstitial keratitis in adults >30 years Bilateral, 3 or more weeks interval Involves deeper layers of stroma - no ulceration CCC, one or more hazy patches in deep stroma Start near margins – progress centrally Whole cornea become hazy, lustreless Iris dimly visible
Deep, radial, brush-like vascularization – salmon patches Opacity extends beyond vessels Cornea clears from margins towards centre Ghost vessels persist Disease is a uveitis, keratitis is secondary Diagnosis – clinical signs of syphilis serology Rx systemic penicillin – shorten disease course topical lubricants, steroids, cycloplegics penetrating keratoplasty
Disciform keratitis Immunological stromal reaction Seen in adults Resembles Arthus reaction Central grey disc in mid stroma Descmet’s folds Permanent opacity Mild uveitis Rx topical steroids Topical antivirals Endothelitis
CORNEAL DEGENERATIONS
Arcus senilis Lipoid infiltration of cornea Elderly Starts as crescentric grey line/ whitish band concentric with upper and lower corneal margins Clear zone between limbus and opacity Arcus juvenilis Rare <40 years of age Abnormal serum lipid profile
Band shaped keratopathy Hyaline infiltration of superficial parts of stroma with deposition of calcareous salts Whitish band in interpalpebral area Clear limbal area Chronic uveitis, blind shrunken eye, apakic eyes with silicon oil Hyperparathyroidism, vit D poisoning, Sarcoidosis Rx scraping, EDTA, Excimer laser PRK
ECTATIC CONDITIONS Keratoconus • Inflammatory causes – keratectasia/ anterior staphyloma • Non- inflammatory causes – keratoconus, keratoglobus, pellucid marginal degeneration
KERATOCONUS Congenital – manifests after puberty - bilateral Acquired – trauma, VKC, Down’s syndrome Vision - d/t myopic astigmatism Signs – Munsen sign ‘oil – droplet’ sign Vogt striae, fleischer ring acute hydrops
corneal reflex on placido’s disc keratometry, pachymetry (thinness), corneal topography
Rx early stages – spectacles rigid gas permeable CL penetrating keratoplasty/ lamellar keratoplasty intra corneal ring segment inserts collagen cross linkage
KERATOGLOBUS Congenital, hereditary, bilateral Hemispherical protrusion of cornea Rx same as keratoconus
CORNEAL SURGERIES
Penetrating keratoplasty
(B) PENETRATING KERATOPLASTY. (C) ANTERIOR LAMELLAR KERATOPLASTY . (D) DEEP LAMELLAR ENDOTHELIAL KERATOPLASTY. (E) DESCEMET'S STRIPPING AUTOMATED ENDOTHELIAL KERATOPLASTY. (F) DESCEMET'S MEMBRANE . ENDOTHELIAL KERATOPLASTY
PENETRATING KERATOPLASTY
Cornea is Immunologically priviliged Cadaveric donors Within 6 hours of death (rarely upto 12 hours) Short term preservation 48 – 72 hours Intermediate term preservation upto 30 days Long term preservation (cryo) upto 1 year Indications: optical therapeutic Corneal allografts : full thickness, partial thickness, patch graft Rotational autograft
Complications: Early – wound leak, shallow AC, persistent epithelial defect, secondary glaucoma, uveitis, graft edema, graft failure Late – after 3 weeks – graft rejection, infection, secondary glaucoma, astigmatism Very late – upto 1 year – graft rejection, wound dehiscence Graft failure Common in vascularized cornea, regrafts Rejection can be epithelial, stromal or endothelial Symptoms: pain, vision, photophobia, ccc Signs: epithelial rejection line, endothelial rejection line, stromal edema, ccc, KPs Rx Steroids
REFRACTIVE SURGERIES
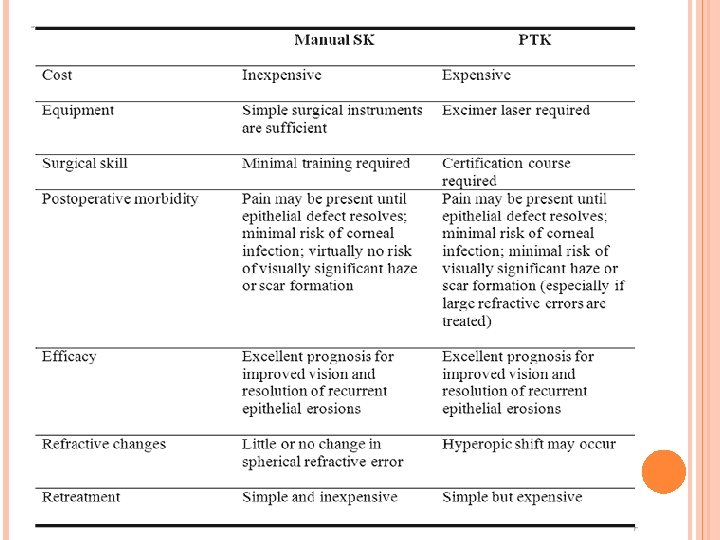
PHOTOTHERAPEUTIC KERATECTOMY
Indications Superficial corneal opacities like band shaped keratopathy, superficial scars, oil droplet keratopathy etc Excimer laser (198 nm) Contraindications: Thin corneas, dry eyes, deeper opacities Side effects: hypermetropia, corneal haze Complications: persistent epithelial defect, infection, hypermetropia, secondary keratectasia
Keratoprosthesis Indications: bilaterally blind with severe OSD like SJ syndrome, recurrent graft rejection Pre-operative requisites: Minimum PL+ Posterior segment Normal Materials used : PMMA, teflon, dacron mesh, osteoodontokeratoprosthesis, cartilage or nail Complications: extrusion, glaucoma, RD, uveitis, membrane formation