Coping with Stress Objectives Evaluate strategies for coping

Coping with Stress Objectives: Evaluate strategies for coping with stress.

Mediating the Stress-illness link • Exercise – Decrease in stress • Gender – Men respond greater to stress • Life events • Type-A personality/behavior – Competitiveness, impatience • Social support – Decrease in illness and stress • Actual or perceived control – Control decreases stress

Two types of coping 1. Approaches 2. Avoidance • Problem solving – Forming a plan of action • Problem avoidance – Refusing to think about the problem • Wishful thinking – Dreaming about better times • Emotional social support – Talking to people about feelings • Instrumental social support – Talking to people and getting advice • Cognitive restructuring – Redefining the problem • Distraction – Link to addictive behavior
 2. Taylor and colleagues")
FOUR Models 1. Moos and Schaefer (Crisis of Illness Theory) 2. Taylor and colleagues (Cognitive Adaptation Theory) 3. Social Support Theory 4. Control Theory
 • Moos and Schaefer – Three processes that make up")
Coping with Illness (stress) • Moos and Schaefer – Three processes that make up the coping process 1. Cognitive appraisal 2. Adaptive tasks 3. Coping skills

Step 1 Cognitive Appraisal • Appraise the situation – How will this influence my life? – Factors • Knowledge • Previous experience • Social support

Step 2 Adaptive Tasks • Illness tasks • General Tasks 1. Dealing with pain and other symptoms 2. Dealing with hospital environment and treatment process 3. Developing and maintaining relationships with health professionals 1. Preserving an emotional balance 2. Preserving self-image 3. Sustaining relationships with family and friends 4. Preparing for an uncertain future
 – – – 2. Logical")
Step 3 Coping Process 1. Appraisal-focused (search for meaning) – – – 2. Logical analysis, mental preparation Cognitive redefinition Cognitive avoidance or denial Problem-focused (confronting and changing so it is manageable) – – – 3. Seeking information and support Taking action to solve problem Identifying rewards (Short Term satisfaction) Emotion-focused – – – Affective regulation (maintain hope) Emotional discharge (venting feelings) Resigned acceptance

Not everyone responds to illness the same way • What determines if the tasks and skills are used? 1. Demographic and personal factors – (age, sex, class, religion) 2. Physical and social/environmental factors – (accessibility of social support and hospital environment) 3. Illness-related factors – (pain, stigma or disfigurement)

Implications of model • What motivates coping? – Maintain equilibrium and normality – Desired outcome of coping is reality orientation • How? – Short-term or long-term goals • Two types of equilibrium – Healthy adaptation • Maturation (positive adjustment to the situation) – Maladaptive response • Deterioration • Does this model work for non-illness stress? – No

Taylor et al. • • Move beyond illness-stress coping only Coping with crisis/stress has three processes 1. Search for meaning 2. Search for mastery 3. Search for self-enhancement • Motivated to maintain a status quo – Maintaining illusions • • cognitive adaptation Based on research with women who have breast cancer

1. Search for meaning • Search for causality (why did it happen to me? ) – 95% of those interviewed gave a cause • Understanding the implications (what effect has it had on my life? ) – Over 50% mentioned improved selfknowledge, self-change and reprioritization • Attributing meaning leads to cognitive adaptation

2. Search for mastery • Mastery achieved through believing another occurrence can be prevented or the illness can be controlled – 66% believed they could influence course or reoccurrence of cancer • Remainder believed that doctors would • Two types – Psychological: positive thinking, meditation – Behavioral techniques: change medications, diet or finding out information

3. Search for Self-enhancement • Build self-esteem – 17% reported only negative changes – 53% reported only positive changes • Comparison – Up: compare with those that are better off – Down: compare with those that are worse off – Most showed downward comparisons

Role of Illusions • Illusions are necessary for cognitive adaptation – “I can control whether my cancer comes back” • Illusions – Positive interpretations of reality – “I know what caused my cancer, I can control whether it comes back” • Better than reality orientation (Moos and Schaefer)

How does Social Support mediate Stress? 1. Main Effect hypothesis 2. Stress Buffering Hypothesis 3. Research: Schwarzer et al. 1994) 4. Pages 15 -16

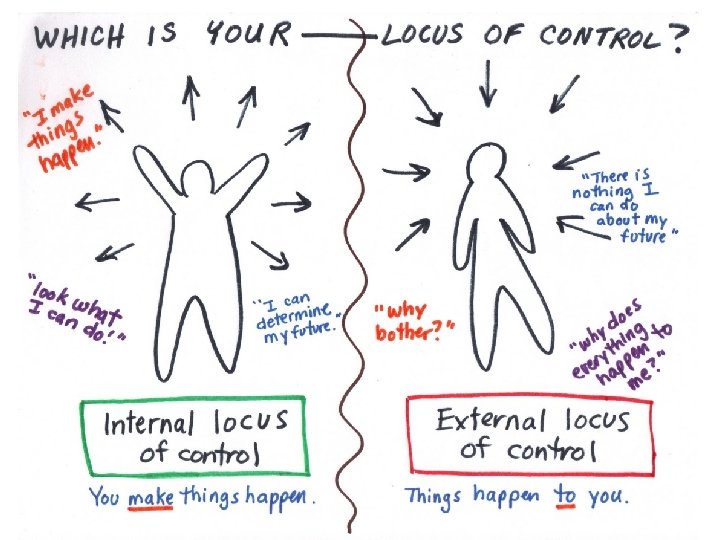
Investigating Control • Psychological theories of control 1. 2. 3. 4. • Attributions and control Self-efficacy and control Categories of control Reality of control Does control affect the stress response? 1. Subjective experience 2. Physiological changes

What is control? 1. Attributions and control 1. Is the cause of the stress controlled by the individual or not • • Controllable cause “I should have prepared better” Uncontrollable cause “the interviewer was biased” 2. Self-Efficacy and control – Individual’s confidence to carry out a behavior – Control is implicit to self-efficacy
 – – – Behavioral control (avoidance) Cognitive control (reappraisal)")
3. Categories of Control (5) – – – Behavioral control (avoidance) Cognitive control (reappraisal) Decisional control (choice over possible outcome) Information control (access information) Retrospective control (could I have prevented …) 4. Reality of Control – Perceived control (I believe…) Most Control – Actual control (I can … ) *** discrepancy is illusory control (I control whether the plane crashed by counting throughout the journey) ***
 – – Stimulus Loud Noise")
…Stress Response…. 1. Subjective Response (Corah and Boffa, 1970) – – Stimulus Loud Noise IV: predictable or nonpredictable DV: Level of Stress Preparation for stress diminishes subjective response to stress 2. Physiological Changes – Uncontrollable increase in corticosteroids

Animal Research on Control • Seligman and Visintainer – IV: uncontrollable and controllable shocks – DV: tumor growth (injection of tumor cells) – Results: • uncontrollable Tumor Growth – Implications: • controllability stress response promote health
 • Natural Environment (Submissive or")
• Manuk et al. 1986 (CHD in Monkeys) • Natural Environment (Submissive or dominant) – Design • IV: New members = unstable environment • DV: Rate of CHD • Results – Dominant/unstable/more CHD • Implications – Control and expectations of control conflict CHD
 – Executive Monkey…i. e. human")
Brady 1958 • Control reduces stress (conflicts with Manuk) – Executive Monkey…i. e. human executives • Design – IV: ability to avoid (control) shock – DV: ulcers and death rate • Results – Executive monkeys dies or became incapacitated • Implications – Constant vigilance (control) illness

Weiss, 1968 • Evaluation of Brady – Sampling error: Selected by learning speed • More emotional learn quicker – High emotion high susceptibility to stress • Follow-up study to correct – Used rats (3 groups) • Results contradicted Brady • Results – Executive negative consequences – No control Severe consequences (increased corticosteroids) – No-shock little deterioration
 – • Job Strain Model")
Human Research • Stress-Illness link (Karasek et al 1981) – • Job Strain Model Participants – – U. S. and Sweden: CHD Three Factors 1. Workload (psychological demands) 2. Autonomy of job (reflecting control) 3. Job satisfaction – Results (Increase in CHD) 1. High demand/workload 2. Low satisfaction 3. Low control

Control and Stress-illness link • Control and preventative behavior – High control maintain healthy lifestyle • Control and behavior following illness – High control change lifestyle • Control and physiology – Control directly influences health via physiological processes • Control and personal responsibility – High control leads to personal responsibility • No behavior change OR • Unhealthy behaviors illness

Benefits to LOW control? • Most theories – High control less stress less illness • BUT…some situations the perception of helplessness leads to less stress – Flying in a plane • Low control low stress • Implications: – Less stressful than trying to control an uncontrollable situation
- Slides: 29