COPD Exacerbations JO RILEY Importance of exacerbations Poorer

COPD Exacerbations JO RILEY

Importance of exacerbations Poorer Quality of Life Greater Airway Inflammation “Frequent Exacerbator ” Faster Decline in Lung Function Higher Mortality

Effect of exacerbations on disease progression Smoke from tobacco and biomass fuel contains ROS, toxins, and particulate matter Viral and bacterial infections FEV 1 (% of predicted) 100 Asymptomatic Stage I 80 Signs and symptoms Stage II Progressive dyspnoea 50 30 Stage III Systemic disease Comorbidities Stage IV Respiratory failure Death 0 25 50 Age (years) Hansel T, Barnes P. Lancet 2009. 75

Frequent exacerbations are associated with increased mortality Probability of surviving 1. 0 0. 8 A p < 0. 0002 0. 6 B 0. 4 p < 0. 0001 p = 0. 069 C 0. 2 0. 0 0 10 20 30 40 50 60 Time (months) A = No exacerbations Soler-Cataluna JJ, et al. Thorax 2005; 60: 925 -931. B = 1 -2 exacerbations C = 3 or more exacerbations

What does an exacerbation mean to a patient? Decline in lung function 1, 2 Increased symptoms (I. e. breathlessness) 6 Greater anxiety 3 Worsening quality of life 4, 5 Social withdrawal Increased risk of mortality 8 More exacerbations 6, 7 Increased risk of hospitalisation 1, 2 1. Garcia-Aymerich J et al. 2001 2. Donaldson D et al. 2002 3. Gore JM et al. 2000 4. Seemungal T et al. 1998 5. Pauwels P et al. 2001 6. Seemungal T et al. 2000 7. Garcia-Aymerich J et al. 2003 8. Anto JM et al. 2001

Who is at risk of exacerbating? �Patients on no medication �Patients with severe disease �Patients with high MRC score �Patients with low BMI �Patients with cardiac arrhythmias �Patients on high levels of medication

Increased risk of dying from COPD Dependent on severity of airflow obstruction: FEV 1< 0. 8 litres (severe disease) - yearly mortality ~25% Poor prognostic indicators �Cor-pulmonalae �Hypercapnoea (raised carbon dioxide levels) �Ongoing cigarette smoking �Weight loss

Prevention of exacerbations �Offer annual influenza vaccinations �Offer pneumococcal vaccination �Give self management advice �Optimise bronchodilator therapy with one or more long acting bronchodilator �Add inhaled corticosteroids (in combination with a LABA) if 2 or more exacerbations per year, or 1 severe exacerbation requiring hospitalisation
 � Usual inhaled/nebulised")
Recognising an exacerbation � More breathless than usual (98% of patients) � Usual inhaled/nebulised therapy not working as well as usual � Cough develops or worsens � Change in sputum amount (66% of patients) � Change in sputum colour (green/purulent) (61% of patients) � Respiratory rate >20 / minute (82% of patients) � Fevers/sweats/rigors Most common causes Bacterial and viral infections � Pollution � Cold weather � Interruption of usual therapy �

Exacerbations – differential diagnosis �Asthma �Pneumonia �Congestive cardiac failure �Pneumothorax �Pleural effusion �Pulmonary Embolus �Cardiac arrhythmia

Exacerbations –What to assess? • Important to assess and document the severity of COPD exacerbations • • Respiratory rate Oxygen saturation (how accurate? ) • • • Check accuracy of pulse oximeter Nail polish Cold hands/poor peripheral circulation Tremor Symptoms

Management of Exacerbations COPD exacerbations are defined as an acute worsening of respiratory symptoms that result in additional therapy. ► They are classified as: Ø Mild (treated with short acting bronchodilators only, SABDs) Ø Moderate (treated with SABDs plus antibiotics and/or oral corticosteroids) or Ø Severe (patient requires hospitalization or visits the emergency room). Severe exacerbations may also be associated with acute respiratory failure. © 2017 Global Initiative for Chronic Obstructive Lung Disease

Treatment of an exacerbation Early recognition and treatment may prevent the need to be hospitalised � Increase inhaled bronchodilators (10 puffs salbutamol via spacer) or commence nebulisers – salbutamol 2. 5 mg and ipratropium 500 mcg 4 times a day � If no response commence oral steroids – prednisolone 30 mg for 5 -7 days � If any evidence of infection (e. g. purulent sputum) commence oral antibiotics � If patient is on oxygen – never increase oxygen without medical advice. � Arrange appropriate review � Consider chest physio / adjunctive personal care Admit to hospital if patient is severely unwell

Management of Exacerbations - Summary © 2017 Global Initiative for Chronic Obstructive Lung Disease

Leaving patient at home? �Arrange follow up �Respiratory community team – leave message for next morning (01865 904418) Home monitoring and adjust therapy Optimise background treatment Educate and provide self management plan Refer to pulmonary rehabilitation Support palliative treatment as appropriate

Safe use of oxygen �Patients are advised that they must not alter oxygen flow without formal assessments and blood gasses �Oxygen alert cards supplied to patients – in messagein-a-bottle �Some patients may have mask to use during exacerbations (normally use nasal) �High risk patients may have home NIV – increasing hours on this can help in exacerbation �(Sats above 92% - alternative strategies to manage breathlessness advised) � FINE LINE BETWEEN TOO MUCH AND TOO LITTLE OXYGEN!
 �New Hypoxia �Respiratory rate")
When to admit? �DNACPR in place? Advanced wishes? (Check message-in-a-bottle) �New Hypoxia �Respiratory rate above 30 despite bronchodilators �No response to treatment? �Already prescribed antibiotics for pseudomonas? �On home oxygen and signs of CO 2 retention
")
Managing Exacerbations Hospital or Home? - When to admit (NICE 2010 - R 135) � Unable to cope at home � Already on LTOT? � Severe breathlessness � Living alone � Deteriorating general � Acute confusion condition � Confined to bed � Cyanosed � Increased peripheral oedema � Impaired level of consciousness � Rapid onset � Significant co-morbidity � Sa. O 2<90% � Changes in chest x-ray � Arterial p. H<7. 35 � Arterial Pa. O 2<7 k. Pa

The ambulance journey � Danish study - Patients arriving by ambulance had a significantly higher risk of arriving acidotic than those who bring themselves in. (Ringbaek 2015) � High flow oxygen can raise Pa. CO 2 within 15 – 20 minutes of administration (NICE 2006) � Target saturation of 88 – 92% in the ambulance – start with low flow oxygen 24 – 28% via venturi mask - titrate up to achieve target saturations. � Observe for drowsiness / flap / bounding pulse / flushed face or palms of hands / confusion

The role of exacerbations in disease progression �Mortality rates associated with COPD exacerbations are high: hospital in-patient mortality rate is at least 10%1, 2 up to 43% of patients will die within 1 year of an exacerbation related admission 3 1. Anto JM et al. Eur Respir J 2001; 17: 982 -994 2. Stoller JK, New Eng J Med 2002; 346: 988 -994 3. Connors et al. Am J Respir Crit Care Med; 1996

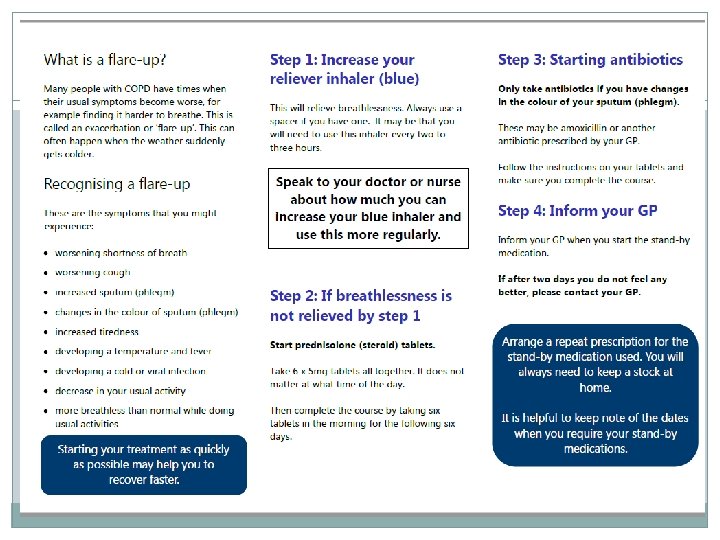
Self Management Plans Aim to help patients: �Manage day to day symptoms �Respond promptly to change in symptoms �In the event of an exacerbation - Start treatment appropriately Oral steroids Antibiotics Adjusting bronchodilator therapy

Discharge criteria and recommendations for follow up �Full review of all clinical and laboratory data �Check maintenance therapy and understanding �Reassess inhaler technique �Ensure understanding of withdrawal of acute therapy – steroids and antibiotics �Assess need to continue oxygen therapy �Provide management plan for comorbidities and follow up �Ensure follow up arrangements made �All clinical and investigational abnormalities have been identified © 2017 Global Initiative for Chronic Obstructive Lung Disease

1 -4 weeks follow up �Evaluate ability to cope in his / her own environment �Review understanding of treatment regime �Reassessment of inhaler technique �Reassess need for long term oxygen therapy �Document the capacity to undertake physical activity and activities of daily living �Document symptoms – CAT or m. MRC �Determine status of co-morbidities © 2017 Global Initiative for Chronic Obstructive Lung Disease

12 – 16 week follow up �Evaluate ability to cope in his / her own environment �Review understanding of treatment regime �Reassessment of inhaler technique �Reassess need for long term oxygen therapy �Document the capacity to undertake physical activity and activities of daily living �Measure Spirometry – FEV 1 �Document symptoms – CAT or m. MRC �Determine status of co-morbidities © 2017 Global Initiative for Chronic Obstructive Lung Disease
: ► An exacerbation of COPD")
Management of Exacerbations OVERALL KEY POINTS (1 of 3): ► An exacerbation of COPD is defined as an acute worsening of respiratory symptoms that results in additional therapy. ► Exacerbations of COPD can be precipitated by several factors. The most common causes are respiratory tract infections. ► The goal for treatment of COPD exacerbations is to minimize the negative impact of the current exacerbation and to prevent subsequent events. ► Short-acting inhaled beta 2 -agonists, with or without short-acting anticholinergics, are recommended as the initial bronchodilators to treat an acute exacerbation. © 2017 Global Initiative for Chronic Obstructive Lung Disease
: ► Maintenance therapy with long-acting")
Management of Exacerbations OVERALL KEY POINTS (2 of 3): ► Maintenance therapy with long-acting bronchodilators should be initiated as soon as possible before hospital discharge. ► Systemic corticosteroids can improve lung function (FEV 1), oxygenation and shorten recovery time and hospitalization duration. Duration of therapy should not be more than 5 -7 days. ► Antibiotics, when indicated, can shorten recovery time, reduce the risk of early relapse, treatment failure, and hospitalization duration. Duration of therapy should be 5 -7 days. ► Methylxanthines are not recommended due to increased side effect profiles. © 2017 Global Initiative for Chronic Obstructive Lung Disease
: ► Non-invasive mechanical ventilation should")
Management of Exacerbations OVERALL KEY POINTS (3 of 3): ► Non-invasive mechanical ventilation should be the first mode of ventilation used in COPD patients with acute respiratory failure who have no absolute contraindication because it improves gas exchange, reduces work of breathing and the need for intubation, decreases hospitalization duration and improves survival. ► Following an exacerbation, appropriate measures for exacerbation prevention should be initiated (Rehab, inhaled therapy, self management plans etc) © 2017 Global Initiative for Chronic Obstructive Lung Disease

What do COPD patients in Oxfordshire have access to? Home Oxygen assessment and review Service 01865 787186 Flying assessments – Lung function lab at Churchill Community services: Breathe easy Individual physio COPD One Stop Shop out-patient service at Churchill Hospital Pulmonary rehabilitation Community 01865 787177 COPD patient Respiratory nursing Service in primary and secondary care: disease education and admission avoidance 01865 904418 Early discharge scheme Community team in-reach to hospital 01865 225472 Liaison with palliative Care and case management Respiratory registrar advice at Chest unit Bleep hospital team

Predicting prognosis • Extremely difficult to predict prognosis for individual patients • Many parameters identified but only a guide i. e. MRC Dyspnoea Scale, BODE, severity of disease, number of admissions • End of Life Discussions/Advanced Care Planning should be offered during a period of disease stability • Discussions about preferences for NIV, intubation and resuscitation are important

Predicting Prognosis – stable COPD � FEV 1 * � Age � Arterial blood gases (Pa. CO 2 > Pa. O 2) � Body Mass Index � Co-morbidity � Number of exacerbations � Exercise capacity

Predicting prognosis – During acute exacerbation of COPD Age >70 Hospital type/resources FEV 1 <30% predicted Sa. O 2 on admission p. H 7. 26 Pa. O 2/Fi. O 2 Pa. CO 2 >8 k. Pa Diffusion capacity Pa. O 2 <7. 3 k. Pa Body mass index <18 No of admissions Albumin Other co-morbidity

Illness Trajectories Typical illness trajectories for people with progressive chronic illness. Adapted from Lynn and Adamson, 2003. 7 With permission from RAND Corporation, Santa Monica, California, USA. Published in BMJ Murray, S. A et al. BMJ 2005; 330: 1007 -1011

How areare people who diediedie How people who How are people who from COPD affected? from. COPD affected? In the last year of life 40% had breathlessness unrelieved 68% had low mood unrelieved 51% had pain unrelieved 20% did not know they might die 70% died in hospital (for 25% of whom it was not the best place to die) Elkington, White, et al Pall Med 2005 19: 485 -491

What can we do to help breathlessness? � 3 F’s Forward leaning Focus on breathing out Fan �Pacing Allow time e. g washing in stages Regular rests �Reassurance
 Cough (Opiates) Secretions (anticholinergics) Anxiety (benzodiazepines) Confusion")
Symptom control Dyspnoea (Opiates, oxygen, cool air) Cough (Opiates) Secretions (anticholinergics) Anxiety (benzodiazepines) Confusion (oxygen, haloperidol, chlorpromazine) British National Formulary 2008 Non pharmacological management Breathing Training Walking aids Hand held fan Pacing Anxiety management Aids for ADLs
- Slides: 37