COPD Chronic BRONCHITIS AND EMPHYSEMA the GOLD committee

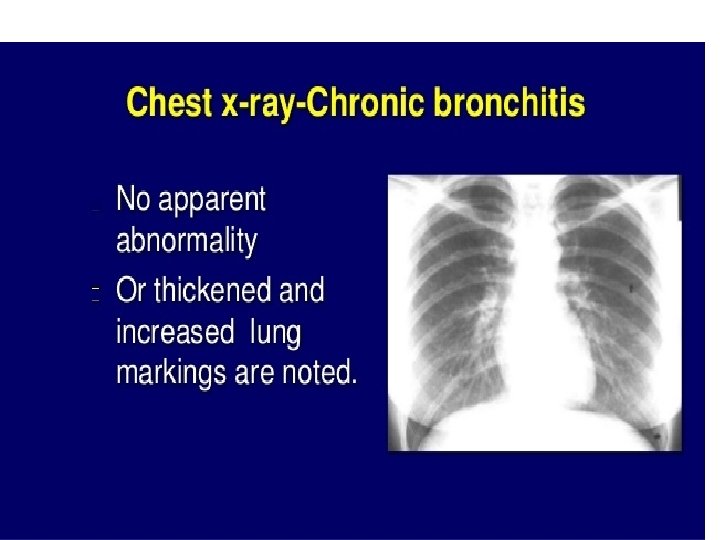
COPD Chronic BRONCHITIS AND EMPHYSEMA

the GOLD committee defines RECENTLY COPD as a "common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation. . . usually caused by significant exposure to noxious particles or gases. "
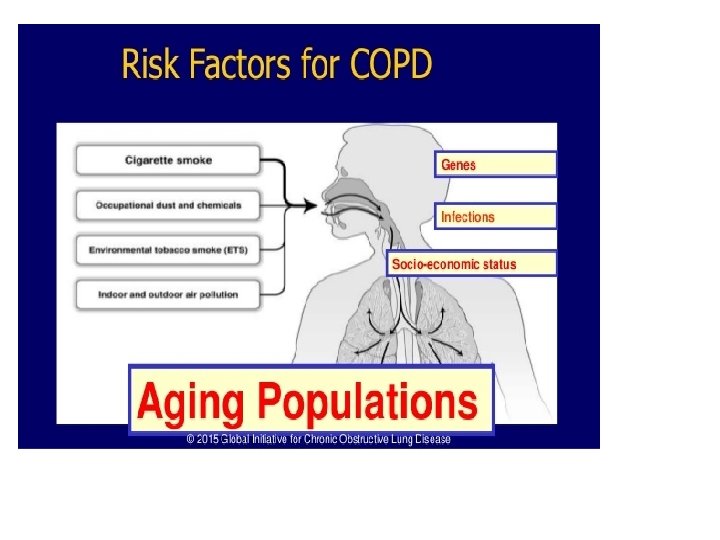

The updated GOLD report acknowledges that we yet don't fully know where the tipping point is in relation to who gets COPD and who doesn't. In addition to exposure to cigarettes, the GOLD committee recognizes other possible factors linked to the disease, including: • • Poor lung growth during gestation and childhood Exposure to noxious chemicals in occupational settings Different types of air pollution Poor socioeconomic status Poorly ventilated dwellings Exposure to burning fuels (including wood fires and cooking fuel) Other lung disorders (such as chronic bronchitis or infections) An abnormal inflammatory response, perhaps congenital or the result of progressive or prior lung injury



Valve Surgery As the air sacs in your lung get larger, your lung can fill with too much air every time you breathe in. “In some patients with overaerated lungs, if a portion of the lung is removed, they may feel a lot better. There’s less trapping of air. Because of that, the standard treatment has been to take out the damaged part of your lung with surgery, but valve surgery is now another option. “The surgeon can use a bronchoscope to put a one-way valve in the airway. This allows the overexpanded part of lung to release air out of the airway, but not to let air in.
 and longacting muscarinic antagonists (LAMAs), can be used")
Combination Therapy long-acting beta-2 agonists (LABAs) and longacting muscarinic antagonists (LAMAs), can be used together to offer more relief of symptoms

Both types of drugs make airways smaller. “You could start out with a LABA and add a LAMA later, but you should not hesitate to start treatment with both Patients can now get combinations of all drugs in one inhaler, so it’s a more convenient

IL-5 drugs Doctors can use blood tests to divide people with COPD into smaller groups to prescribe more targeted treatments for them, Hatipoglu says. For example, one group includes people with eosinophilia, a high number or percentage eosinophils in their blood. Eosinophilia is more common in asthma, but some people with COPD have a high amount of these white blood cells, too. If levels are above 300, a new group of biologic drugs called IL-5 antagonists might work well. For now, they’re approved only for severe asthma, not COPD, but “new trials of the drugs for people with COPD


- Slides: 50