Cook Cervical Ripening Balloon Product information 18 Fr

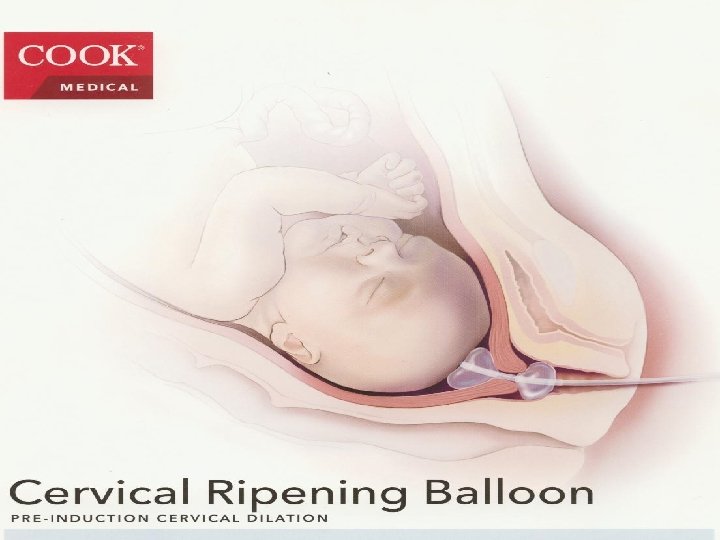

Cook Cervical Ripening Balloon • • • Product information 18 Fr, 40 cm Dual 80 ml balloons 100% Silicone Box of 10 J – CRB – 184000 or G 48149 •

Advantages of this balloon over other methods include • It is particularly successful in women with unfavourable cervices • It is non pharmacological, so does not cause hyperstimulation • It is relatively easy to insert • Reduces the need for multiple vaginal examinations • Reduced the need for continuous monitoring • Increases the chances of vaginal delivery by producing a primed dilated cervix for ARM • Can be used for women with IUD 3 rd trimester IUDS reducing the need for multiple vaginal examinations

Disadvantages • May require a doctor to insert in lithotomy position • Catheter remains for 12 – 24 hours which may be unacceptable to women

Contra – indications • • • • Patients receiving or planning to undergo exogenous prostaglandins Placenta previa / vasa previa or placenta accerta Transverse lie / breech / head above the pelvic brim Ruptured membranes Severe maternal / fetal compromise ( e. g. PET requiring urgent delivery ) Multiple gestation Polyhydramnios Abnormal fetal heart rate changes Any contraindication to induction of labour Active genital herpes Invasive cervical cancer Pelvic structural abnormality Previous hysterotomy / uterine perforation / myomectomy traversing the myometrium

Cautions • • • • Must not be left for more than 24 hours Must be used with care in women with previous caesarean section If fetal membranes rupture whilst the CCRB is in situ then it must be removed and plan of management discussed with the consultant on call Must not be used in women who have recently been given prostaglandins ( < 12 hours ) as this accentuates the adverse events associated with their use Hyperstimulation Impaired utero – placental circulation Tachysystole Uterine rupture Amniotic fluid embolism Pelvic pain Retained placenta Genital bleeding shock Bradycardia

Setting up for cooks cervical ripening balloon insertion • • • Equipment Syringes 60 ml × 4 Needle 16 gauge needle Vaginal pack Sponge holder × 1 Normal saline bags 100 ml × 2 Cook cervical ripening balloon Disposable speculum Water / aqueous savlon solution to clean

Patient preparation 1 - the patient is brought to labour ward 2 - once a normal CTG is obtained the doctor is informed to insert the balloon 3 -confirm presentation / placental localization with abdominal ultrasound 4 - place the patient on the left lateral position / lithotomy position 5 -Insert large vaginal speculum to gain cervical access 6 - Clean the cervix with the appropriate cleaning solution to prepare for device insertion

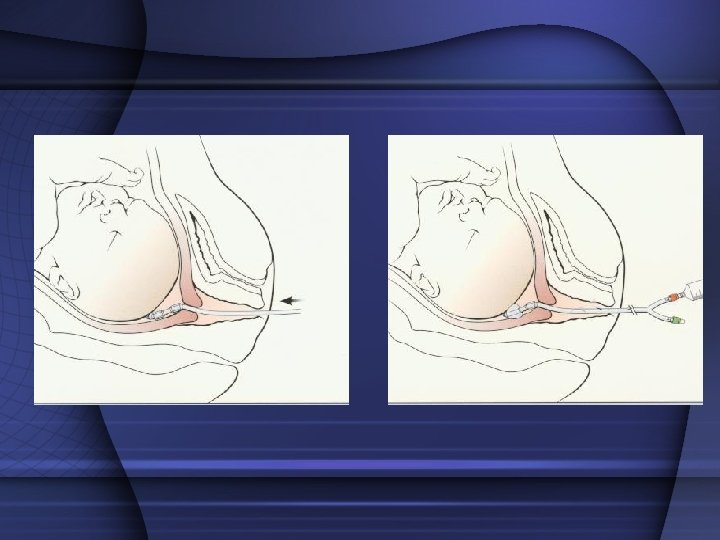
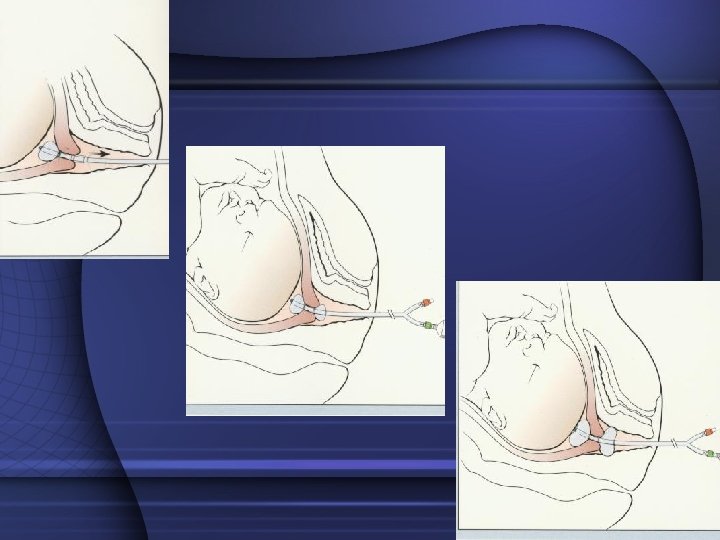
Device insertion • Insert the device and advance both balloon into the cervical canal • Inflate the internal balloon with 40 ml of normal saline through the check flow valve u ( red) • Once inflated pull back until balloon rests against the internal os • The vaginal balloon is now inflated to 40 ml through check flow valve v (green) • Once on either side of the cervix and device the speculum is removed • Add more fluid into each balloon until both balloons are filled to 80 mls each • Do not over inflate the balloon • Taped to patients leg • Remove after 12 -24 hours

Procedure for removal of the balloon and afte r • 12 - 24 hours later the balloon is removed , this is • • • done by removing fluid from both balloon. The patient dose not need to be placed in lithotomy for this. Once the balloon is removed, an ARM should be done soon after. If not contracting within one hour, then an oxytocin infusion should be commenced. In the event that the head is high ARM should be avoided until the head is lower in the pelvis. Consideration for commencement syntocinon with intact membranes

• PGE 2 , Oxytocin , Ripening Balloon • Results • Balloon and PGE 2 Were comparable - Change in Bishop score – 5 - Interval to delivery - 20 hours - Cesarean Rate • Both methods were superior to oxytocin

• PGE 2 , Oxytocin , Ripening Balloon • Results • Balloon was superior to both PGE 2 & Oxytocin - Cervical Dilation - > 3 cm in > 90% of patients - Failure Rate - < 10% • Compared to over 20% for PGE 2 & 50% for oxy
- Slides: 15