Convulsive Status epilepticus Dr Jithangi Wanigasinghe Senior Lecturer












 4 (13%) 7 (24%)")




 Premonitory")






, Lacosamide,")




 monitoring • • Initiated for RSE (after one hour) Useful")






- Slides: 40
Convulsive Status epilepticus Dr. Jithangi Wanigasinghe Senior Lecturer Consultant Paediatric Neurologist MPhil, MD, DCH
Scope • What is CSE in the ED? – Operational definition and new definition • What are we dealing with? – Underlying aetiology • What do we do? – Optimal management
Definition Single seizure lasting more than 30 -min duration or a series of epileptic seizures during which function is not regained between ictal events in a 30 -min period Commission of Epidemiology and prognosis ILAE 1993
Operational definition for management of SE Generalized, convulsive status epilepticus in adults and older children refers to a 5 min of (a) continuous seizures or (b) two or more discrete seizures between which there is incomplete recovery of consciousness Lowenstein D H 1999
New definition of CSE Status epilepticus is a condition resulting either from the failure of the mechanisms responsible for seizure termination or from the initiation of mechanisms, which lead to abnormally, prolonged seizures (after time point t 1). It is a condition, which can have long-term consequences (after time point t 2), including neuronal death, neuronal injury, and alteration of neuronal networks, depending on the type and duration of seizures. Trinka E. 2015
Conceptual definition with two operational time points Onset t 1 Length of the seizure and the time point (t 1) beyond which the seizure should be regarded as “continuous seizure activity. ” t 2 The time of ongoing seizure activity after which there is a risk of long-term consequences
Epidemiology • • 50 per 100, 000 population Highest in children Bimodal increase in incidence Significant mortality – 22%-23% for children – 26% for adults • Neurological morbidity in 11 -16% • Refractory SE (RSE) is common (31 -44%)
Stages of SE Stage 1 Early phase Premonitory SE, Impending SE 5 -10 min Stage 2 Established SE 10 -30 min Stage 3 Refractory SE Subtle SE, stuporous SE Stage 4 Super-refractory SE : SE that continuous in spite of treatment with anaesthetics for > 24 hrs 30 -120 min >24 h
Scope • What is CSE in the ED? – Operational definition and new definition • What are we dealing with? – Underlying aetiology • What do we do? – Optimal management
Underlying aetiology • Commonest single group of causes is acute symptomatic aetiology • Same for adults and children • In adults – CVA commonest in developed countries and elderly – CNS infections commonest in developing countries Murthy J M K
Epilepsy and Behavior 2015
Causes of CSE in children • • • Hypoxic brain injury CNS Infections Traumatic brain injury Metabolic derangements CNS demyelinataion Vascultis, Autoimmune encephalitis Shorvon S 2006
Acute symptomatic Febrile status Remote symptomatic Epilepsy Unclassified 9 (31%) 4 (13%) 7 (24%) 2 (06%) n=29
Scope • What is CSE in the ED? – Operational definition • What are we dealing with? – Underlying aetiology • What do we do? – Optimal management
Therapeutic principles • Address pathophysiology – GABAA Agonists – NMDA antagonists – multiple receptors or ion channels • Rx plan according to stages • Considerations – ease of administration – onset of action (rapid) – duration of action (intermediate to long) – spectrum of activity (broad) – minimal morbidity
Therapeutic principles Commence rapidly and continue sequentially Use therapeutic doses ALWAYS Critical care treatment and monitoring Treatment of underlying cause Commencement of neuro-protective mechanisms • Constant management of complications • • •
Stages of SE Stage 1 Early phase Premonitory SE, Impending SE 5 -10 min Stage 2 Established SE 10 -30 min Stage 3 Refractory SE Subtle SE, stuporous SE Stage 4 Super-refractory SE : SE that continuous in spite of treatment with anaesthetics for > 24 hrs 30 -120 min >24 h
Stages of SE Stage 1 Early phase (MAY BE PRE or IN HOSPITAL) Premonitory SE, Impending SE 5 -10 min BDZ first choice for out-of- hospital Mx IV – Lorazipam (Alldredge BK 2001) IM – Midazolam Rectal Diazepam in children (Dreifuss FE 1998) IV Diazepam Nasal or buccal – MDZ (Scott RC 1999, Mc. Intyre J 2005) Clear benefit of prehospital Rx with LRZ or DZP
Early phase SE Trinka E 2015
Key highlights • Out of hospital administration – Clear benefit shown due to early SE abolition – Buccal MDM favoured over DZP • In hospital when resuscitation facilities available – Use the IV preparations recommended – Lorazepam favoured
Stages of SE 5 -10 min Stage 2 Established SE 10 -30 min p. H water solubility and neutral • • more rapid administration with less adverse effects Second-line drugs when BDZ fail to • terminate compatibility with all IV fluids IV phenytoin/fosphenytoin IV phenobarbate IV sodium valproate IV leveteracetam No clear evidence to support one over the other for CSE termination
Established status Trinka E 2015
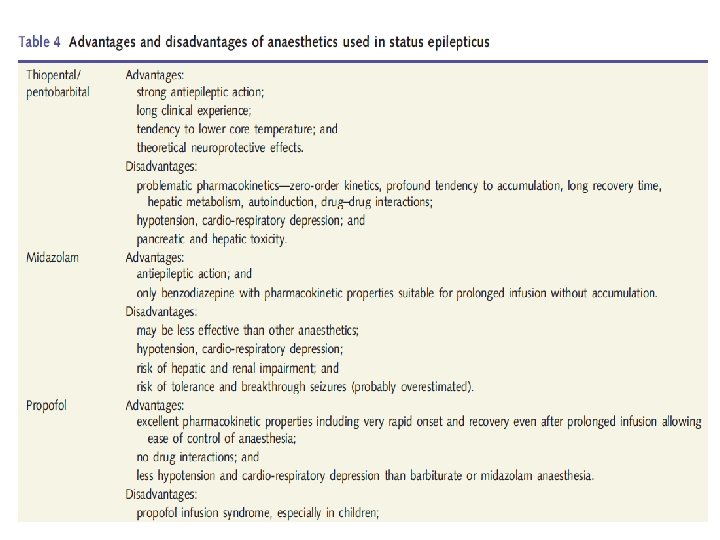
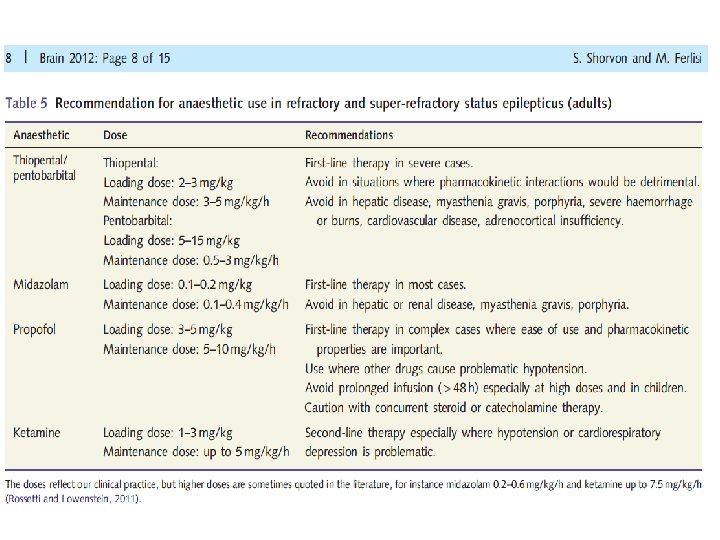
Stages of SE 5 -10 min 10 -30 min Stage 3 Refractory SE Subtle SE, stuporous SE • NO RCTs • Continuous infusion (c. IV) of anesthetic agents: - Thiopental/ pentabarbital, midazolam and propofol (Shorvon S 2012) • Successful Rx with propofol in 2/3 of RSE • For 24– 48 hours of electrographic control by c. EEG monitoring • Dosing titrated to cessation of electrographic seizures or burst suppression 30 -120 min
• Propofol: IV bolus 2 mg/kg, repeated if necessary, followed by a continuous infusion of 5– 10 mg/kg/hour initially, reducing to maintain a burst suppression (usually 1– 3 mg/kg/hour) • Thiopental: IV bolus 100– 250 mg given over 20 s with further 50 mg boluses every 2– 3 min until seizures are controlled, followed by a continuous IV infusion to maintain a burst suppression (usually 3– 5 mg/kg/hour) • Midazolam: IV bolus 0. 1– 0. 3 mg/kg at a rate not exceeding 4 mg/min initially, followed by a continuous IV infusion to maintain a burst suppression pattern (0. 05– 0. 4 mg/kg/hour).
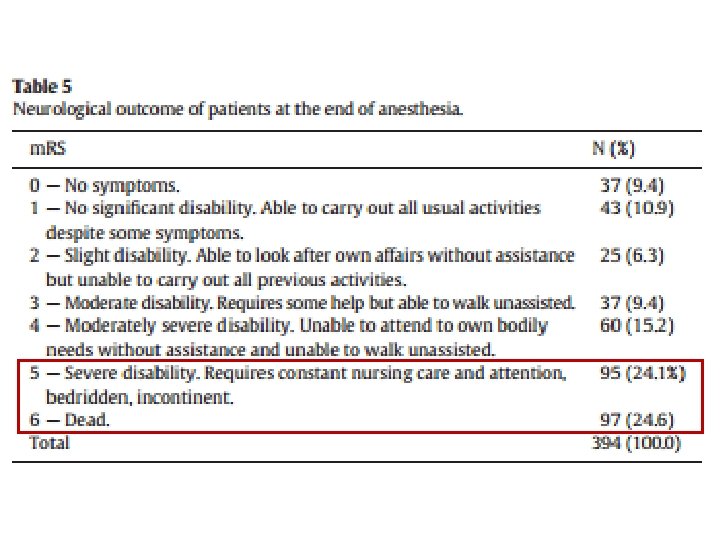
Stages of SE No RCTS Use different conventional AEDs – TPM (via NG), Lacosamide, LEV Inhalational agents - isoflurane and desflurane IVIG, High dose steroids Ketamine (NMDA receptor Antagonist) Budesonide Ketogenic diet Magnesium Sulphate, pyridoxine Epilepsy surgery, Vagal nerve stimulation, DBS Stage 4 Super-refractory SE : SE that continuous in spite of treatment with anaesthetics for > 24 hrs 10 -15% of all CSE Outcome – 35% mortality, 35% recovery to baseline (Shorvon S 2012) 5 -10 min 10 -30 min 30 -120 min >24 h
Anaesthetics in SRE • How long to use? – Exotoxic damage already occurred – ? Risk of anaesthesia exceed risk of SE? • Complications of anaesthesia • How to cycle? – Initially 24 -48 hour cycles and then longer • Should one switch anaesthetics? – Prolonged propofol carries specific risk – What stage to switch ? ? • NO DATA ON THESE POINTS
Anti Epileptic drug therapy • Approach to use AEDs in SRE (via NG / PEG) • Purpose – coverage when anaesthetic effects are withdrawn • Principles – Polytherapy with two – High dose – Avoid frequent switching – Favour those with lower interaction potential, predictable kinetics and without renal or hepatic toxicity – Avoid GABAergic AEDs
Concommittent multimodal approach
Common reasons for treatment failure • Under-dosing at the stage of established SE • Neglecting maintenance therapy • Misdiagnosis- i. e. psychogenic nonepileptic status, drug-induced or metabolic encephalopathy • Failure to identify and treat the underlying etiology • Failure to address Iry complications
Continuous EEG (c. EEG) monitoring • • Initiated for RSE (after one hour) Useful for titration of other maintenance AEDs Duration – at least 48 hours if NCSE treatment endpoints for c. EEG monitoring – cessation of nonconvulsive seizures – diffuse beta activity – burst suppression 8– 20 seconds’ intervals – complete suppression of EEG
Supportive management • Assisted ventilation and cardiovascular monitoring • Vasopressor agents • Cerebral oedema lowering agents • Continuation of maintenance AEDs • Brain cooling
Systemic complications of SRE • Complications due to therapy with inhalational Anaesthetics – Hypothermia, infection, death • Complications due to prolonged ICU stay and immobility – PE, DVT – Pulmonary complications – Sepsis, colitis – Skin complications, fungal infections – Critical illness nopathy/ neuropathy
Systemic complications of SRE • Complications due to status and treatment • Complications due to treatment
Prognostic factors • Poor outcome related to – underlying etiology – de novo development of SE in hospitalized patients – older age – impairment of consciousness – duration of seizures – focal neurological signs at onset – presence of medical complications
Summary • What is CSE in the ED? – Operational definition • What are we dealing with? – Underlying aetiology • What do we do? – Optimal management