Controversies in Endodontics SingleVisit Versus Multivisit Treatment Introduction







 It reduces the number of patient’s appointments while achieving")
 The longer single visit appointment may be tiring and")




 Teeth without apical periodontitis did")
 Found that 90% of success was achieved in")






 Disease Normal Periapical Tissues Symptomatic Apical Periodontitis ( SAP )")

 flat, (B) beveled & (C) notched. D-F: Closed-ended needles; (D)")



 v Rins. Endo v Endo. Vac v Self adjusting")







, rotary system. v It adjusts to the anatomy of the")
 41")


- Slides: 45
Controversies in Endodontics Single-Visit Versus Multivisit Treatment
Introduction Over the past decade, , the development of advanced instruments and devices as: nickel titanium rotary instrumentation, more reliable apex locators, ultrasonics, microscopic endodontics, digital radiography, newer obturation systems, biocompatible sealing materials and new irrigants & irrigation devices have helped practitioners to perform endodontic procedures more effectively and efficiently than ever before. All of these advances increase the efficiency of treatment performance and the trend to use single-visit endodontics in the dental clinics. Completing the endodontic treatment in a single visit is an old concept more than 100 years ago. Nowadays, single visit appointment endodontics has gained increased acceptance as the best treatment for many cases. The rational for one visit treatment regime are less stressful and only one anesthesia is needed, which makes it very well accepted by the patient, less time-consuming, reduces the risk of inter-appointment contaminations, less expensive and more productive for the clinician. Recent studies have also shown that there is no difference in quality of treatment, incidence of post- treatment complications, or success rates between single-visit and multiple visit root canal treatment.
DEFINITION q Single visit endodontic therapy is defined as the conservative , non surgical root canal treatment of an endodontically involved tooth consisting of cleaning and shaping, and obturation of the root canal system in one visit. q Many dentists nowadays are preferring single visit endodontic treatment because of many advantages. Perhaps, the most important advantage is the prevention of root canal contamination and bacterial re-growth that can occur when the treatment is prolonged over an extended period.
HISTORY Historically the single visit procedure can be traced through the literature for more than 100 yrs. Although the concept remained constant , the technique varied. Following world war II there came a reappearance of single visit endodontics. initially it started with the immediate root resection i. e. apicectomy, but later some of the clinicians began to practice single visit endodontics without periapical surgical procedures.
Guidelines for single Visit Endodontics Success in endodontic therapy is based on v Accurate diagnosis v Proper case selection v Use of skilled techniques of treatment The first and important criteria is that single visit endodontics should not be undertaken by inexperienced clinicians. The dentist must posses a full understanding of endodontic principles and the ability to exercise these principles fully and efficiently. As a guideline, the case should be one that can be completed within 60 minutes. Treatments that takes considerably longer time should be done in multiple
Oliet’s criteria for case selection include : Ø Positive patients acceptance. Ø Sufficient available time to complete the procedure properly. Ø Absence of any acute symptoms requiring drainage via the canal and of persistent continuous flow of exudates or blood. Ø Absence of anatomical obstacles like v calcification in the canals, and v procedural difficulties (ledge formation, blockage, perforation, inadequate fills)
Indications for single visit Ø Uncomplicated vital cases. Ø Fractured anterior or bicuspid teeth where esthetics is a concern and temporary post and crown are required. Ø Physically disabled person who cannot come on multiple visits. Ø Patients with heart valve damage or prosthetic implants who require repeated regimens of prophylactic antibiotics. Ø Necrotic, uncomplicated teeth with draining sinus tracts. Ø Patients who require sedation or operating room treatment Contra Indications for Single visit. Ø Painful, necrotic tooth with no sinus tract for drainage. Ø Teeth with severe anatomic anomalies or cases with procedural difficulties Ø Asymptomatic nonvital molars with periapical radiolucencies and no sinus tract. Ø Patients who have symptomatic apical periodontitis with severe pain on percussion. Ø Most of the re-treatment cases. Ø Patients with TMJ dysfunction.
Advantages of single visit. 1) It reduces the number of patient’s appointments while achieving predictably high levels of success and patients comfort. 2) It eliminates the chance for inter appointment microbial contamination and flare-ups caused by leakage or loss of the temporary seal 3) For anterior cases it allows immediate use of the canal space for retention of a post, and construction of an esthetics temporary crown 4) Allows the practitioner to prepare and fill the canals at the same appointments without the need for the clinician’s refamiliarization with the canal anatomy at the next visit. 5) It minimizes fear and anxiety in the apprehensive patients. 6) It eliminates the problem of the patient who does not return to have their case completed.
Disadvantages of Single Visit. 1) The longer single visit appointment may be tiring and uncomfortable for the patient. Some, patients especially with TMJ dysfunction or other impairments may not be able to keep their mouth opened long enough for a single appointment procedure. 2) Flare ups cannot be easily treated by opening the tooth for drainage. 3) if hemorrhage or exudation occurs, it may be difficult to control that and to complete the case at the same visit, and if it doesn’t stop after pulp extirpation also, then better to go for multiple visit. 4) Difficult cases with extremely fine, calcified, multiple canals may not be treatable in one appointment without causing under stress for both the patient and the clinician. 5) The clinician may lack the expertise to properly treat a case in one visit. This could result in failures, flare up etc. . .
PATIENT CONSENT The patient should accept the proposed single appointment procedure. SYSTEMIC EVALUATION AND PREMEDIc. ATION : A history of Myocardial infarction within the past six months is contraindicated for elective dental treatment. These patients should be treated with a stress reduction protocol which includes short appointments , psycosedation and pain and anxiety control. Patients with a history pf Rheumatic heart disease should be premedicated with amoxicillin , erythromycin or clindamycin, as per the current “American heart association guidelines”
American heart association guidelines”
TECHNIQUES FOR CLEANING AND SHAPING USED IN SINGLE VISIT.
POST OPERATIVE PAIN AND FLARE UP IN SINGLE VISIT ENDODONTICS v There is a ‘myth’ that single visit endodontic treatment causes more post operative discomfort and flare up rates to the patients. Most studies show that single visit root canal procedures produce no more pain than multiple visit ones. v In 1970, Fox and co-workers have found that only 7% single visit cases reported of severe pain in 24 hours. They found that 90% of the teeth were free of spontaneous pain after 24 hours. v Wolch in 1970 treated 500 non vital cases in single visit and he found severe pain in only 5% of patients. Many more studies have shown the success of single visit which is comparable to multiple visit treatment. v ‘Morese’ defines “Flare - up” as swelling and pain combined or swelling above that necessitates unscheduled emergency appointments. v ‘Wolton’ defines “Flare-up” within a few hours to a few days after a root canal treatment procedure, a patient has either pain or swelling or combination of both.
According to the findings of Trope (Int-Endo J. 1991) Teeth without apical periodontitis did not flare up and may be treated in a single visit. Teeth with apical periodontitis but no previous root canal treatment can be treated in single visit, with a low probability of a flare-up occurring. In teeth with apical periodontitis which need retreatment, the flare up rate was highest and single visit root canal treatment would be inadvisable.
Oliet, 1970 (J. of Oral Surgery) Found that 90% of success was achieved in single visit treated teeth. This was comparable to multiple visit treated teeth. He found that overfilling of the root canals of teeth treated in a single visit resulted in moderate to severe pain in 255 of cases, younger patients aged 10 to 39 years, had significantly more pain than older patients. SUCCESS RATES AND FAILURE OF SINGLE VISIT Prognostic studies have shown that there is no substantial difference in the success rate of single and multiple appointment cases. Alkenaz claimed that single appointment root canals succeeded 97% of time comparable to multiple visit. Pekruhum in a study J. of Endodontics 1986 found a failure of only 5. 2% in single visit cases. He noted that teeth not previously opened showed three times the number of failures as those that had been previously opened. This was especially true of teeth involved with periapical extension of pulpal disease. The success is more in the cases where combination of hand instrumentation and ultra sonic techniques are utilized.
SURVEY RESULTS v After the survey, it was found that single visit endodontics was taught in 85. 7% of dental schools. In 1982. v In 1990 Survey of 568 dentists, reported that 35% would complete cases in one visit for teeth with normal periapex whereas only 16% would do so when apical periodontitis was present. Fewer than 10% of the dentists would complete a non vital cases in single visit. v But, the trend is changing now as many endodontist prefer single visit endodontics treatment for patients keeping the indications of single visit in mind. ONE VS. SEVERAL VISITS In recent years, a most heated discussion has emerged as to the need for more than one treatment session in endodontics. Traditionally, treatment has been divided into two or more appointments before the placement of a permanent filling, allowing the clinician to enhance root canal disinfection, to increase patient comfort, and to observe the progress of healing (Trope and Bergenholtz, 2002). Unfortunately, the arguments for the number of patient visits are often unclear.
When one carefully considers the case selection criteria from advocates of one-visit treatments, it becomes clear that there are many exclusion criteria which are not articulated in the debate. • Ashkenaz (1984) suggested that multi-rooted teeth should be excluded. • Pekruhn (1986) limited the inclusion criteria to "teeth in my practice, which could be conveniently treated in a single visit". • Roane et al. (1983) stated that decisions on the use of single- or multiple-visit treatment were based solely on the time available for treatment.
In conclusion multiple visit and single visit root canal treatment demonstrated almost equal success. Briefly, in cases of vital pulp, a single-visit treatment should be used whenever possible. This is based on the fact that the pulp is only superficially infected and the root canal is free of bacteria, provided the aseptic procedures is maintained during root canal treatment. Therefore, there is no apparent reason not to treat vital pulps in a single visit. Conversely, if the pulp is necrotic and/or associated with a periradicular disease, there is ample evidence that the root canal system is infected. In these cases, the root canal system should ideally be cleaned and shaped, an intracanal medication placed, and the canal filled at a second appointment. One visit endodontic should be viewed as a procedure relates to endodontics and not as a technique that is going to totally replace multivisit procedures. Both single and multivisit treatments should be viewed as part of a total endodontic treatment spectrum, with the choice of one over the other being determined by the circumstances surrounding each individual case. The practitioner should not routinely apply one technique to all situations, but rather evaluate the circumstances peculiar to each particular case and then choose the technique that best fits those circumstances. However, when doubt exists, the multiple visit procedure should be performed. Thus, the clinician will be most effectively utilizing his time in delivering the best possible endodontic service available to the patient that supplements and complements total patient care
The major objective in endodontic treatment is to remove all necrotic and vital organic tissue, some hard tissue including dentin chips created by instrumentation, to kill microorganisms, and give the canal system a shape that facilitates ideal irrigation, debridement , and three-dimensional obturation and finally a placement of functional and esthetic permanent restoration during the lifetime of the suffering teeth.
Clinical Classification of Pulpal and Periapical Diseases Because there is little or no correlation between the histologic findings of pulpal pathosis and clinical symptoms, the diagnosis and classification of pulpal diseases are based on clinical signs and symptoms (the objective and subjective findings ) rather than histopathologic findings. Because removal of the questionable pulpal tissue for histologic examination is not practical, clinical classifications have been developed in order : v to indicate the status of the tissue healthy or diseased tissue and v to formulate treatment plan options.
CLASSIFICATION OF PULPAL DISEASES Pulpal conditions can be classified as normal pulp reversible irreversible pulpitis, symptomatic or asymptomatic previously treated. Previously Initiated Therapy Hard tissue responses include calcification and resorption.
Apical ( Periapical ) Disease Normal Periapical Tissues Symptomatic Apical Periodontitis ( SAP ) Asymptomatic Apical Periodontitis (AAP) Condensing Osteitis Acute Apical Abscess Chronic Apical Abscess
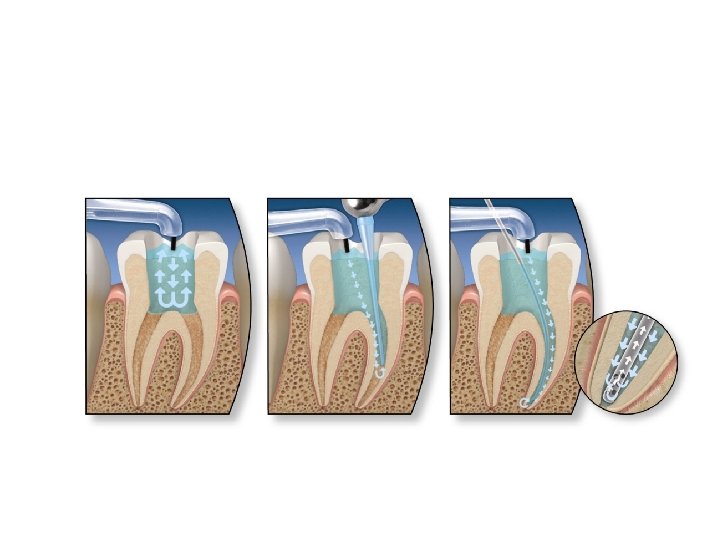
WHY DO WE NEED IRRIGATION ? COMPLEX root canal system Mechanically → IMPOSSIBLE The only way → IRRIGATION
A-C: Open-ended needles; (A) flat, (B) beveled & (C) notched. D-F: Closed-ended needles; (D) side-vented, (E) double sidevented & (F) multi-vented. 24
Navi. Tip FX 26
Endo. Activator q is a new type of irrigation system. It is based on sonic vibration (up to 10, 000 rpm) of a plastic tip in the root canal. q The system has 3 different sizes of tips that are easily attached (snapon) to the handpiece that creates the sonic vibrations the use of Endo. Activator facilitates irrigant penetration and mechanical cleansing compared with needle irrigation, with no increase in the risk of irrigant extrusion through the apex.
Endo. Ultra by Vista Dental Dr Abdussalam Salem Elsanfaz
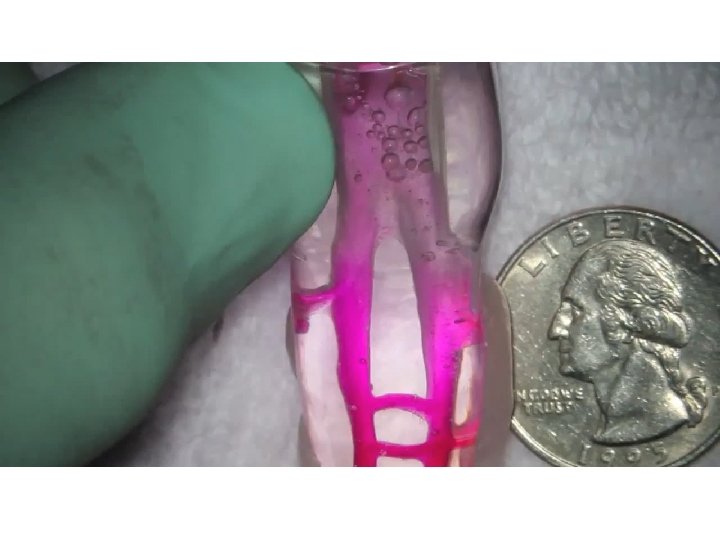
Pressure alternation devices (negative-pressure irrigation) v Rins. Endo v Endo. Vac v Self adjusting file (SAF) 29
Rins. Endo 30
Endo. Vac the Endo. Vac system is based on a negative-pressure approach whereby the irrigant placed in the pulp chamber is sucked down the root canal and back up again through a thin needle with a special design
Ultrasound • Contribute better cleaning system ran irrigation and hand instrumentation alone • Effective to cases with complex anastomoses canal system • Less preparation complication with ultrasonic files
Acoustic microstreaming and cavitation: Ø Acoustic stream can be defined as a rapid movement of the fluid in a circular or vortex shape around the vibrating file. Ø Cavitation is defined as the creation of steam bubbles or expansion, contraction and/or distortion of pre-existing bubbles in a liquid. 34
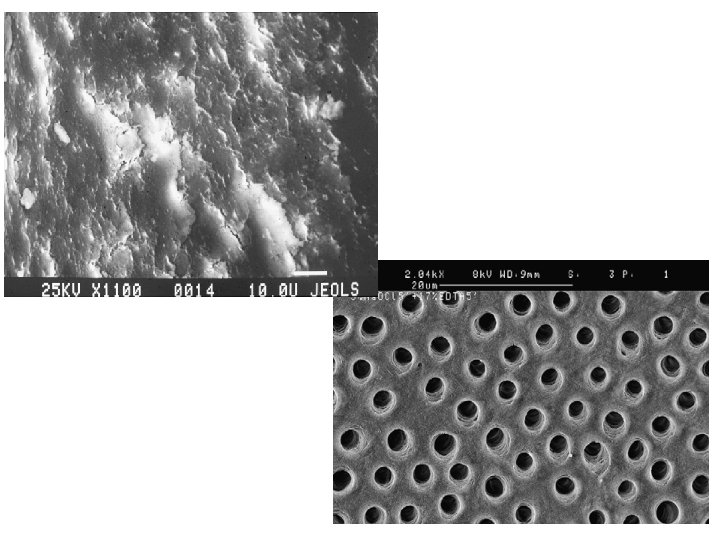
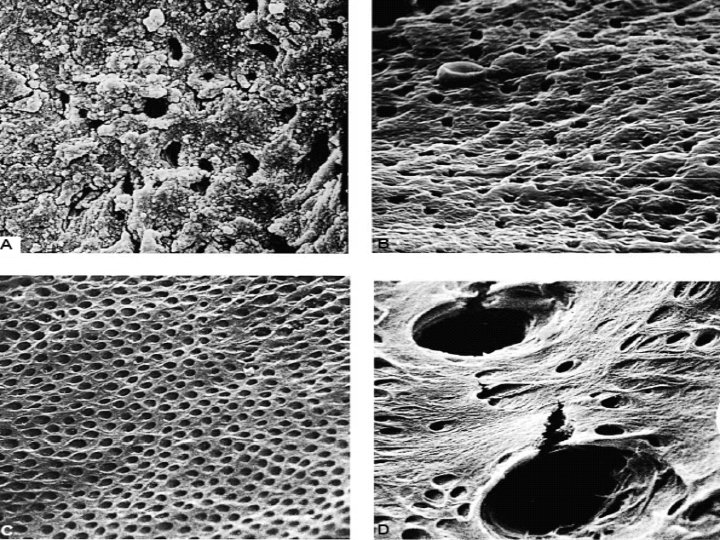
Cross section of root dentin covered by the smear layer created by instrumentation. Notice smear plugs in dentin canals
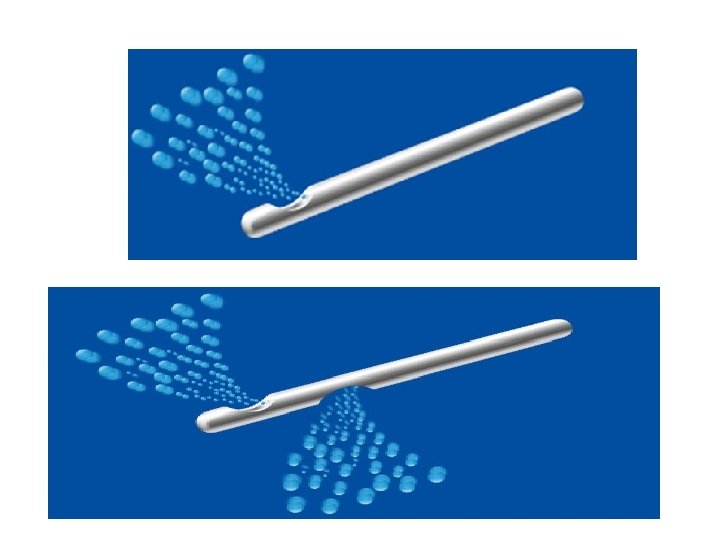
v The irrigant doesn't move apically more than 1 mm beyond the irrigation tip. v The closer the needle tip to the apex, the greater the potential for damage to the periradicular tissues. v * The volume of irrigant is more important than the concentration or type of irrigant. v The apical 5 mm are not flushed until they have been enlarged to size 30 and more often size 40 file. v The importance of recapitulation–re-instrumentation with a smaller instrument following each irrigation. 38
Manual-dynamic irrigation Ø It is often difficult for the irrigant to reach the apical portion of the canal because of the vapor lock effect. Ø Gently moving well-fitting gutta-percha master cone up and down in short 2 to 3 mm strokes (manual-dynamic irrigation) within an instrumented canal: * can produce an effective hydrodynamic effect * can force the irrigant to the untouched canal surfaces. 39
Self Adjusting file (SAF), rotary system. v It adjusts to the anatomy of the root canal. v It has a hollow thin walled cylinder composed of a thin nickel-titanium lattice. v Provides continuous irrigation during instrumentation. v In oval canals, the SAF was found superior to rotary Ni-Ti files used with needle irrigation (Na. OCl). v SAF is designed to prepare root canals that do not have a round cross section. v It has an abrasive surface. v Up & down movement (vibration) during rotation. 40
Self adjusting file (SAF) 41
42