Control and regulation of GFR and renal blood

Control and regulation of GFR and renal blood flow • Sympathetic nervous system activation _decreases_ GFR. – Strong activation of renal sympathetic nerves can constrict the renal arterioles and decrease renal blood flow and GFR. • Only strong activation due to brain ischemia or hemorrhage. – Mild activation has insignificant effect.

Control and regulation of GFR and renal blood flow • Hormonal and autacoid control of renal circulation. • Norepinephrine, and endothelin constrict renal blood vessels and decrease GFR. • Angiotensin II constricts efferent arterioles which helps to prevent a decrease in glomerular hydrostatic pressure and GFR. – Decreased arterial pressure or low blood volume induce angiotensin II production. » These effects normally decrease GFR • Endothelial-derived NO decreases renal vascular resistance (induces dilation) and increases GFR. • Prostaglandins increase renal blood flow and increase GFR.

Autoregulation of GFR and renal blood flow • Mechanisms which maintains renal blood flow and GFR relatively constant despite changes in arterial blood pressure. • Myogenic Mechanism • Tubuloglomerular Feedback Mechanism. Sherwood’s Human Physiology 14 -12 5 th Ed. & 14 -11 6 th Ed.

Autoregulation of GFR and renal blood flow Sherwood’s Human Physiology 14 -12 5 th Ed. & 14 -11 6 th Ed.

Autoregulation of GFR and renal blood flow • Myogenic Mechanism of GFR – Smooth muscle cells in the afferent arteriole respond to changes in vascular pressure – Increase in arterial pressure leads to _constriction – Decrease in arterial pressure leads to _relaxation_ Sherwood’s Human Physiology 14 -12 5 th Ed. & 14 -11 6 th Ed.

Autoregulation of GFR and renal blood flow • Tubuloglomerular Feedback Mechanism. – Involves the Juxtaglomerular complex which is made up of juxta- glomerular cells from the afferent & efferent arterioles and specialized epithelial cells in the distal tubule called the macula densa. Sherwood’s Human Physiology 14 -12 5 th Ed. & 14 -11 6 th Ed.

Autoregulation of GFR and renal blood flow • Tubuloglomerular Feedback Mechanism. – Juxtaglomerular cells (JG cells) • Mechanoreceptors • Modified smooth muscle cells that secrete renin • Leads to efferent arteriole constriction Sherwood’s Human Physiology 14 -12 5 th Ed. & 14 -11 6 th Ed.

Autoregulation of GFR and renal blood flow • Tubuloglomerular Feedback Mechanism. – The macula densa senses changes in the Na+ & Cl - content in the distal tubule which can be related to the flow rate through the tubule. • Chemoreceptors – A decreased flow rate results in less Na+ & Cl- in the proximal tubules and therefore less would be present in the distal tubule. Sherwood’s Human Physiology 14 -12 5 th Ed. & 14 -11 6 th Ed.

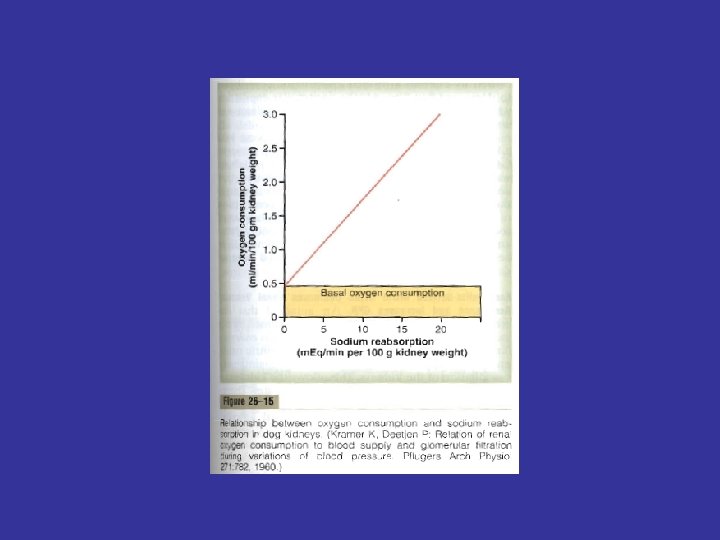
Tubuloglomerular Feedback Mechanism. ↓ Arterial pressure • Decreased Arterial Pressure or Decreased concentration of Na. Cl at the macula densa results in dilation of the afferent arterioles and increased renin release to increase the GFR back to normal. Guyton’s Textbook of Medical Physiology 26 -15 ↓ Glomerular Hydrostatic pressure ↓ GFR ↓ Macula Renin densa Na. Cl Angiotensin II efferent arteriole resistance afferent arteriole resistance

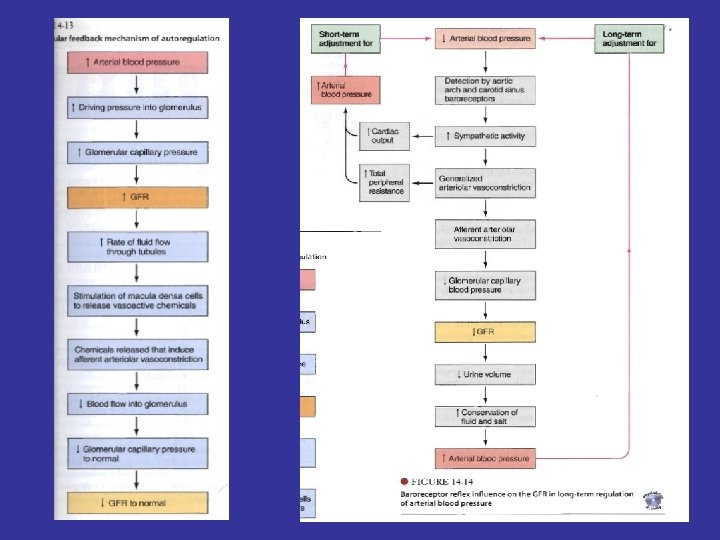
Tubuloglomerular Feedback Mechanism. • Increased Arterial Pressure or Increased concentration of Na. Cl at the macula densa results in constriction of the afferent arterioles decrease the GFR back to normal. ↑ Arterial pressure ↑ Glomerular Hydrostatic pressure ↑ GFR ↑ Macula densa Na. Cl Afferent arteriole constriction ↓ GFR hydrostatic pressure ↓ GFR to Normal Sherwood’s Human Physiology 14 -13 5 th Ed. & 14 -12 6 th Ed.

Tubular Reabsorption • For a substance to be reabsorbed it must first be transported across the tubular epithelial membrane into interstitial space and then through the peritubular capillary membrane into the blood. Sherwood’s Human Physiology 14 -17 5 th Ed. & 14 -14 6 th Ed.

Tubular Reabsorption • Water and solutes are transported via: – Transcellular route – Paracellular route – Bulk flow into the bloodstream Guyton’s Textbook of Medical Physiology 27 -1

Tubular Reabsorption – Transcellular route • Substance needs to traverse 5 distinct barriers – Paracellular route • Substance needs to traverse 3 distinct barriers Sherwood’s Human Physiology 14 -17 5 th Ed. & 14 -14 6 th Ed.

Tubular Reabsorption • Passive transport – Due to electrical and chemical gradient (Urea and Cl-) • Osmosis • Active transport – Primary active transport Na+- K+-ATPase. • Pinocytosis – Especially for reabsorption of proteins. Guyton’s Textbook of Medical Physiology 27 -1 & Sherwood’s Human Physiology 14 -18 5 th Ed & 14 -15 6 th Ed
- Slides: 16