Contraception Dr K Dissanayake Bute House Medical Centre

Contraception Dr K Dissanayake Bute House Medical Centre

Different Methods § Hormonal § Barrier methods § IUD § Natural methods § Sterilisation

Things to consider § Age, consider whether Fraser competent in <16 yrs § Medical History – UKMEC / WHOMEC § Current medications § Menstrual cycle § Patient preference – previous experience, hormonal/nonhormonal, amenorrhoea § Efficacy § Quick starting


Table 4: Percentage of women experiencing an unintended pregnancy within the first year of use with typical use and perfect use (modified from Trussell et al. ) Method Typical use (%) Perfect use (%) Fertility awareness-based methods 24 0. 4– 5 Male condom 18 2 Combined hormonal contraception (CHC) Progestogen only pill (POP) 9 0. 3 Implant 0. 05 DMPA 6 0. 2 Cu-IUD LNG- IUS 0. 8 0. 2 0. 6 0. 2 Female sterilisation Vasectomy 0. 5 0. 15 0. 1

UKMEC criteria § Provides guidance who can use the contraceptive methods safely – related to safety not efficacy UKMEC Definition 1 A condition for which there is no restriction of use of the method 2 A condition where the advantages of using the method generally outweigh theoretical or proven risks 3 A condition where theoretical or proven risks usually outweigh the advantages. Expert clinical judgement or referral advised 4 A condition which represents and unacceptable health risk if the method is used
 § Ulipristal (Ella One) § Copper IUD")
Emergency Contraception § Levonorgestrel (Levonelle) § Ulipristal (Ella One) § Copper IUD
 or decreasing levels (Cat. 3) for")
Considarations § Persistently elevated b-HCG levels (category 4) or decreasing levels (Cat. 3) for Cu-IUD § Post partum < 4 week and distorted uterus are category 3 for Cu-IUD

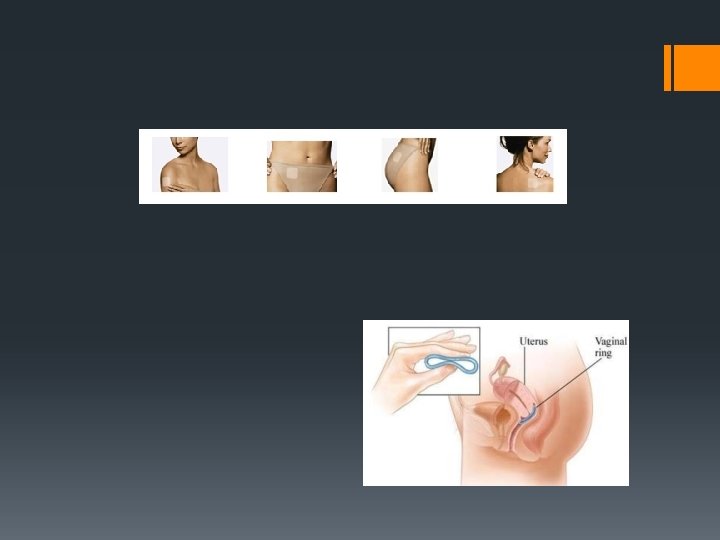
Hormonal contraception § Combined hormonal contraception 1. COC a. First line - Ethinylestradiol 30 mcg +levonorgestrel or Norethisterone – eg Microgynon, Rigevidon. b. Higher risk of VTE if the progestogen is Drospirenone (Yasmin), Gestodene (Femodene) and Desogestrel (Marvelon/Gedarel) 2. 3. Transdermal patches –eg Evra Vaginal ring - Nuva. Ring

CHC § Mechanism of action – Inhibition of ovulation, some effect on the cervical mucus and endometrium. § When to start § Missed pills 1. 2. One missed pill 2 or more missed pills § Diarrhoea and vomiting
 and breastfeeding – category 4 §")
CHC and UKMEC § Postpartum (0 -<6 weeks) and breastfeeding – category 4 § Post partum (3 -6 weeks) and non breast feeding 1. 2. With other risk factors for VTE – category 3 Without other risk factors for VTE – category 2 § Age and smoking 1. 2. <35 yrs – category 2 >35 yrs - <15 cigarettes – cat. 3 and >15 cig cat. 4

CHC and UKMEC § Obesity 1. 2. BMI >= 30 -34 Cat. 2 BMI>= 35 Cat. 3 § Hx of or current VTE – Cat. 4

Progestogen only contraception 1. POP 2. Depo injections 3. Subdermal implant UKMEC Current breast cancer Cat 4, past breast cancer Cat 3 Check if hx of stroke and IHD 4. IUS
, suppression")
POP § Mechanism of action – changes to cervical mucus, suppression of ovulation(Desogestrel>norgeston), suppression of midcycle peaks of LH and FSH, hostile endometrium, reduced activity of cilia in the fallopian tube § When to start § Delayed or missed pills § Vomiting and diarrhoea
 2.")
LARC § Progestogen only injections 1. Depot medroxyprogesterone acetate 150 mg deep IM(depoprovera) 2. Depot medroxyprogesterone acetate 104 mg SC (Sayana Press) 3. Norethisterone enantate 200 mg deep IM (Noristerat) § Subdermal implant § IUS § IUD

Progestogen only injectables

Progestogen only injectables § Mechanism of Action – Inhibition of ovulation and thickening of cervical mucus § When to start § Depo Provera – every 12 weeks and Sayana Presss – every 13 weeks § Loss of bone mineral density

Progestogen only implant § Nexplanon – Etonogestrel 68 mg

Nexplanon § Mechanism of Action – Inhibition of ovulation, some changes to cervical mucus § When to start § 3 years § Menstrual irregularities § Liver enzyme inducing drugs are likely to reduce efficacy § Deep implants/migration of implant

IUS § Levonorgestrel intrauterine systems Mirena Levosert Jaydess Dose 52 mg 13. 5 mg Contraception 5 yrs 3 yrs Endometrial protection 4 yrs - - Menorrhagia 5 yrs 3 yrs - size 32 mm(h) 32 mm(w) 30 mm(h) 28 mm(w)

Mirena

IUS § Mechanism of Action – prevents implantation of the fertilised ovum and changes to cervical mucus § When to start

IUD § Copper containing devices § Most effective devices contain at least 380 mm 2 of copper and have copper bands on the transverse arms.

IUD § TT 380 Slimline – 10 years § Mini. TT 380 Slimline – 5 years § T-Safe 380 A QL – 10 years

IUD § Mechanism of Action 1. 2. 3. Toxic to the sperm and ovum thereby preventing fertilisation Alteration in the copper content of the cervical mucus – inhibits penetration Inflammatory reactions within endometrium – prevents implantation § When to start § Heavier and more painful periods

IUS/IUD § Risk of Uterine Perforation – 1/1000 § Risk of PID – related to insertion and background risk of STI § Educate patient to feel for threads § Risk of ectopic pregnancy § Actinomyces like organisms on smear

Permanent methods § Sterilisation • Vasectomy • Tubal Occlusion

Vasectomy § Minor surgical procedure § Small risk of haematoma and infection § Potentially irreverisible § Need to use contraception for 12 weeks post procedure until azoospermia in confirmed § Risk of testicular/scrotal pain post vasectomy – can develop months or years later. 1 -14%

Vasectomy

Tubal Occlusion § Surgical procedure § Potentially irreversible § If tubal occlusion fails the resulting the pregnancy might be ectopic § Filshie clips and modified Pomeroy technique – contraception for 4 weeks following the procedure § Hysteroscopic sterilisation – need contraception for 3 months until confirmation of occlusion

Tubal Occlusion
- Slides: 32