CONTEMPORARY STANDARDS IN TREATMENT OF CHRONIC HEART FAILURE


 is Common- 2% of the population n")
 is the inability of the heart to")

























 Highly variable kinetics + VERY narrow therapeutic index = need to")


 anorexia abdominal discomfort vomiting diarrhea")

 • Potassium (if")

- Slides: 70
CONTEMPORARY STANDARDS IN TREATMENT OF CHRONIC HEART FAILURE JERZY JANKOWSKI MD DEPARTMENT OF CLINICAL PHARMACOLOGY
http: //www. zfk. ump. edu. pl/
Key issues in Chronic Heart Failure (CHF) is Common- 2% of the population n Dangerous- high mortality n Disabling- high morbidity n Costly- 2% of health care budget n Treatable- very successful pharmocological therapy developed n
Definition of CHF n Heart failure (HF) is the inability of the heart to maintain an output adequate to meet the metabolic demands of the body. n Definition of HF I. Symptoms and signs of heart failure (at rest or during exercise) and II. Objective evidence (preferably by echocardiography) of Cardiac dysfunction (systolicand/ordiastolic) (at rest) and (in cases where the diagnosis is in doubt) and III. Response to treatment directed towards heart failure *Criteria I and II should be fulfiled in all cases.
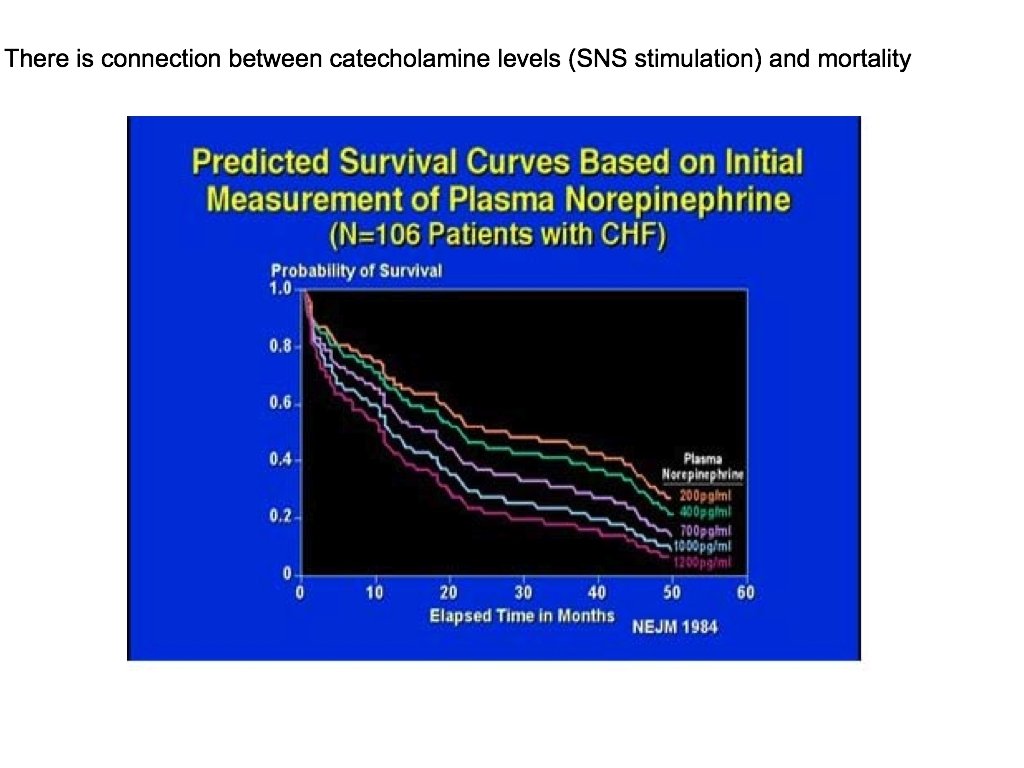
Pathophysiology of Heart Failure Autonomic and hormonal control of cardiovascular function
Pathophysiology of Heart Failure
Pathophysiology of Cardiac Performance Cardiac performance is a function of 4 factors PRELOAD AFTERLOAD CONTRACTILITY HEART RATE
Preload
Diuretics in Heart Failure Loop diuretics: furosemide, torsemide Thiazide and thiazide-like diuretics: hydrochlorothiazide chlorthalidone + K sparing diuretics: + Na channel inhibitors: amiloride, triamterene Aldosteron antagonists: spironolactone, eplerenone
Diuretics in Heart Failure
Loop Diuretics Furosemide, torsemide, ethacrinic acide, torsemide Secreted into the tubular fluid by proximal tubule cells
Loop Diuretics: Side Effects and Drug Interaction n n n Volume depletion, hyponatremia, hypokalemia Hypocalcemia, hypomagnesemia, hypochloremia Ototoxicity – especially with ethacrynic acid Hypotension Metabolic effects – hyperuricemia, hyperglycemia, hypercholesterolemia (↑LDL, ↓HDL, ↑TGL) Cardiac glycosides (risk of ventricular arrhythmias) Aminoglycoside antibiotics, cisplatin (risk of ototoxicity)
Loop Diuretics: Drug Interaction n NSAIDs – reduced effects n Probenecid – blocks secretion into the distal tubule and decreases the response to the LD
Thiazide Diuretics Hydrochlorothiazide – the prototype for this class of drugs n Thiazide-like – chlorthalidone, indapamide and metolazone (long acting diuretics) n The same mechanism of action n
Thiazide Diuretics – Side Effects Electrolyte abnormalities – hypokaliemia, hyponatremia, hypercalcemia, hypomagnesemia, hypochloremia, hypovolemia n Hyperuricemia, hyperglycemia (reduced effecacy of hypoglycemic drugs n Increased plasma levels of LDL and TGL n Sexual dysfunction n Cardiac arrhythmias n Drug interactions – as loop diuretics n
Aldosterone Antagonists
Aldosterone Antagonists
Aldosterone Antagonists
Aldosterone Antagonists RALES TRIAL
RALES TRIAL
Aldosterone Antagonists EPHESUS TRIAL
EPHESUS TRIAL
EPHESUS TRIAL
EPHESUS TRIAL
EPHESUS TRIAL
EPHESUS TRIAL
Cardiac glycosides
Cardiac glycosides – mechanism of action
Pharmacokinetics (Digoxin, Digitoxin) Highly variable kinetics + VERY narrow therapeutic index = need to individualize dose regiments Relatively long half-lives of elimination accumulation to stedy state loading doses employed delays following changes in therapy
Pharmacokinetics Plasma concentration determinations Effective range = 1. 0 – 2. 5 ng/ml Toxic range = 1. 5 – and up Rarely essential to a diagnosis of toxicity Estimate of degree of overdose Can be used to calculate dose adjustments
Comparative Pharmacokinetics
Toxicity Gastrointestinal (relate to vagal effects) anorexia abdominal discomfort vomiting diarrhea
Toxicity Cardiac disturbances premature ventricular depolarization nodal rhytms A – V dissociation
Treatment of Toxicity • Stop giving the drug (for a time) • Potassium (if hypokalemic) • Cholstyramine, activated charcoal (to bind digoxin in GI tract and shorten half-life ) • Digoxin Antibodies (Fab fragments) • Antiarrhythmics (very cautiously) • Electrotherapy (defibrillation only in the case of VF
Drug Interactions • Increased plasma concentration – verapamil, diltiazem, quinidine, amiodaron, spironolacton • Changes in plasma electrolyte – diuretics, salts (K+, Ca++), adrenocorticoids • Changes in digoxin absorption – antacids, cholestyramine, laxatives, antidiarrheal absorbents • Changes in cardiac cell activity sympathomimetics