Consumer Involvement in Guideline Development Why Every Guideline

")


 Composition")













 with Middle Ear Effusion (MEE)")


- Slides: 25
Consumer Involvement in Guideline Development Why Every Guideline Needs It Richard M. Rosenfeld, MD, MPH Professor and Chairman of Otolaryngology, SUNY Downstate Senior Consultant for Guidelines and Quality, AAO-HNS Chair Emeritus, Guidelines Int’l Network – North America
Who are we? AAO-HNS The American Academy of Otolaryngology— Head and Neck Surgery (AAO-HNS) is the world's largest organization representing specialists who treat the ear, nose, throat, and related structures of the head and neck. The Academy represents more than 12, 000 otolaryngologist—head and neck surgeons who diagnose and treat disorders of those areas. Headquarters in Alexandria, VA EMPOWERING PHYSICIANS TO DELIVER THE BEST PATIENT CARE
AAO-HNS Guideline Usage Summary National Guideline Clearinghouse & Google Scholars Guideline title Date released Page views (NGC) 8/14 Citations (GS) 8/14 Acute otitis externa 7/14/06 102, 556 128 Adult sinusitis 8/22/08 61, 861 611 Cerumen impaction 4/17/09 49, 353 66 Benign paroxysmal positional vertigo 4/17/09 57, 630 299 Hoarseness (dysphonia) 4/23/10 46, 048 122 Tonsillectomy in children 3/15/11 48, 594 196 PSG for SDB prior to tonsillectomy in children 12/1/11 32, 324 63 Sudden hearing loss 4/1/12 42, 726 108 Improving voice outcomes after thyroid surgery 6/1/13 8, 445 27 Tympanostomy tubes in children 7/1/13 8, 662 34 11/4/13 6, 043 9 464, 242 1, 663 Bell’s palsy TOTAL
83 Standards 20 Standards Institute of Medicine 2001 – http: //www. iom. edu
Standards for Developing Trustworthy Clinical Practice Guidelines Standard 3. Guideline Development Group (GDG) Composition 3. 2 Patient and public involvement should be facilitated by including (at least at the time of clinical question formulation and draft CPG review) a current or former patient, and a patient advocate or patient/consumer organization representative in the GDG http: //www. iom. edu/Reports/2011/Clinical-Practice-Guidelines-We-Can-Trust/Standards. aspx
www. g-i-n. net
Ann Intern Med 2012; 156: 525 -531
Begin with the End in Mind Habit #2, Stephen Covey Consumers Covey S. The 7 Habits of Highly Effective People. Fireside Press, 1989
Begin with the End in Mind Habit #2, Stephen Covey Consumers X Consumers do not have to be content experts! (the same applies to clinicians)
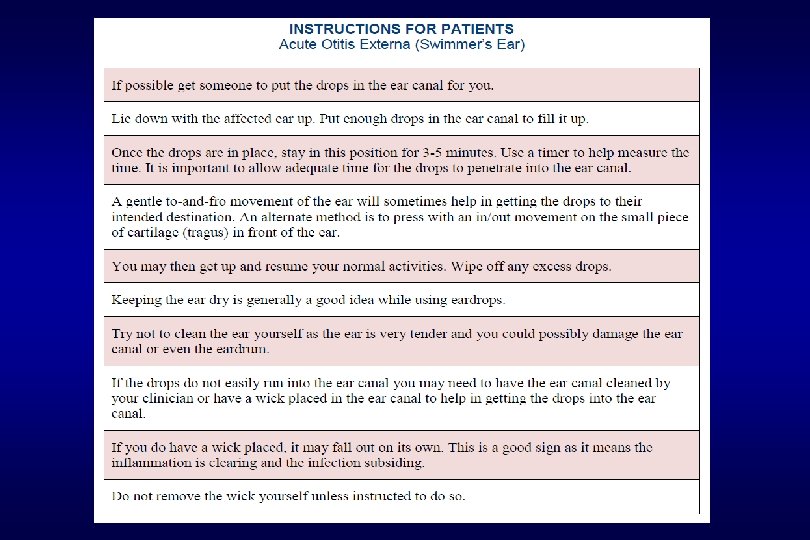
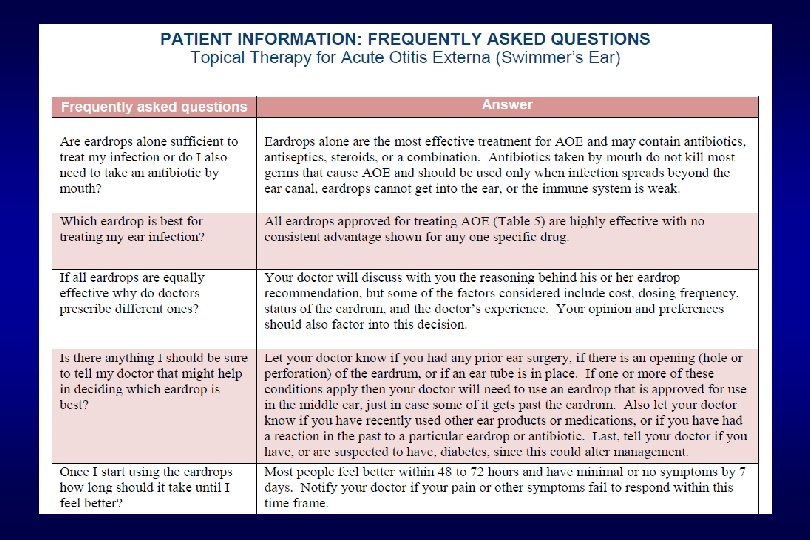
AAO-HNS Guideline Action Statements with Strong Consumer Influence n The clinician should advocate for pain management after tonsillectomy and educate caregivers about the importance of managing and reassessing pain. n The clinician should educate the patient about the potential impact of thyroid surgery on voice once a decision has been made to have surgery. n Clinicians should educate patients with idiopathic sudden sensorineural hearing loss about the natural history of the condition, the benefits and risk of interventions, and the limitations of existing evidence regarding efficacy. n In the perioperative period, clinicians should educate caregivers of children with tympanostomy tubes regarding the expected duration of tube function, recommended follow-up schedule, and detection of complications. n Clinicians should inform patients how to administer topical drops for acute otitis externa (swimmer’s ear). Source: AAO-HNS Clinical Practice Guidelines
Post-Tonsillectomy Pain Management Education for Caregivers 1. Throat pain is greatest the first few days and may last up to 2 weeks 2. Encourage your child to tell you if he or she has throat pain since pain may not always be expressed or recognized promptly 3. Make sure your child drinks plenty of fluids after surgery. Staying well hydrated is associated with less pain. 4. Ibuprofen can be used safely for pain control after surgery. 5. Many clinicians recommend not waiting until your child complains of pain. Instead, the pain medication should be given on a regular schedule. 6. Expect your child to complain more about pain in the mornings; this is normal. Call your health care provider if you are unable to adequately control your child’s pain. AAO-HNS Tonsillectomy CPG. Otolaryngol Head Neck Surg 2011; 14(Suppl): S 1 -S 30
Clinical Infectious Diseases Advance Access, September 9, 2012
Sir William Osler Canadian Physician, 1849 -1919 Common sense in medical matters is rare, and is usually in inverse ratio to the degree of education.
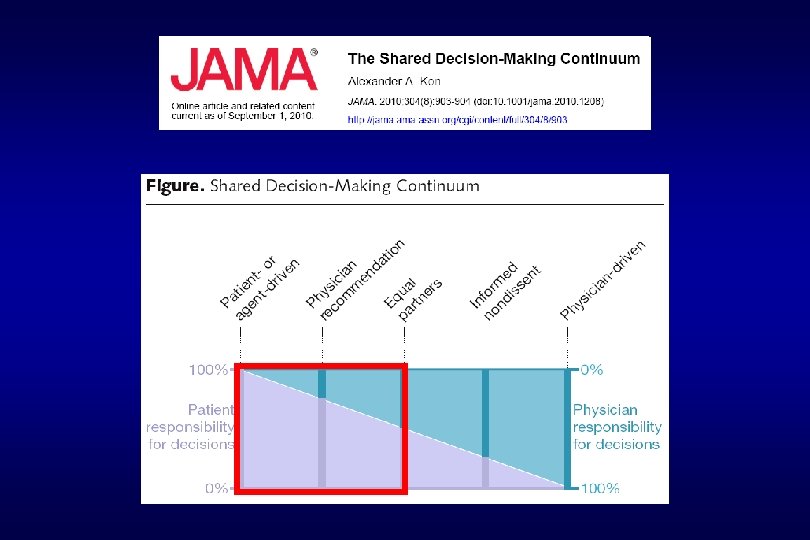
Consumer Involvement in Guidelines What are the Possibilities? What do Consumers contribute to GDGs? Passion Perspective Skepticism Respect for harms Patient education Shared decisions
Arch Intern Med 2012; doi: 10. 1001/2013. jamaintermed. 56
Barriers to Capacious, Non-Foreclosed Thought Rita Charon, MD, Ph. D Director, Narrative Medicine Program, Columbia, University Lack of Time Habits and Routines Narrow Range of Thought Fear of Novelty & Uncertainty Foreclosed = rule out or prevent (a course of action)
Policy Statements as Behavior Constraints Policy strength Implication for clinicians Pt. preference Strong recommendation Follow unless a clear and compelling rationale for alternative approach is present Limited role Recommendation Generally follow a recommendation, but remain alert to new information Should be considered Option Be flexible in decision making regarding appropriate practice, although bounds may be set on alternatives Substantial influencing role No recommendation Feel little restraint in decision making and be alert to new published evidence that clarifies the balance of benefit vs. harm Substantial influencing role Pediatrics 2004; 114: 874 -877
Key action statement with recommendation strength and justification Action statement profile: Ø QI opportunity: Ø Aggregate evidence quality: Ø Confidence in evidence: Ø Benefit: Ø Risk, harm, cost: Ø Benefit-harm assessment: Ø Value judgments: Ø Intentional vagueness: Ø Role of patient preferences: Ø Differences of opinion: Ø Exclusions: Action Statement Profiles and Guideline Development 1. Encourage an explicit and transparent approach to guideline writing 2. Force guideline developers to discuss and document the decision making process 3. Create “organizational memory” to avoid re-discussing already agreed upon issues 4. Allow guideline users to rapidly understand how and why statements were developed 5. Facilitate identifying aspects of guideline best suited to performance assessment
Tympanostomy Tube CPG AAO-HNS Recurrent Acute Otitis Media (AOM) with Middle Ear Effusion (MEE) Clinicians should offer bilateral tympanostomy tube insertion in children with recurrent AOM who have unilateral or bilateral MEE at the time of assessment for tube candidacy. Recommendation based on RCTs with minimal limitations and a preponderance of benefit over harm. • Benefits: Mean decrease of about 3 episodes of AOM per year; ability to treat future episodes with topical antibiotics instead of systemic; reduces pain with future AOM • Level of confidence in evidence: Medium; some uncertainty regarding the magnitude of clinical benefit, because of heterogeneity in the design and outcomes of trials • Value judgments: In addition to the benefits seen in RCTs, the presence of effusion at the time of assessment served as a marker of diagnostic accuracy for AOM • Role of patient preferences: Substantial role for shared decision making regarding the decision to proceed with, or to decline, tympanostomy tube insertion Otolaryngol Head Neck Surg 2013; 149(Suppl): S 1 -35 EMPOWERING PHYSICIANS TO DELIVER THE BEST PATIENT CARE
Plain Language Guideline Summaries What Belongs in Patient and Consumer Versions? 1. 2. 3. 4. 5. Statement of purpose Description of how guideline was developed and to whom it applies Definitions, diagnostic criteria, natural history, prognosis Summary of key action statements (recommendations) Decision aids, especially when role for shared decisions is significant 6. Comparisons of harms and benefits for main treatment alternatives 7. Instruction aids, self-care advice 8. Information to help patients navigate the health care system Inspired by: Santesso NAM. Dissemination of Clinical Practice Guidelines to Patients and the Public. Graduate Thesis; Mc. Master University, 2014
An Educated Consumer…Can be the Best Member of a Guideline Development Group The challenge is now for the medical profession to…develop alliances with consumers to move forward toward a wider recognition of the uncertainty and weaknesses of medicine and the biases in the process of setting research priorities. Alessandro Liberati BMJ 1997; 315: 499 Thank You for Your Kind Attention! Richard M. Rosenfeld, MD, MPH – richrosenfeld@msn. com