Connecticut Long Term Care Mutual Aid Plan LTCMAP
 Leadership Education RPA Support Team: Scott")

 (Evacuation: May 2006 / Recovery: Sept. 2006) Source: Boston")




 • Sign it - Transfer Agreements with")
 (Located in Annex I of the plan) • • The")

 receives the resident: • • Do")

, DSS (Medicaid)")





 Provides Public Health, Fire, EMS and Emergency")










")
 HANDOUT Operational")

 Coordinating Center § Region 1: Lord Chamberlain (Stratford) / Back-up:")


- Slides: 41
Connecticut Long Term Care Mutual Aid Plan (LTC-MAP) Leadership Education RPA Support Team: Scott Aronson Lori Cheever Andy Mc. Guire Jim Garrow Darren Osleger
What Led to Mutual Aid in New England: Learning from experiences in: • • • NY State – 1 st Plan (began in 1983) 2001 Tropical Storm Alison (Houston) 2001 9/11 2005 Hurricanes Katrina / Rita Massachusetts Disasters (1 st New England State) • • May 2006 Flooding (Mother’s Day Storm) November 2006 Chemical Explosion (Danvers) 2008 Ice Storm in Central & Western MA
Mary Immaculate Evacuated (250 beds) (Evacuation: May 2006 / Recovery: Sept. 2006) Source: Boston Globe. com
Other Incidents where Mutual Aid Plans were Activated § § § § Aug/Sept 2011 - Tropical Storm Irene/Lee Flooding Oct/Nov 2011 - “Halloween Storm” - Snowstorm/ Power Failure July 2012 – MA Nursing Home Generator Failure (Region 5) August 2012 – Industrial Fire – NYS (MA Region 1) Oct/Nov 2012 - Superstorm Sandy Jan 2013 Influenza Event – Boston & Hartford, CT Activations for Hospital Resident Decompression Feb 2013 – Blizzard (NEMO) Jan 2014 – Snowstorm
OVERVIEW of the CT LTC-MAP
Plan Operation is 1 st within your town/city. Additional Support will come from your Region then other regions in a widespread disaster. ~500 LTC / 30 Hospitals / 4 LTACs or Rehab Hospitals 213 LTC / 11 Hospitals Regions 1, 3, 4 & 5 151 LTC
The Basics • • Identify needs and provide supplies/ equipment/pharmaceuticals as necessary Assist with transportation of supplies / staff / equipment / evacuated residents Provide staffing support (whether a facility is evacuating or isolated) Place and support the care of evacuated residents (continuity of care / surge locations)
Member Responsibilities • Memorandum of Understanding (MOU) • Sign it - Transfer Agreements with everyone • If no MOU = No transfer agreement (per DPH, DSS and CMS) • Who are we qualified to care for? (# and type) • • Required Plan Forms for Use: • • Surge Capacity – Accept 110% of licensed beds (not mandated; but a process to support others) Resident Emergency Evacuation Form Resident / MR / Staff / Equipment Tracking Sheet Influx of Residents Log Controlled Substance Receiving Log Pharma / Equip / Supplies Request Form Mandatory Attendance at Annual Meeting Exercise Annually with the LTC-MAP
Memorandum of Understanding (MOU) (Located in Annex I of the plan) • • The MOU is a “voluntary agreement” among members By signing the (MOU) all facilities agree to their intent to abide by the terms in the event of a disaster. The terms are to be incorporated into the facility’s Emergency Management Plans and Emergency Operations Plans BE SURE YOUR MOU IS SIGNED AND RETURNED TO RUSSELL PHILLIPS & ASSOCIATES OR CAHCF
Are You Required to Take Residents in an Evacuation? NO – Why? • If you are impacted by the disaster, it could be more dangerous to move them to your location • • • Infrastructure issue Staffing issue (and they can’t send staff) Example: Superstorm Sandy – NYC was looking to move 2, 000 residents into CT. ONLY facilities that were on commercial power were considered.
Responsibility for Care • Patient Accepting Facility (PAF) receives the resident: • • Do not admit (being finalized with DSS) Under the care of the PAF Return the resident to the facility or origin after completion of the disaster Ethical standpoint – no marketing efforts to the residents and their families
Reimbursement Approach Disaster Struck Facility • • Can the facility reopen within 30 days? IF YES – The resident is never discharged and they are “sheltered” at the PAF IF NO – The resident is discharged and permanent placement will be addressed Process of not admitting (“sheltering”) – enables surge to 110% of licensed beds to take place (waiver) DPH will support this process
Reimbursement Approach • Disaster Struck Facility • • Paid by CMS (Medicare), DSS (Medicaid) or private pay PAF is paid by DSF at DSF rate • • If 100% of services provided by PAF, 100% of payment If staff, equipment and meds come from DSF, amicable division (incremental labor costs & consumables) If exceeding licensed beds, amicable division Mediation or Arbitration (called out in MOU)
Facilities Still Must Be Ready Internally What we need to have internally: • • Have an Incident Command System (Nursing Home Incident Command System – NHICS) Full Building Evacuation Plan • • • Get residents to the sidewalk Influx of Residents (Census Reduction / Surge Capacity Plan) Resources & Assets for 96 hours • Self-sustainability
Disaster Struck Facility
Shelter-in-Place / Evacuating Disaster Struck Facility (when speaking with DPH, the LTC-MAP, Local Emergency Manager or 911) • Size-up the Situation • • Resource & Assets needs to stay operational Failure of infrastructure to remain in the facility Who – Your contact name and phone number Where – Facility Name, Address and Town/City What – What is the issue? When – Window of time the resources will be required in / How long until the evacuation must commence Why – Reason
Shelter-in-Place / Evacuating
Actions of Disaster Struck Facility NOTIFY: Call 911 / begin Internal Activation process • NOTIFY: CMED 24/7 to activate the Region’s Healthcare Facilities and Critical Partners through the alert notification system • ACTIVATE: Emergency Reporting System • • www. mutualaidplan. org/ct • LTC Coordinating Center PREPARE: Evacuation? Staffing? Equip? Supplies? • PREPARE: Transportation Evacuation Tool Complete (if evacuating) • PREPARE: Generator Information - Update (if prestorm/event) •
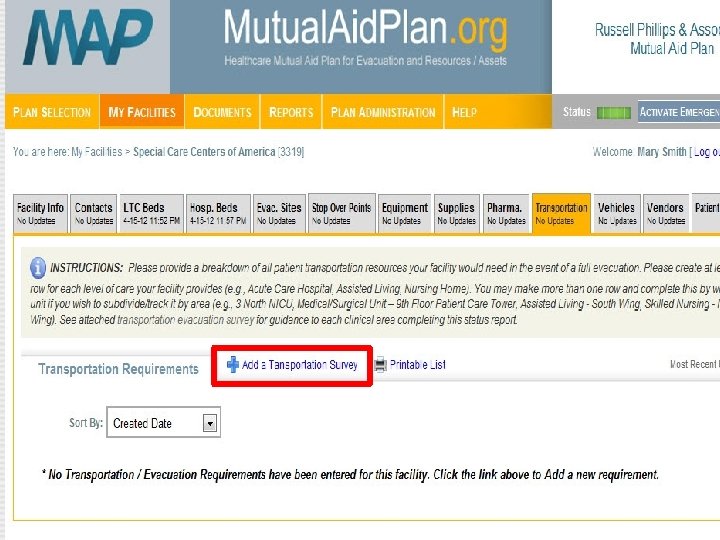
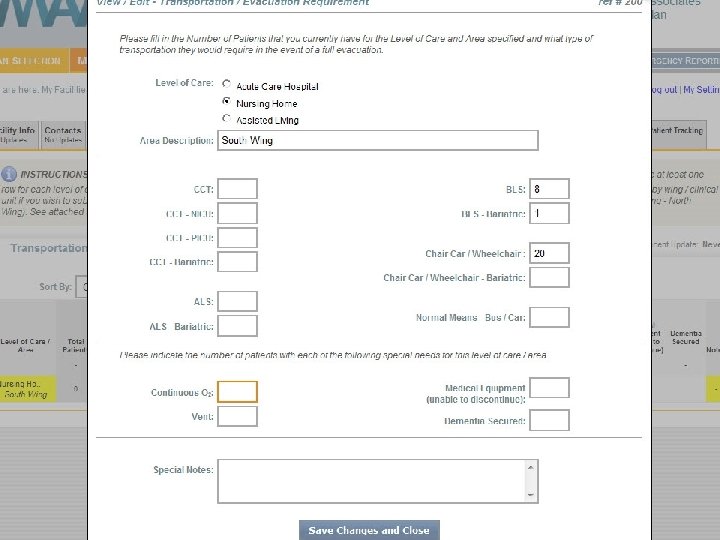
Transportation Evacuation Surveys (transportation tab on website) Provides Public Health, Fire, EMS and Emergency Management with strong knowledge of the resources needed to evacuate our facility (Ambulances, wheelchair vehicles and buses) • • Consider completing with monthly fire drills (each resident care area) On website for an automated tool
Transportation Resources Total Vehicles Owned by Members • • • 189 Vehicles 1, 173 Total seats 271 Residents in Wheelchairs • • Capacity: 1, 472 Transportable Patients Supplies/Equipment: 34 Dump / Box Trucks & Pick-ups
Pre-established Evacuation Sites • • Primary sites should be pre-selected using the LTC Patient Care Categories (next slide – from website) Address highest acuity residents first • • Who matches up best with our residents Address their surge numbers next Always assume they have no open beds • How many of your residents can they accept at 110% surge • • Process to communicate with them • Know where they are, their point person and contact information
24
Resident Tracking – What goes with the Resident • Resident Emergency Evacuation Form • • Active Chart (or Current Service Plan for AL) • • • 1 per resident - info and acuity / mobility / risks Include MAR (Med List), Meds & Controlled Substances Wristband (name / DOB) Resident, MR, Staff & Equip Tracking Sheet • List of residents; by facility they evacuated to • Transportation vehicle info and time departed • What (and whom) went with them • • Photo, if possible DNR Bracelets / Transfer Sheets
Patient Accepting Facilities/Lenders
Actions of Patient Accepting Facilities/Lenders • Prepare to receive residents • • Complete Emergency Reporting Complete the Influx of Resident Log - residents arrive Confirm with DSF or LTC Coord. Center that the residents are received – “CLOSE THE LOOP” • • • Open beds vs. Surge Area Complete Electronic Resident Tracking information Start a new chart for resident Notify DPH (if NH/RCH) and your local AHJ about activating a Surge Plan (Influx / Surge Guidelines) If Lender: Prepare to provide Resources/Assets
What happens at 2: 00 AM? Anyone who might answer the phone: Basic knowledge that CT LTC-MAP exists (there is a plan) • Get the name of the person calling, facility, contact number and issue or request • OR – Listen to the automated message and take down directions for what it tells you to do • Inform the Nursing Supervisor ASAP • Nursing Supervisor – Scope will determine actions • • • Immediate analysis of open beds – M / F / Either Activate internal emergency notification tree Complete Emergency Reporting- www. mutualaidplan. org/ct Evacuation? Prepare to receiving incoming residents Resource & Asset Request: Prepare to provide staff, equipment, supplies or transportation
Influx of Residents / Surge Plan Algorithm
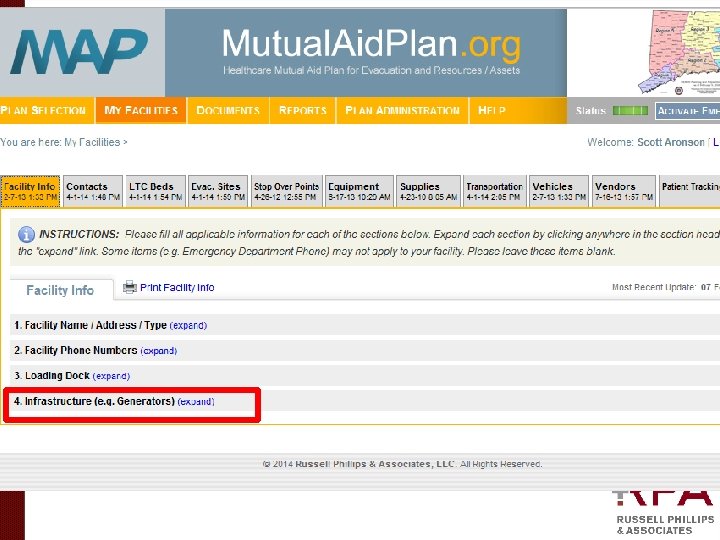
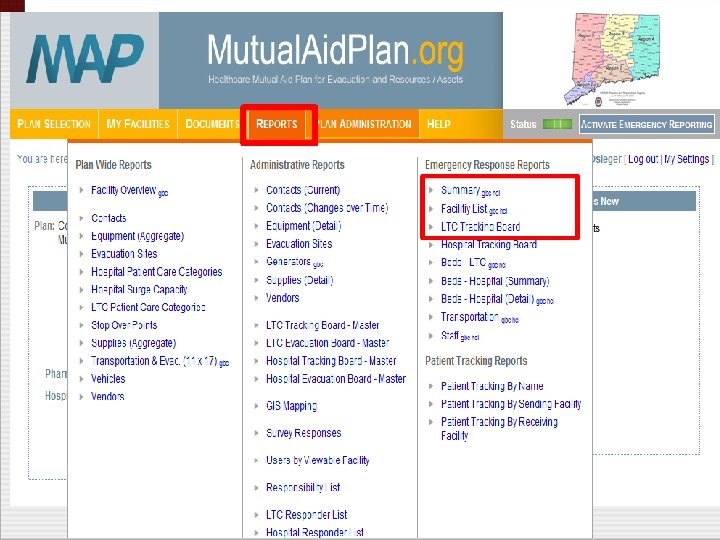
CT LTC-MAP Website (all tabs are specific to our facility based on data we enter)
Know your generator information in advance of an emergency
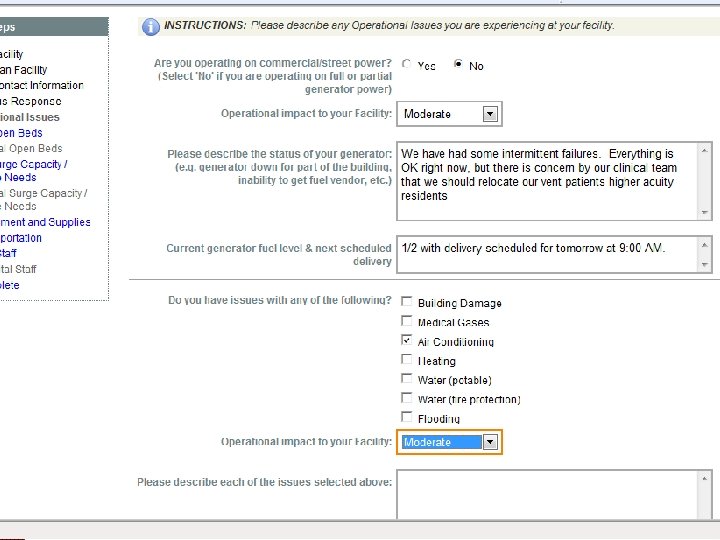
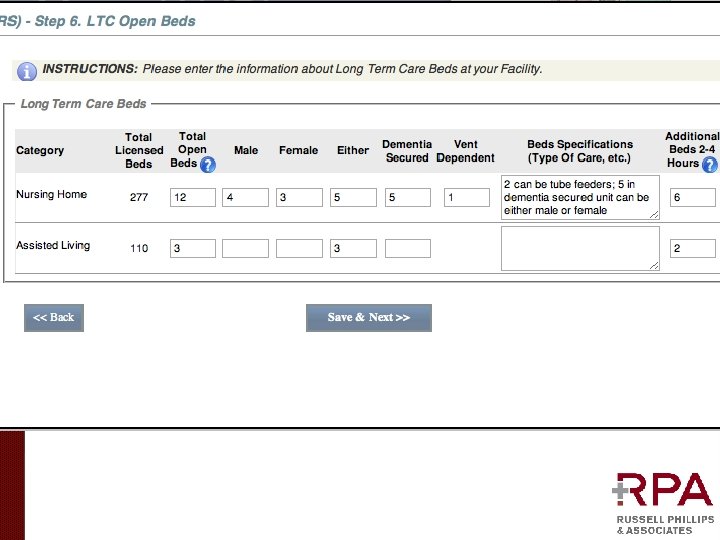
Emergency Reporting Designated Facility Leadership or Nursing Supervisor (complete for LTC -MAP when requested)
Internal Situation-Status Report & Emergency Reporting: What You Should Know (and WHY) HANDOUT Operational Issues at your facility (other plan members) • Open Beds • Available Transportation for • • Resident Transportation • Movement of Supplies and Equipment Resources & Assets (needed) • Resources & Assets (you could provide) • • Equipment • Supplies • Staffing
LTC Coordinating Center
Long Term Care (LTC) Coordinating Center § Region 1: Lord Chamberlain (Stratford) / Back-up: Jewish Senior Services (Fairfield) § Region 3 Duncaster (Bloomfield) / Back-up: RCC in Manchester or CRCOG § Region 4: Groton Regency Center / Back-up: Region 3 § Region 5: Masonicare at Newtown / Back-up: Meadow Ridge (Redding)
Function of the LTC Coordinating Center “Air Traffic Control” • • • Staffed by volunteers from the LTC-MAP Assist with resident placement Support resident tracking - “Close the loop” Assist with obtaining staff, supplies and equipment Assist with transportation of residents, staff, supplies and equipment Support interaction with local and state agencies ENSURE ALL MEMBERS ARE ACCOUNTED FOR
Who to go to with Questions? David Hood dhood@phillipsllc. com Scott Aronson saronson@phillipsllc. com