Congenital Syphilis Irina Tabidze MD MPH and Thad

Congenital Syphilis Irina Tabidze, MD, MPH and Thad Zajdowicz, MD, MPH STD/HIV Division Chicago Dept of Public Health
 • Syphilis is a chronic infection caused by the spirochete Treponema")
Congenital Syphilis (CS) • Syphilis is a chronic infection caused by the spirochete Treponema pallidum, which is of particular concern during pregnancy because of the risk of transplacental infection of the fetus. • Congenital infection is associated with several adverse outcomes, including: -Perinatal death -Premature delivery -Low birth weight -Congenital anomalies

Modes of Transmission: • Sexual contact. • Trans-placental passage from infected mother. • Contact with lesion at the time of delivery. • The risk of developing syphilis after exposure is about 40%.

Risk Factors for CS • Lack of or inadequate prenatal care. • Maternal substance abuse. · Failure to repeat a serological test for syphilis in the third trimester. · Treatment failure. · Inadequate access to Sexually Transmitted Diseases (STD) clinics and STD outreach activities.

Epidemiology of CS • Incidence of CS reflects the rate of syphilis in women of childbearing age. • Peaks in CS occur one year after peaks in P&S syphilis in women.

Congenital syphilis — Rates for infants <1 year of age: US, 1981– 2002 and the Healthy People 2010 objective Rate (per 100, 000 live births) 125 Cong. Syphilis 2010 Objective 100 75 50 25 0 1981 83 85 87 89 91 93 95 97 99 2001 Note: The Healthy People 2010 objective for congenital syphilis is 1. 0 case per 100, 000 live births. The surveillance case definition for congenital syphilis changed in 1988.

Congenital syphilis — Reported cases for infants <1 year of age and rates of P &S syphilis among women: US, 1970– 2002 P&S rate (per 100, 000 population) CS cases (in thousands) 7. 5 20 Kaufman Criteria CDC Surveillance Definition 16 12 6. 0 4. 5 P&S Syphilis 8 3. 0 Congenital Syphilis 4 0 1970 75 80 85 90 95 1. 5 0. 0 2000 Note: The surveillance case definition for congenital syphilis changed in 1988.

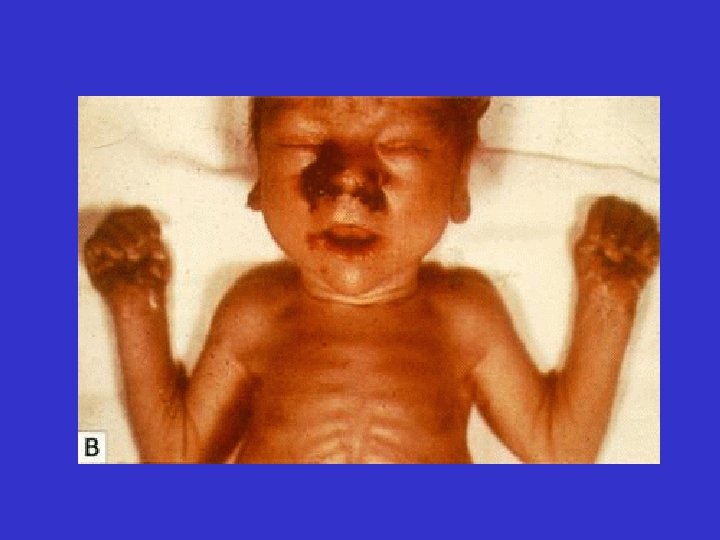
Syphilis in Newborns • Two-thirds of live-born neonates with CS are asymptomatic at births. • Overt infection can manifest in the fetus, the newborn, or later in childhood. • The infant may have many or even no signs until 6 -8 weeks of life (delayed form). • Clinical manifestations after birth are divided arbitrarily into: - Early CS (<=2 years of age) and - Late CS ( >2 years of age)

Clinical Manifestations of Early CS • • Condyloma Lata Maculopapular rash Hepatosplenomegaly Jaundice due to the hepatitis Anemia Osteochondritis Snuffles Pseudoparalysis • Lymphadenopathy • Mucous patches

Congenital Syphilis

Congenital Syphilis

Congenital Syphilis

Congenital Syphilis
: -Hutchinson’s teeth (blunted upper incisors)")
Clinical Manifestations of Late CS • Hutchinson’s triad (63%): -Hutchinson’s teeth (blunted upper incisors) -Interstitial keratitis -VII nerve deafness • Frontal bossae (bony prominences of the forehead) (87%) • Saddle nose (74%) • Defect of hard pallet • Clutton’s joints (bilateral painless swelling of knees) • Saber chins • Short maxillas • Protruding mandible
: Interstitial keratitis Teeth abnormalities Deafness")
Congenital Syphilis Hutchinson’s Triad (late congenital syphilis): Interstitial keratitis Teeth abnormalities Deafness

Congenital Syphilis

Clutton’s Joints

Saddle Nose

Sabre Shins

Laboratory Diagnosis • Direct visualization - Darkfield examination of exudate - Direct fluorescent antibody to T. pallidum • Serologic testing - Nontreponemal Antibody tests (VDRL test and RPR test) - Treponemal Antibody tests (FTA-ABS and MHA-TP)

Interpretation of the Syphilis Serology of Mothers & their Infants Nontreponemal Test Treponemal Test Mother Infant - - + + - - Interpretation No syphilis or incubating syphilis in the mother and infant No syphilis in mother Maternal syphilis with possible infant infection + + or - + + + Recent or previous syphilis in the mother; possible infection in infant - - + + Mother successfully treated for syphilis before or early in pregnancy;

Maternal Treatment • Penicillin is the gold standard for the treatment of syphilis. • Pregnant women with syphilis should be treated with the appropriate penicillin regimen according to their stage of disease. • Sexually Transmitted Diseases Treatment Guidelines 2002. MMWR 2002; 51 (No. RR-6): [19 -23]

Treatment of Infants • Sexually Transmitted Diseases Treatment Guidelines 2002. MMWR 2002; 51 (No. RR-6): [26 -28]

Follow-up evaluation • Non-treponemal antibody serologic testing should be checked at 1, 3, 6, 12 and 24 months following treatment. • Titers should decrease four-fold by 6 months post therapy and become non -reactive by 12 to 24 months. • Titers that show a four-fold rise or do not decrease suggest either treatment failure or re-infection.
- Slides: 25