CONGENITAL DIAPHRAGMATIC HERNIA Maj Asrar Ahmad MBBS FCPS

CONGENITAL DIAPHRAGMATIC HERNIA Maj Asrar Ahmad MBBS, FCPS

Anatomy 5% 95 %

Embryology

Pathophysiology

Pathophysiology q Pulmonary hypoplasia “compression theory” - modeled in fetal lambs - rationale for early surgery “global embryopathy” - modeled in newborn rats - rationale for new therapeutic ideas q Pulmonary hypertension - causes persistent fetal circulation

Incidence q 1: 2500 -5000 live births q 1100 cases in the U. S. annually q 80 % Left side survival remains around ~65%

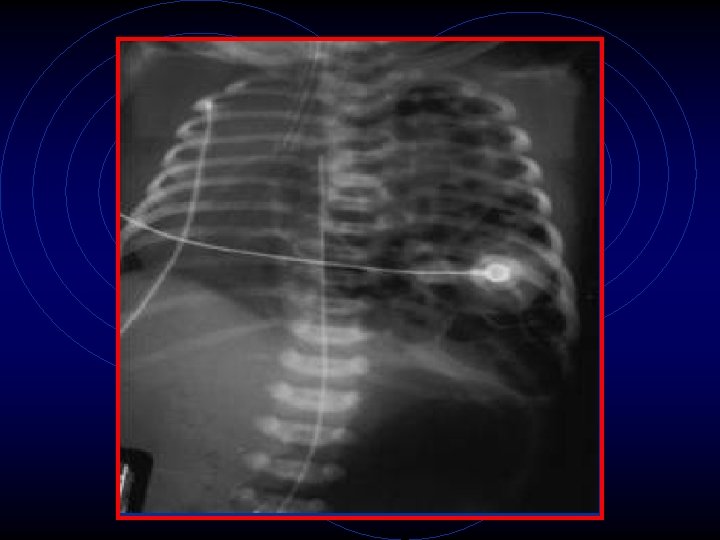
Diagnosis q Antenatal: Ø U/S at ~20 weeks gestation Ø ~60% Ø Polyhydramnios; intrathoracic stomach or liver; abdominal circumference; lung-to-head ratio

Presentation q Shortness of breath q Scaphoid abdomen Three general presentations: q Severe respiratory distress at the time of birth. q Respiratory deterioration hours after delivery q Benefit from correction of hypoxemia and pulmonary hypertension q Feeding difficulties, chronic respiratory disease, pneumonia q 10 -20 % intestinal obstruction

Initial Management q Oxygenate but avoid barotrauma q Intubate q Sedate q NGT for decompression

Medical Management q Medical emergency not surgical q q q Pulmonary vasodilators Inotropes High frequency oscillatory ventilation ECMO Surfactant Antenatal steroids?

ECMO

ECMO

Surgical Management

Surgical Management

Surgical Management

Surgical Management

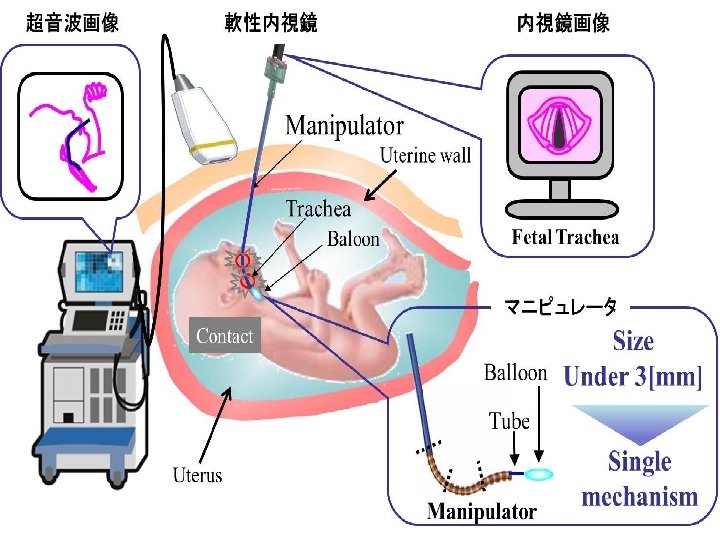
Developing Therapies q Fetal surgery q PLUG fetal surgery q Growth factors

THANK YOU
- Slides: 20