Congenital cardiac defects Prepared by Ayda khader LOGO

Congenital cardiac defects Prepared by : Ayda khader L/O/G/O April / 2018

Ø Babies born with congenital heart defects is the second largest group of babies born with abnormalities. Ø Incidence 8/1000 live births have some degree of congenital heart disease Ø about one-third of these babies will be symptomatic in early infancy. Ø The critical period of exposure to teratogens in respect of embryological development of cardiac tissue is from the 3 rd to the 6 th week.

Ø Prenatal detection of cardiac problems are being identified by means of detailed ultrasound scanning Ø For babies with complex congenital heart disease this enables a multidisciplinary plan for birth and immediate neonatal care, to be made well in advance of delivery Ø the detection of many defects is still dependent upon accurate observations and examination during the neonatal period.

Ø Postnatal recognition by symptomatic and routine check Ø early identification and referral of babies with significant cardiac malformations is desirable Ø baby with suspected congenital heart disease should not be sent home until he/she has been reviewed by an experienced paediatrician or a definitive diagnosis has been made
 Cyanotic")
• babies with cardiac anomalies can be divided into two groups: 1) Cyanotic heart disease (right-to-left shunt) 2) Acyanotic heart disease (left-to-right shunt)

Causes • Approximately 90% of cardiac defects cannot be attributed to a single cause. • Chromosomal and genetic factors account for 8% • 2% are caused by teratogens. .
 Cardiac catheterization")
Diagnostic evaluation by : Echocardiogram Chest X ray Electrocardiogram (ECG) Cardiac catheterization
, v Ventricular Septal Defect (VSD), v")
Acyanotic Heart Disease v Atrial Septal Defect (ASD), v Ventricular Septal Defect (VSD), v Patent Ductus Arteriosus (PDA), v coarctation of the aorta v aortic stenosis v hypo plastic left heart syndrome.

qmidwives may detect in these babies the first subtle signs is : § tachypnoea, tachycardia § incipient cyanosis, especially following the exertion of crying or feeding § seldom require medical or surgical intervention in early neonatal life, but do require careful follow-up for signs of developing heart failure and may require surgery or interventional cardiology at a later stage.
 • It is an abnormal opening between right and left")
Ventricular Septal Defect (VSD) • It is an abnormal opening between right and left ventricles, may vary in size ; small pinhole to the absence of the septum, resulting in common ventricle. • Frequently associated with other defects • Lt –to – Rt Shunt • 30% of defects

• Ventricular septal defects are a common cause of murmurs in the term infant. • Many of these defects are small, no haemodynamic consequence and close spontaneously. • Larger defects may lead to heart failure and surgical closure may be necessary although not usually in the neonatal period
 • An abnormal opening between atria with a Lt-to-Rt Shunt.")
Atrial Septal Defect (ASD) • An abnormal opening between atria with a Lt-to-Rt Shunt. Blood in left atrium flows into right atrium. • 10% of defects • Reduced blood volume in systemic circulation
 • more common in preterm infants • The fetal ductus")
Patent Ductus Arteriosus: (PDA) • more common in preterm infants • The fetal ductus artery connecting the aorta and the pulmonary artery fails to close within few weeks after birth, so the blood flows from the high pressure of the aorta to the lower pressure of the pulmonary artery (Lt – to –Rt ) shunt ØDuctus normally closes within hours of birth ØConnection between the pulmonary artery (low pressure) and aorta (high pressure)
 which constricts the muscle in")
• Medical management by using Endomethacin (Prostaglandin inhibitor) which constricts the muscle in the wall of the PDA and promotes closure • Surgical Management if medical treatment with ibuprofen or indomethacin is ine�ective

v Coarctation of the aorta and aortic stenosis are usually amenable to surgical correction. Hypoplastic left heart syndrome remains a major surgical challenge, requiring a number of surgical procedures in childhood v As in the duct-dependent cyanotic heart conditions, a prostaglandin infusion may be required whilst further investigations and discussions regarding the possibility of surgical correction take place

cyanotic Heart Disease v v v transposition of the great arteries pulmonary atresia tetralogy of Fallot tricuspid atresia total anomalous pulmonary venous drainage univentricular /complex heart.

q Although cyanosis can be a presenting feature of a number of non-cardiac conditions (As respiratory disease, persistent pulmonary hypertension of the newborn, sepsis), congenital heart disease should always be considered as a possible explanation. q Administration of oxygen to babies with cyanotic heart disease may have little e�ect on their oxygen saturation levels. q This observation, along with other routine investigations excluding other causes of cyanosis, may suggest a diagnosis of cyanotic heart disease. q The definitive diagnostic investigation is Echo
, tachypnoea")
q The persistence of central cyanosis (cyanosis of the lips and mucous membranes), tachypnoea and tachycardia may be the first signs q Chest X-ray should be carried out to exclude abnormalities of the respiratory tract, respiratory disease and diaphragmatic hernia. q Cyanosis occurs when there is more than 5 g/dl of circulating deoxygenated haemoglobin. q In congenital cyanotic heart disease, abnormal anatomy leads to mixing of oxygenated and deoxygenated blood
 • It is narrowing at the entrance of the pulmonary artery")
Pulmonary Stenosis (PS) • It is narrowing at the entrance of the pulmonary artery (pulmonary valve) leads to narrowing and obstruction between the right ventricle and the pulmonary artery. • Resistance to blood flow cause Hypertrophy of right ventricle • Nonsurgical treatment by Cardiac catheterization to dilate the valve and open up the obstruction by using a balloon angioplasty • Surgical correction by Transventricular valvotomy Bock procedure
 • Narrowing of aortic valve causing resistance to blood flow in")
Aortic Stenosis (AS) • Narrowing of aortic valve causing resistance to blood flow in the Lt ventricle, decrease cardiac output, Lt ventricular hypertrophy and pulmonary vascular congestion. • Nonsurgical correction: Dilating narrowed valve with balloon angioplasty in the cath lab • Surgical correction by valvotomy
 • There is localized narrowing near the insertion of ductus")
Coarctation of Aorta: (COA) • There is localized narrowing near the insertion of ductus arteriosus resulting in: – Increased pressure in proximal structures to the defect (Head and upper extremities) – Decreased pressure distal to obstruction (body and lower extremities) • Congenital narrowing of the descending aorta • 7 % of defects • 80% have aortic-valve anomalies • Difference in BP in arms and legs (severe obstruction)

• Medical Treatment: – Prostaglandin may given to keep the PDA open to reduce the pressure changes – Antibiotic prophylactic need due to possible aortic valve abnormalities.
 • Most common cardiac malformation responsible for cyanosis in a")
Tetralogy of Fallot (TOF) • Most common cardiac malformation responsible for cyanosis in a child over 1 year
")
Tetralogy of Fallot (TOF)

TOF • The most common type of cyanotic heart disease • its involve four Components ØVentricular Septal defect - VSD ØPulmonary stenosis ØOverriding of the aorta – enlargment of aortic valve ØHypertrophy of right ventricle

Clinical Manifestations: TOF • Some infants are acutely cyanosed at birth, others have mild cyanosis that progresses over the 1 st year as the pulmonary stenosis worsen • Acute episodes of cyanosis and hypoxia (blue spells) usually during crying or after feeding • Severe irritability due to low oxygen levels • Poor growth • clubbing of fingers,
 ccc by sudden cyanosis and")
• Squatting pouster • hypoxia spell (Tet spells) ccc by sudden cyanosis and syncope
 medical or surgical intervention in early neonatal life, but do require careful")
Management: (TOF) medical or surgical intervention in early neonatal life, but do require careful follow-up for signs of developing heart failure and may require surgery or interventional cardiology at a later stage

q It is important to realize, however, that not all heart murmurs heard at this time are significant. q Equally the absence of a murmur at discharge from hospital does not exclude significant heart disease. q There is therefore increased responsibility on community midwives to be observant and to communicate effectively with parents. q Parents who report any changes in the baby's behaviour such as breathlessness or cyanosis should never be ignored, but rather encouraged to seek medical advice promptly.
 • • • Pulmonary artery leaves the Lt ventricle")
Transposition of Great Arteries (TGA) • • • Pulmonary artery leaves the Lt ventricle Aorta exits from the Rt ventricle With no communication between systemic and pulmonary circulation Males are affected more than females Associated defects such as Septal defects or patent ductus arteriosus permits blood to enter the systemic circulation and or pulmonary circulation for mixing of saturated and non saturated blood
 Surgical Palliative treatment Administration of IV prostaglandin E 1 to keep the")
Management: (TGA) Surgical Palliative treatment Administration of IV prostaglandin E 1 to keep the ductus arteriosus open 1. Rashkin procedure: Enlarge septal defect Complete repair: • Switching the great vessels to their correct anatomic position.

l nervous system abnormalities L/O/G/O

Central nervous system abnormalities Ø Ingestion of folic acid supplements prior to conception and during the early stages of pregnancy has helped prevent such abnormalities. Ø In addition, the ability to recognize these anomalies prenatally has resulted in some parents choosing selective termination of pregnancies where severe neural tube defects are found.

Anencephaly • This major abnormality describes the absence of the forebrain and vault of the skull. • It is a condition that is incompatible with sustained life but occasionally such a baby is born alive. • The midwife should wrap the baby carefully before showing him to the mother.

• It may be beneficial for the parents then to see the full extent of the abnormality, unpleasant though it is. • Seeing the whole baby will help them to accept the reality of the situation and prevent imagination of an even more gruesome picture.

Spina bifida ü Spina bifida results from failure of fusion of the vertebral column ü There is no skin covering the defect, which allows protrusion of the meninges, hence the term meningocele ü The meningeal membrane may be flat or appear as a membranous sac, with or without cerebrospinal fluid, but it does not contain neural tissue

Meningomyelocele ü Is a more serious defect in which the spinal cord and / or nerve roots as well as meningocele covering protrude through the spina bifida. ü Meningomyelocele usually gives rise to neural damage, producing paralysis distal to the defect, and impaired function of urinary bladder and bowel.
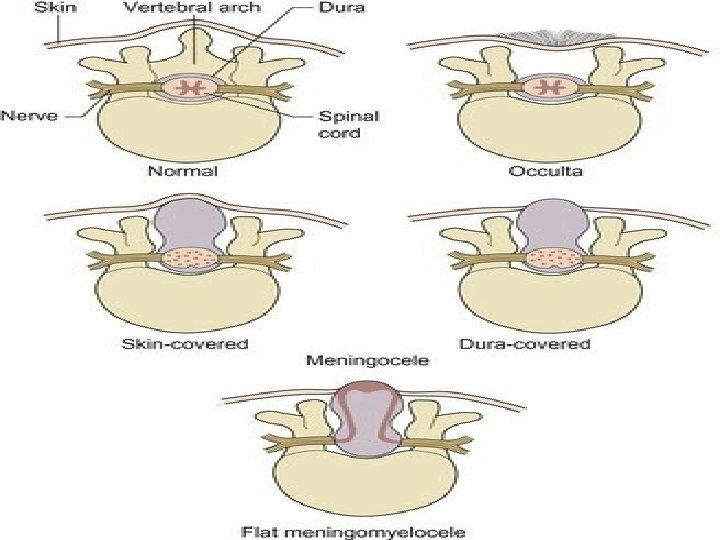

ü The lumbosacral area is the most common site for these to present, but they may appear at any point in the vertebral column Encephalocele is a congenital anomaly characterized by herniation of the brain and/or meninges through a defect in the skull.

v. Surgical intervention for myelomeningocele carries a high rate of success of skin closure, but has no impact on any damage already present in the cord or more distally v. It is seldom necessary to close the back within 24 hrs of birth v. Following examination of the baby, discussion with the parents will allow them to make an informed choice about whether or not they wish their baby to have surgery.

Spina bifida occulta v. Usually the 5 th lumber and 1 st sacral vertebrae are affected with no protrusion of interspinal contents the spinal cord and its cover the skin over the defect may reveal a dimple, small fatty mass or a tuft of hair.

Hydrocephalus ü The abnormal increase in cerebrospinal fluid volume within the intracranial cavity due to a defect in the cerebrospinal fluid drainage system, intracranial pressure increases, the scalp veins dilate, and the cranial suture begin to separate ü hydrocephalus may either be present at birth or develop following surgical closure of a myelomeningocele

ü The risk of cerebral impairment may be minimized by the insertion of a ventriculoperitoneal shunt ü Attendant risks with these devices are that the line blocks and that the shunt is a portal for infection leading to meningitis

The midwife must be alert for the signs of increased intracranial pressure: q large tense anterior fontanelle q splayed skull sutures q inappropriate increase in occipitofrontal circumference q sun-setting appearance to the eyes q irritability, or abnormal movements.

Microcephaly ü This is where the occipitofrontal circumference is more than two standard deviations below normal for gestational age. ü The disproportionately small head may be the result of intrauterine infection (e. g. rubella), a feature of fetal alcohol syndrome, or part of a number of defects in some trisomic disorders. ü Most babies will have learning difficulties with evidence of cerebral palsy and often seizures.

Parents who have a baby with a neural tube defect should be offered genetic counselling since the risk of recurrence is one in 25.

Thank You! L/O/G/O With best wishes , Ayda khader
- Slides: 47