Congenital abnormalities Prepared by Ayda khader Sept 2017

Congenital abnormalities Prepared by : Ayda khader Sept. 2017

Out lines v Objective v Communicating the new v Prenatal screening v Chromosomal abnormality v Gastrointestinal defect v Respiratory abnormality v Congenital cardiac defect v Central nervous system abnormality v Musculoskeletal deformities v genitourinary system defect v Disorder of sexual development v Teratogenic causes v Support for the midwife

objectives ü address issues such as who should tell the parents and how and when they should be told ü describe and explain specific congenital abnormalities ü explore the complementary roles of the midwife and paediatrician in providing care ü consider the psychological impact on staff and the strategies that could be put in place to minimize the accompanying stress

Ø midwife who first notices an abnormality in the baby either during the process of the birth or on routine newborn examination. Ø there is sometimes a difference of opinion as to who should communicate the news to the parents Ø The midwife–client relationship ought to be, one of mutual trust and respect. Honesty is an implicit tenet of such a relationship Ø the midwife tells both parents sensitively but honestly that she has concerns, and shows them any obvious abnormality in the baby.

Ø in cases of suspected chromosomal disorders, it could be argued that the issue is less clear cut. Discretion could therefore be exercised in the precise form of words used, but the intention of inviting a second opinion should be made clear to the parents. Ø midwife be present when an paediatrician examines the baby and during any dialogue between the parents and medical staff so that she is aware of exactly what has been said

Ø Some abnormalities are slight and cause no further problems for the parents or child, whereas others are profound and cause the subsequent daily care to be fraught with difficulties. Ø abnormalities involving the face cannot be hidden and most distressing for parents Ø The psychological impact on parents of being told or shown Ø Great sensitivity is required when showing the baby to the parents for the first time. Ø families receive accurate, and appropriate information about their baby's condition Ø the midwife is most likely to encounter in any discussion

NB : it is essential that families receive accurate, consistent and appropriate information about their baby's condition. Since a comprehensive discussion of every malformation is clearly not possible, selection has therefore been made of those the midwife is most likely to encounter.

FACTS ü An estimated 276 000 babies die within 4 weeks of birth every year, worldwide, from congenital anomalies. ü The incidence of major congenital malformations is 2– 3% of all births ü Congenital anomalies can result in long-term disability, which may have significant impacts on individuals, families, health-care systems and societies. ü The most common severe congenital anomalies are heart defects, neural tube defects and Down syndrome.

ü Although congenital anomalies may be genetic, infectious, nutritional or environmental in origin, most often it is difficult to identify the exact causes ü Some congenital anomalies can be prevented. For example, vaccination, adequate intake of folic acid or iodine through fortification of staple foods or provision of supplements, and adequate antenatal care keys for prevention.

Palliative care v There a number of severe congenital malformations which are incompatible with sustained life, such as anencephaly. v Many of these conditions are diagnosed antenatally and, whereas some parents opt for termination of the pregnancy, others choose palliative care after birth v Discussion with the parents should explore any anxieties they may have, e. g. pain relief for the baby. v It should also include factual information about the likely clinical course including how long the baby may survive and a gentle explanation of the process of death.

v After birth priority should be given to ensuring the comfort of the baby whilst at the same time supporting the parents v It is important to treat the parents and the baby with kindness and dignity at all times v Providing end of life care for infants with severe congenital malformations can be di�cult and emotionally draining for sta� v A formal debrief within the multi-professional team may be useful.

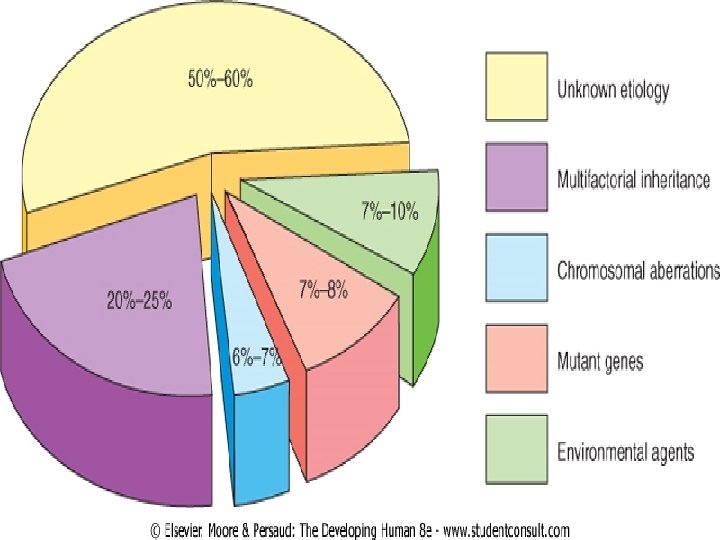
What is birth defect ? Any defect or abnormality of structure, function or form, present at birth that results in physical or mental disability or is fatal What Causes birth defect ? 1) chromosomal abnormalities 2) single gene defects 3) mitochondrial deoxyribonucleic acid (DNA) disorders 4) teratogenic causes 5) multifactorial causes 6) unknown causes. •

Chromosomal abnormalities Ø Every human cell carries a blueprint for reproduction in the form of 44 chromosomes (autosomes) and two sex chromosomes. Ø Each chromosome comprises a number of genes, which are specific sequences of DNA coding for particular proteins. Ø The zygote should have 22 autosomes and one sex chromosome from each parent Ø Any a fault occur in either the formation of the gametes or following fertilization abnormalities in chromosome number (aneuploidies) or structure (deletions, duplications, inversions, translocations) may occur. Ø Each abnormal chromosomal patern has a characteristic clinical presentation
 • Genes are composed of DNA • each is concerned")
Gene defects (Mendelian inheritance) • Genes are composed of DNA • each is concerned with the transmission of one specific hereditary factor • inherited factors may be dominant or recessive • A dominant gene will produce its e�ect even if present in only one chromosome of a pair • . osteogenesis imperfecta and Huntington's chorea are examples of dominant conditions • A recessive gene needs to be present in both chromosomes before producing its e�ect • Examples of autosomal recessive conditions are cystic fibrosis or phenylketonuria. • .
 for")
• In a recessive disorder, the risk is 1 : 4 (25%) for each and every pregnancy • In a dominantly disorder the risk of an a�ected fetus is 1 : 2 (50%) for each and every pregnancy • In an X-linked recessive inheritance the condition a�ects almost exclusively males, although females can be carriers

Mitochondrial inheritance • Mitochondria are cellular structures responsible for energy production • Mitochondria are always inherited from the mother • Symptoms and signs of mitochondrial disorders can be diverse but tend to occur in tissues that have high energy requirements such as the brain and muscles • Examples are very rare but include, mitochondrial encephalomyopathy with lactic acidosis and stroke-like episodes (MELAS

Teratogenic causes • A teratogen is any agent that raises the incidence of congenital malformation • The list of known and suspected teratogens is continually growing included: 1) prescribed drugs(e. g. anticonvulsants, anticoagulants and preparations containing large concentrations of vitamin A such as those prescribed for the treatment of acne), 2) drugs used in substance abuse (e. g. heroin, alcohol and nicotine), 3) environmental factors such as radiation and chemicals (e. g. dioxins, pesticides), 4) infective agents (e. g. rubella, cytomegalovirus) and maternal disease (e. g. diabetes

• several factors influence the e�ect produced by any one teratogen, such as 1) gestational age of the embryo 2) fetus at the time of exposure 3) length of exposure 4) toxicity of the teratogen. • Direct cause and e�ect is sometimes di�cult to establish
 and")
Multifactorial causes • These are due to interactions between specific genes (genetic susceptibility) and environmental influences (teratogens).

Unknown causes • In spite of a growing body of knowledge, the specific cause of many congenital anomalies remains unspecified and they occur sporadically in families

Although approximately 50% of all congenital anomalies cannot be linked to a specific cause, there are some known causes or risk factors.

Can birth defect be Prevented? • Preventive public health measures delivered through health services decrease the frequency of certain congenital anomalies. Primary prevention of congenital anomalies includes: ü improving the diet of women throughout their reproductive years, ensuring an adequate dietary intake of vitamins and minerals, and particularly folic acid, through daily oral supplements or fortification of staple foods such as wheat or maize flours

ü ensuring mothers abstain from, or restrict, their intake of harmful substances, particularly alcohol; ü controlling preconceptional and gestational diabetes, through counselling, weight management, diet and administration of insulin when needed; ü avoiding environmental exposure to hazardous substances (e. g. heavy metals, pesticides) during pregnancy;

ü ensuring that any exposure of pregnant women to medications or medical radiation (e. g. imaging rays) is justified, based on careful health risk–benefit analysis; ü improving vaccination coverage, especially against the rubella virus, for children and women. ü increasing and strengthening education of health staff and others involved in promoting prevention of congenital anomalies.

Preventing Birth Defects • • Eat well during pregnancy Avoid marrying close relatives Consider not having children after age 35 or 40 Avoid all medicines during pregnancy Avoid contact with pesticides and other poisons Avoid tobacco and alcohol While pregnant, stay away from children with German measles

Can some birth defect be diagnosis befor birth ? some birth defect can be diagnosed befor birth some prenatal tests that can be taken are: q Amniocentesis q Ultrasound q Choronic villus sampling

PRENATAL DIAGNOSIS • Methods of prenatal diagnosis are divided into invasive and non-invasive techniques. • Technique Time Disorders diagnosed (in weeks) • A. Non-invasive: • Maternal serum screen: • Alpha feto protein (AFP) 16 Neural tube defects (NTD) • Triple test 16 Down syndrome • Ultrasound 18 Structural defects in many organs as CNS, heart, kidney, and limbs. • B. Invasive: • - Amniocentesis 14 -16 Chromosomal and metabolic abnormalities, and DNA analysis. • - Chorionic villus sampling 10 -12 As amniocentesis. • - Fetal blood sample near term As amniocentesis + blood • disorders.

Can birth defect be treated before birth? Ø Advances in prenatal therapy now make it possible to treat some birth defect before birth Ø Prenatal surgery-urinary tract blockage , rare tumors in lungs, spina bifida
 • Characteristic features of Down syndrome include: upslanting")
Chromosomal abnormalities Trisomy 21 (Down syndrome) • Characteristic features of Down syndrome include: upslanting palpebral fissures • a small head with flat occiput • small nose • small mouth with relatively large tongue • short broad hands with an incurving little finger (clinodactyly) • a single palmar (simian) crease • a wide space between the great toe and second toe (sandal gap),
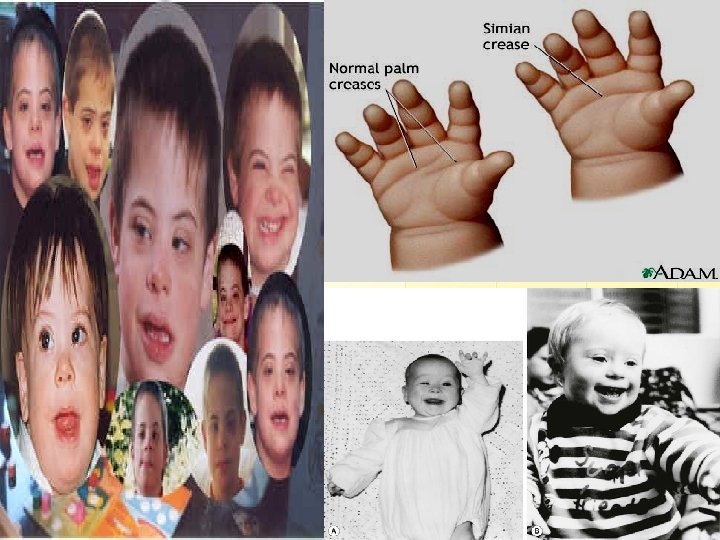

• Brushfield spots in the eyes • generalized hypotonia. • Intelligence quotient is below average, at 40– 80. v Not all of these manifestations need be present and any of them can occur alone without implying chromosomal aberration. v Babies born with Down syndrome also have a higher incidence of cardiac anomalies, cataracts, hearing loss, leukaemia and hypothyroidism v The overall incidence of Down syndrome is 1 in 700.

v Down syndrome arising sporadically as a result of a non disjunction process occurs in 95% of cases. v Unbalanced translocation occurs in 2. 5% of cases, usually between chromosomes 14 and 21 v There is no di�erence between the types in clinical appearance. v Parents who have a baby with Down syndrome, therefore, should be o�ered genetic counselling to establish the risk of recurrence v The parents are likely to require a great deal of emotional support in the first few days following diagnosis.

v Providing audiovisual or reading material about Down syndrome for the parents may be helpful v individual baby's needs will vary depending on whethere any co-existing anomalies. Although initial feeding problems are common owing to generalized hypotonia, v breastfeeding should be encouraged if that is what the mother had planned v Investigations indicated include chromosome analysis and echocardiography,
 ü This condition is found in about 1 in")
v. Trisomy 18 (Edwards syndrome) ü This condition is found in about 1 in 5000 births. ü An extra 18 th chromosome is responsible for the characteristic features. ü The lifespan for these children is short and the majority die during their 1 st year. ü The head is small with a flattened forehead, a receding chin and frequently a cleft palate. ü The ears are low set and maldeveloped. ü Mental deficiency; growth retardation; ü prominent occiput; short sternum; ventricular septal defect , micrognathia, flexed digits,
 ü An extra copy of the 13 th chromosome")
v. Trisomy 13 (Patau syndrome) ü An extra copy of the 13 th chromosome leads to multiple abnormalities. ü These children have a short life. ü Only 5% live beyond 3 years. ü Affected infants are small and are microcephalic. ü Midline facial abnormalities such as cleft lip and palate are common and limb abnormalities are frequently seen. ü Brain, cardiac and renal abnormalities may coexist with this trisomy.
 ü In this monosomal condition, only one sex chromosome exists:")
v. Turner syndrome (XO) ü In this monosomal condition, only one sex chromosome exists: an X. ü The absent chromosome is indicated by ‘O’. ü The child is a girl with a short, webbed neck, widely spaced nipples and oedematous feet. ü The genitalia tend to be underdeveloped and the internal reproductive organs do not mature. ü The condition may not be diagnosed until puberty fails to occur. ü Congenital cardiac defects may also be found. Mental
 ü This is an abnormality affecting boys diagnosed until pubertal")
v. Klinefelter syndrome (XXY) ü This is an abnormality affecting boys diagnosed until pubertal changes fail to occur. ü Small testes, aspermatogenesis; ü Often tall with disproportionately long lower limbs. ü Intelligence is less than in normal siblings. ü Approximately 40% of these males have gynecomastia

thank you L/O/G/O
- Slides: 39