Conference Good prison health better public health safer

Conference Good prison health – better public health – safer society 24 November 2009, Oslo, Norway “Healthier lifestyles for would-be, current and past prisoners - a “silver bullet” or a “red herring”? Dr Mikko Vienonen NDPHS Expert Group SIHLWA SOCIAL INCLUSION, HEALTHY LIFESTYLES & WORK ABILITY

”Silver bullet” was a legendary weapon that was supposed to hit its target every time and in all circumstances


Everyone knows what a herring is ! But what is a red herring?

A red herring is something that really does not exist although someone claims that it does! (“Emperor’s new clothes”)

European health systems recognize and endorse as our fundamental values: Universality Equity Solidarity All citizens – including prisoners – have the same right to health under these fundamental values.

Promotion of healthy lifestyle in prison is neither a silver bullet nor a red herring but a practical tool in the right place at the right time. Loosing an opportunity simply is not very clever inhumane and “bad business” (= expensive to the society)

In our region we have thousands of child-prisoners and 1 -3 million street-children. No need for a miracle, just common sense and decency!

DECLARATION ON PRINCIPLES OF COOPERATION BETWEEN PRISON HEALTH AND PUBLIC HEALTH SERVICES AND DEVELOPMENT OF A SAFER SOCIETY … You cannot ignore prison health issues, as they constitute a fundamental component of public health. Health and well-being of prisoners are beneficial to the society as a whole, including social and economic development. Importance of healthy nutrition, exercise opportunities, tobacco cessation and focus on better mental health and coping skills are seen as a resource for better quality of life in prisons and time after it. [Question: is alcohol a taboo in prison, in spite of its crucial role in landing to prison and problems after it ? Are prison staff immune to alcohol problems? Drugs and HIV are frightening but alcohol is a bigger killer! Including people who work there. ] Drug-free [and smoke-free? ] prison wards should be available for persons wanting treatment for their addiction disorders. Access to substitution therapy and counselling for prisoners in jurisdictions where substitution treatment is available outside of prisons [how about nicotine substitution and treatment? Have inmates access to it if they want? ]. Specific responses to the needs of persons with mental illness, and those who are physically challenged, that are age, language, culturally and gender appropriate. Additional challenge calling for action is the overrepresentation of indigenous populations among prison inmates in some countries.

Leading 12 selected risk factors as causes of disease burden Developed Countries 1. Tobacco 2. Blood pressure = presently the biggest health risk for our working-age population 3. Alcohol ALKOHOL 4. Cholesterol 5. Body mass index 6. Low fruit & veg. 7. Physical inactivity 8. Illicit drugs 9. Unsafe sex 10. Iron deficiency 11. Lead exposure 12. Childhood sexual abuse

Que vadis, Homo Borealis*? * Where are you going, mankind of the North?

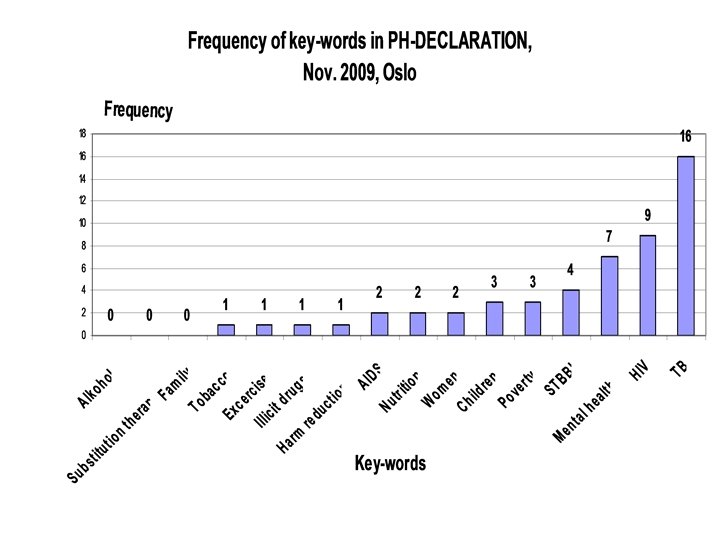
Frequency of key-words in PH-DECLARATION, Nov. 2009, Oslo KEY-WORDS Frequency Alcohol 0 Family 0 Substitution therapy 1 Excercise 1 Harm reduction 1 Illicit drugs 1 Tobacco 1 AIDS 2 Nutrition 2 Women 2 Poverty 3 Children 3 STBBI 4 Mental health/disease 7 HIV 9 TB 16

Why we should make ”Disease Producing Prisons” into “Health Promoting Prisons” 1. Health status among prison population is bad and has not become better during last 20 years (possibly worse? ). 2. 90 % of new inmates in Finland have a disease that needs treatment and/or rehabilitation when addictions (alcohol, narcotics) are included. 3. 50 % of new inmates have a disease other than addiction. 4. Double-triple diagnoses are common. 5. Total morbidity is about 6 times higher (!) than among general population in Finland. 6. Mental disorders are rather a rule than exception. Alcohol and/or drugs often combined with psychiatric problems. 7. What about smoking? Have we given up in prisons? 8. Mental problems self medication with alcohol addiction mental disturbances …. 9. Finland about 3500 inmates at one time 7000 visited prisons every year. Russian Federation roughly one million inmates at one time 2 -3 million visited prisons every year. Yet, ”revolving door” not as common as we think: about 70 % do NOT return. 10. It is not we and them – it is us. We are all mixed. 11. Paradoxically, prison could become an opportunity for a lifestyle change, if properly managed.

How to make ”Disease Producing Prisons” into “Health Promoting Prisons” 1. 2. 3. 4. 5. Health interview and check-up of arriving prisoners (could start already before sentence starts as briefing for to-be prisoners waiting to start their sentence). Health check-ups tend to be somatic and disease oriented and neglecting health and social behavior history (When did smoking start and are you interested to quit? Hazardous and/or harmful alcohol use/ audit? When came drugs into picture? Family violence/abuse? Physical activity/sports? Nutritional habits? BMI/ Body Mass Index, belly circumference – not just weight? Depression? Family: wife/husband/partner, children, parents? Previous prison history? Education? . . . ). Improve health interviews more towards health promotion. Make a genuine effort to map the health risks of inmates thinking that stronger health is a powerful asset for better self-confidence and own life control when freedom is taken away. Time in prison can paradoxically become a window of opportunity. Innovative positive incentives. E. g. drug-free and smoke-free wards/cells better equipped than those which are not. Weight-watchers diets with additional attractions (fruit, coffee, fresh fish, etc. ), Possibilities for physical exercise with modern equipment and attractive practice-hours and quality supervision/coaching. Guarded opportunities to use public swimming pools. Access to nicotine replacement treatment (chewing-gum or plaster), etc. Counseling during prison sentence on available public (municipal) healthylifestyle and sports possibilities and how to get free or subsidized access after release from prison.

How to make ”Disease Producing Prisons “ into “Health Promoting Prisons” Experience from “Terve” (= be healthy) –project (Finland 2006 -07) 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. “Mini-Intervention” (“EIBI”= Early Identification – Brief Intervention on hazardous and harmful use of alcohol/ drugs). Asking how much and how you use alcohol, not just “do you have a problem”. Takes only 5 -10 min. Effectivity is evidence based. As (or more? ) important as blood-pressure measurement. Empowers individual and grass - root interventions. “Healthy prisoner” –courses. Provides addictive substance information and counseling sessions (e. g. in open prisons). Counseling in freedom before arriving to prison and just before release (where to find places for healthy lifestyle support, social and health care services, probation & aftercare services). 5 -6 inmates per one course, 4 -9 sessions, total 8 -18 hours. Recruitment to courses was easy, inmates were motivated. Reaches also those inmates, who in freedom never use places for healthy lifestyle support. Peer-group support a powerful motivator also in prisons. Long term follow up shown that healthy lifestyle support during prison sentence had helped adaptation into civil life and empowered the individual towards better coping and addiction-free life. Lessons learned: “Be healthy”-courses are not yet a routine practice: should be! Collaboration with civil sector services should be made more frequent. More open and unprejudiced discussion of addictive substance policies within prison administration.

Prisons are a work place for thousands of prison workers. Are prisons an occupational health hazard for people working there? Health Promoting Prisons can also promote their workers’ health. 1. 2. 3. 4. 5. 6. “Mini-Intervention” (“EIBI”= Early Identification – Brief Intervention on hazardous and harmful use of alcohol/ drugs) make a ROUTINE part of occupational health services. Appropriate guidelines and policies for work-place drunkenness (alcometer use in case of doubt, zero-tolerance, functional channels for professional counseling and alcohol rehabilitation Smoking cessation opportunities (smoke free prisons like smoke free hospitals, schools, administrative institutions, ministries…). Nicotine replacement therapy free of charge. Tobacco sale in prison kiosks and canteens? Who checks what kiosks sell: chunk food only? Nutritional counseling (BMI/ Body-Mass-Index/belly circumference), healthy food choices in canteens (low-fat, low-sugar, low-salt, high fruit & vegetable, Cholesterol monitoring. What are the criteria for planning prison meals? Has anyone seen an assessment of prison food from health promotion point of view? Physical exercise promotion (free/subsidized access to swimming pools and fitness centers, sports and rehabilitation equipment as additional bonuses for outstanding work Better health consciousness (“literacy”) of prison staff ALL-TOGETHER

Links of life-styles and life-fortunes with “career” as prisoner - should we who are concerned with prison health worry about that? 1. 2. 3. 4. 5. 6. Alcohol use is strongly associated with aggressive and violent behaviour. It increases impulsivity, and decreased awareness of both risk and consequences of one’s action. This all contributes to actions that lead to crime and hence imprisonment. In over 50% of violent crimes alcohol has been at least partly a risk factor. We should actively support national and international prevention initiatives against harmful alcohol use aimed at reducing accessibility and demand for alcohol, in order to prevent crime. Adolescents are a special risk group. Alcohol use is also a risk factor for HIV/AIDS infection (through unprotected sex), and HIV/AIDS disease progression (causing failures in following complicated treatment/medication regimes). Criminal career is more likely to start for young who were neglected (parents, sisters), came from broken-families, and had started using alcohol early. Intervention BEFORE criminal career starts is possible if societies provide resources for it. Presently they are cutting it. General alcohol policy and especially access to children (under 18) does matter. Why do we allow advertisement of a substance which increases crime? The more actively an inmate had participated in alcohol- and/or drugrehabilitation programmes during imprisonment, the more likely he/she considered to be able not to return to criminal behaviour ( ref. RSV 2009: Study on “Short-term prisoners in Finland”)
 but a 1000 times")
OUTRAGE Everyone is afraid of ”swine-flu” (H 1 N 1) but a 1000 times bigger risk is …

ILL-

You must be a Because what healthy you told me is lifestyle Where Yes, absolutely researcher! are we? Thank for your how did you correct but attention! you completely know? useless! The problem Martin Mc. Kee 2003, modified by M. Vienonen 2009 Because you don’t know where you are, you don’t You must know where be a prison you’re going, and Yes. You’re health 30 now you’re How metres policy blaming me! did you above the maker? know? ground in a balloon!
- Slides: 23