Concussion and Neurologic Injury Jamie B Varney M

Concussion and Neurologic Injury Jamie B. Varney, M. D. CAQ Sports Medicine Pikeville Medical Center Orthopedics and Sports Medicine

What is a Concussion? Complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces 1

Cause of Concussion May be caused by direct blow to head, face, neck or elsewhere Thought to be due to axonal injury caused by acceleration forces Not typically a structural injury Electrolyte shifts and release of neurotransmitters and free radicals thought to play role Fuel need/delivery mismatch
 Improper technique Male > Female")
Risk Factors Previous concussion (strongest factor) Improper technique Male > Female

High Risk Sports Football Ice Hockey Soccer Boxing Rugby Field Hockey Lacrosse

Symptoms Headache Loss of consciousness Confusion/Memory Loss Dizziness/Vertigo Nausea/Vomiting Phono/photo phobia Incoordination/Slowed reaction Emotional lability/irritability Sleep disturbance

Symptoms Confusion – Vacant stare – Slow response – Easily distracted – Decreased focus – Disoriented – Slurred speech

Symptoms Memory Deficits – Repeats questions – Retrograde amnesia – Anterograde amnesia (inability to form new memories)

Rare Symptoms Seizure 1% or less Cortical blindness

Evaluation Should be evaluated by trained personnel as soon as suspected injury On Field – Loss of Consciousness – ABC’s – Rule out C-Spine injury assumed if LOC – Neurological Status – Mental Status

Mental Status Orientation Memory Cognitive skills
 – Word recall – Number sequence")
Memory Short term – Events of game (plays/score) – Word recall – Number sequence recall Intermediate – Delayed word recall – Previous games – World events Long term – Teammates/Family members – Birthdates – Presidents

Cognitive skills Serial 7’s Reverse spelling Reverse alphabet Concentration / complex commands

Neurological function Cranial Nerves Motor Sensory Reflexes Cerebellar function/Coordination – Finger/nose – Heel/shin – Gait/Tandem (eyes closed as well) – Rhomberg/ Pronator drift

Additional Exam Skull for depressions Cervical spine tenderness Nose for clear drainage Ears for hemotympanum Signs of skull fracture
 Maddock's Questions Modified BESS")
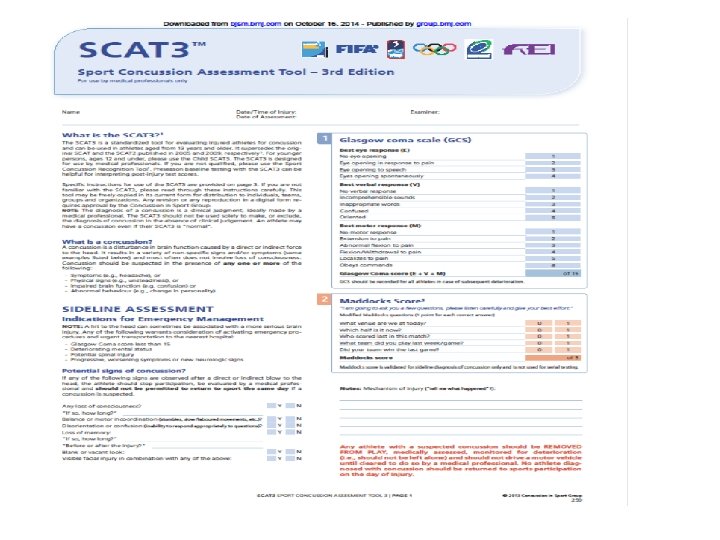
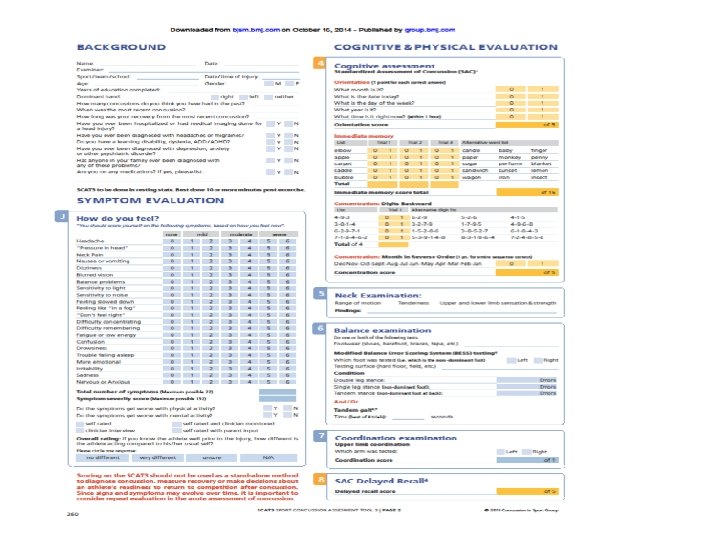
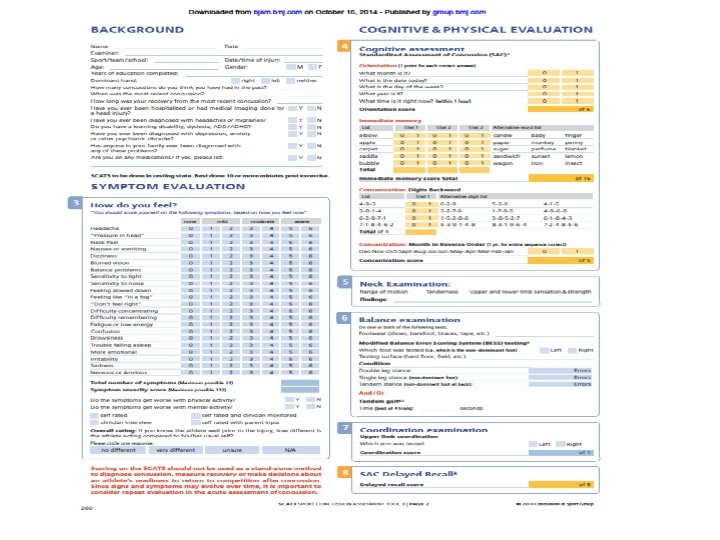
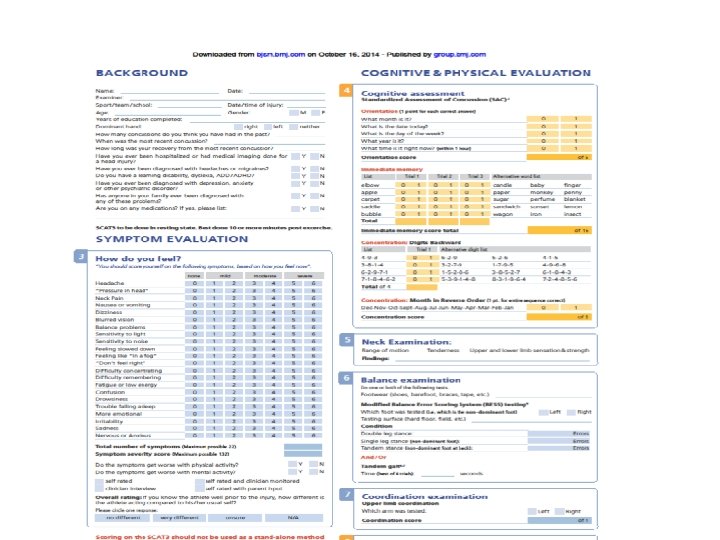
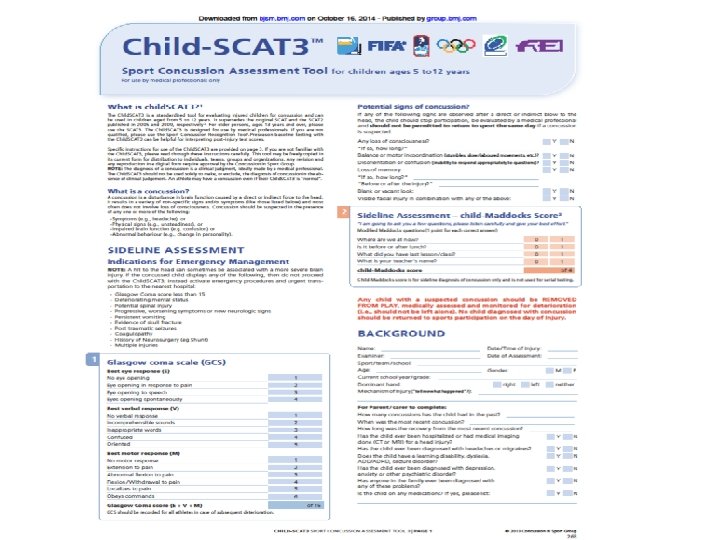
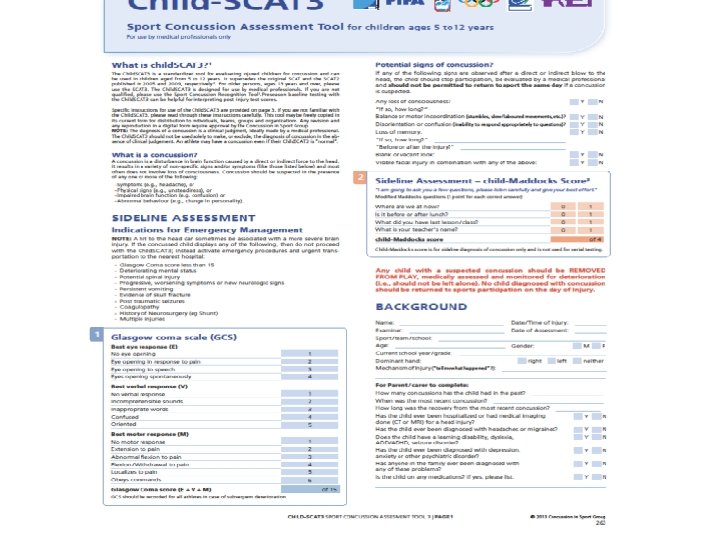
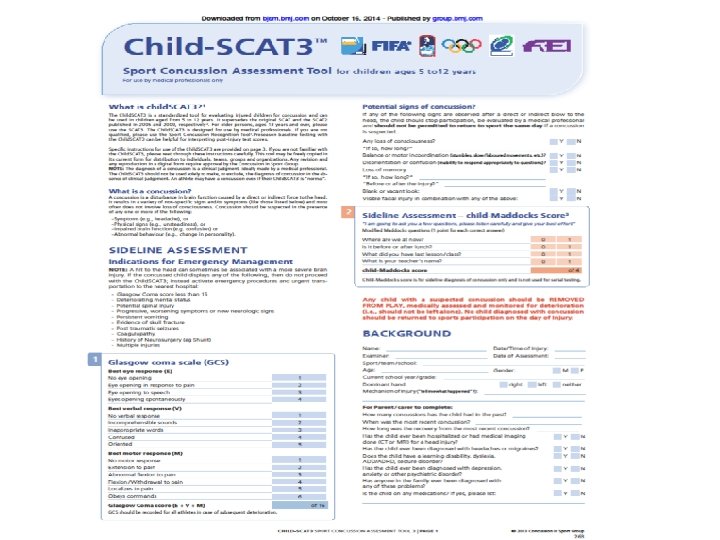
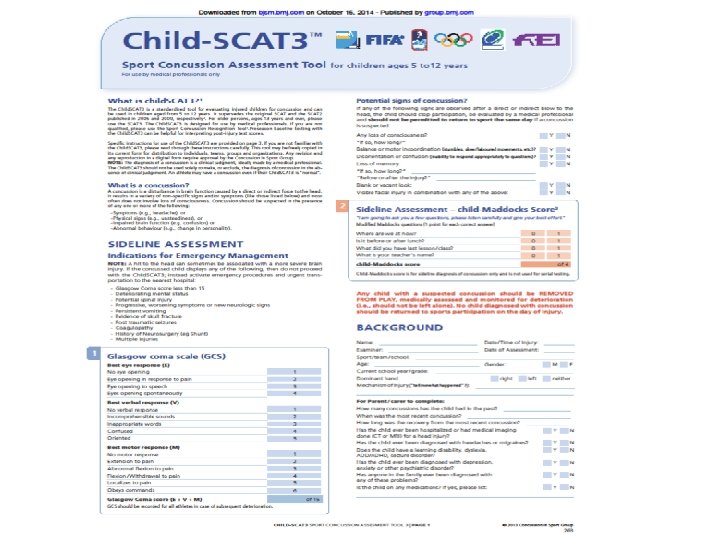
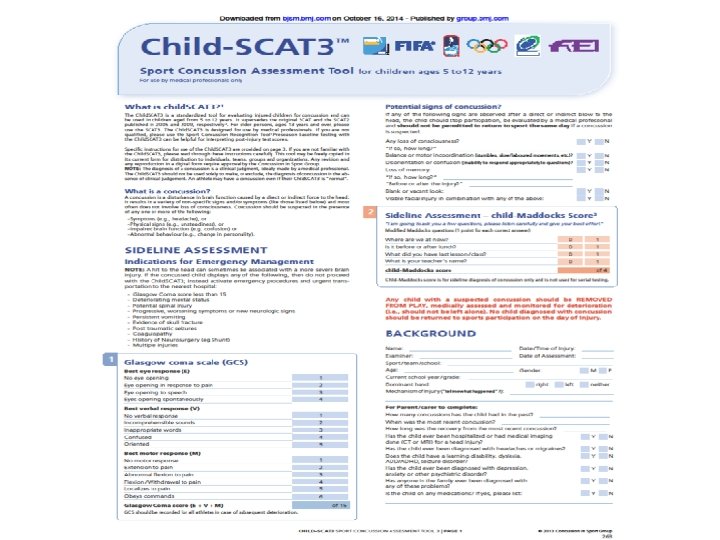
Sideline Tools SCAT 3>13 y/o Standardized Assessment of Concussion (SAC) Maddock's Questions Modified BESS –Balance Error Scoring System Child SCAT 3 <13 y/o

SCAT 3 Demo

Neuroimaging Typically normal CT preferred if necessary MRI more sensitive but may not correlate with severity or outcome Possible future role for functional MRI

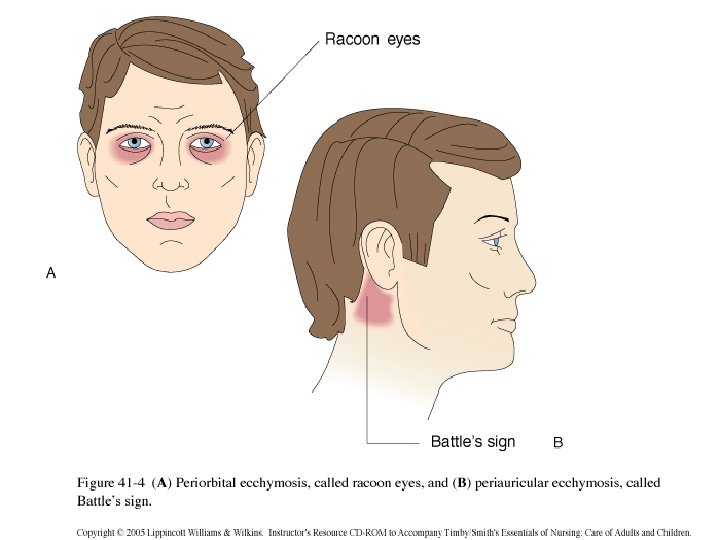
Recommended Imaging Neurological deficit Suspected C-Spine injury Suspected skull fracture – Raccoon eye’s – Battle’s Sign – Rhinorhea – Hemotympanum Seizure Coagulopathy / Anticoagulant use Progressive symptoms

Consider Imaging Canadian CT criteria – GCS <15 two hours after injury – Two or more episodes vomiting – Age > 65 – Amnesia longer than 30 min prior – Dangerous mechanism MVA Fall > 3 ft or 5 stairs
 – Headache – Vomiting – Age >60")
Consider Imaging New Orleans Criteria (GCS 15) – Headache – Vomiting – Age >60 – Drug/ETOH intoxication – Persistent anterograde amnesia – Visible trauma above clavicle

Comparison Two studies have shown both are 100% sensitive for detecting neurosurgical abnormalities One study showed higher sensitivity for clinically significant findings with New Orleans (99. 4% vs 87. 2%) Canadian CT rules more specific – Lowered CT rates 52. 1% versus 88% – Other study specificity 39. 7% vs 3%

Bottom Line 1 Imaging usually not helpful for concussion Helpful to rule out bleeds if progressive symptoms or clinical suspicion

Hospital Admission GCS <15 Abnormal CT scan Seizures Bleeding diasthesis or anticoagulants Consider if no one available to monitor for progression of symptoms

Outpatient Monitoring Monitor Closely 1 st 24 hrs Educate about warning signs – Somnolence/Confusion – Worsening headache – Vision difficulties – Vomiting or stiff neck Neurological deficits Avoid strenuous activity
 Cantu")
Grading Concussion Old system • • • Colorado American Academy of Neurology (AAN) Cantu • Prague Statement 2004 – Simple <10 days – Complex >10 days/seizures/prolonged LOC • Zurich Statement 2012 – Forget Grades

Return to Play 1 No same day play • KHSAA and NCAA Physical Rest Until Asymptomatic Consider Cognitive Rest Exercise Testing

Progressive Return To Play 1 Step 1 No activity, rest, when symptom free without meds go to step 2 • Step 2 • Light aerobic exercise, no resistance training • Step 3 • Sport specific exercise • Step 4 • Non Contact Practice and Resistance Training • Step 5 • Full Contact Practice • Step 6 • Full Game

Office Exertional Maneuvers • Treadmill/Bike • Sprints/Run in place • Sit-ups, Push-ups

Progressive RTP If symptoms develop at any step stop and rest. Do not proceed. ATC's are invaluable resource More conservative in children with focus on cognitive rest and return to learn before return to play

Second Impact Syndrome Occurs after second injury before first injury has healed Diffuse cerebral swelling that can be life threatening Few cases with documentation that is consistent with description May only require minor injury

Post traumatic Epilepsy Seizure within 1 st week not epilepsy Mild TBI associated with twofold risk epilepsy in 5 years
 –")
Post Concussive Syndrome Not related to severity of injury Symptoms >3 months (DSMIV) – Headache – Dizziness – Fatigue – Irritability – Anxiety/Depression – Insomnia – Loss of concentration or memory – Cognitive impairment

Post Concussive Syndrome Treatment – Consider referral – Treat symptoms
 Mood Disorders Dementia Movement Disorders")
Chronic Traumatic Encephalopathy (CTE) Mood Disorders Dementia Movement Disorders

Neuropsychiatric Testing Paper tests interpreted by experienced neuropsychologist Computerized Tests

Neuropsychiatric Testing Speed of information processing Memory Attention Concentration Reaction Time Scanning Visual tracking Problem solving

Neuropsychiatric Testing Tested at baseline then post injury if needed More sensitive than classic testing Concern is maybe too sensitive and not specific enough

Prevention Proper equipment / fitting Proper training for coaches and support staff Enhancement and enforcement of protective rules Pre-participation evaluation of concussion history

Other Neurological Injury C-Spine Brachial Plexus Transient Cord Neuropraxia

Other Neurological Injury C-Spine Brachial Plexus Transient Cord Neuropraxia

Brachial Plexus Injury Commonly called stinger / burner Caused by stretch or compression Unilateral symptoms – Weakness – Numbness – Stinging pain C 5 -6 most common If has bilateral symptoms think cord injury

Brachial Plexus Injury Single episode – May return when no pain or neurologic deficit Recurrent episode – Consider evaluation including flex/ext xrays and canal diameter If symptoms last more than 1 week consider MRI/EMG to rule out cord lesion

Stinger/Burner
 Neck rolls/cowboy collars")
Prevention Rehab to strengthen neck/shoulders Proper hitting technique Proper equipment (pads) Neck rolls/cowboy collars

Transient Cord Neuropraxia Flexion/extension injury with underlying spinal stenosis Post traumatic neurological findings Bilateral symptoms of paresthesia and or weakness Upper > Lower extremities Lasts minutes to days If occurs must evaluate with imaging for cord injury and spinal canal diameter

Torg Ratio of spinal canal to vertebral body Ratio <0. 8 suggestive of stenosis MRI measurement of cord vs. canal diameter more reliable

Treatment If have transient neuropraxia then protect cervical spine until fracture ruled out Must evaluate canal diameter which may imply risk of future injury Neurosurgeon familiar with treatment should help make any return to play decision

References 1. Mc. Crory, P. et al. Consensus Statement on Concussion in Sport (Zurich Statement 2012). Br J Sports Med 2013; 47: 250 -258 2. Meehan, WP, O'Brien, MJ. Sports. Related Concussion in Children and Adolescents: Clinical Manifestations and Diagnosis. Up. To. Date. 9 -22 -14
- Slides: 60