Computed Tomography Imaging in Intestinal Obstruction By Naguib

Computed Tomography Imaging in Intestinal Obstruction By Naguib Naeem Assistant Lecturer, Faculty of Medicine, Alexandria University, Egypt. Visiting Radiologist, Frankfurt University Hospital, Germany.

• Intestinal obstruction accounts for at least 20 percent of all admissions to an emergency surgical service. • Obstruction of the intestine occurs when there is impairment in the normal flow of luminal contents caused by an extrinsic or intrinsic encroachment on the lumen. • Intestinal pseudoobstruction, or adynamic ileus, can mimic mechanical obstruction, but differs in that the underlying problem is due to disordered motility.

Intestinal Obstruction Classification: • According to the level of obstruction into high or low small-bowel, colonic. • According to rate of progression of the obstruction into acute, chronic, or acute-onchronic. • According to the presence or absence of peristalsis into dynamic (mechanical) and adynamic.

Diagnosis of bowel obstruction: • The diagnosis of intestinal obstruction is usually suspected on the basis of clinical signs and patient history but the clinician needs to know whether obstruction is present and if so, the level and cause, and whether strangulation is present.

• A variety of imaging investigations are possible these include: 1. Plain X-ray to the abdomen and pelvis. 2. Contrast studies (small bowel followthrough, entercolysis or small bowel enema, contrast enema) 3. Computed Tomography. 4. Ultrasonography. 5. Magnetic Resonance Imaging.

Thus our aim when we examine a case of intestinal obstruction is to answer the following questions: 1. 2. 3. 4. 5. Is there intestinal obstruction? If yes, is it mechanical or functional? What is the level of obstruction? What is the cause of obstruction? Is the obstruction of the simple type or the closed loop type? 6. Are there signs of threatened bowel wall viability or not?

Important anatomical facts: The thickness of the wall of the small bowel is ordinarily 2 to 3 mm when the lumen is distended (defined as 2 cm or greater luminal diameter). The small bowel generally is considered dilated if the luminal diameter exceeds 3 cm. The thickness of the wall of the normal colon is usually less than 3 mm. Walls that measure 4 -6 mm are considered suspicious and walls over 6 mm must be considered definitely abnormal. The allowable diameter of the colon varies depending on the anatomic segment of colon.

The valvulae conniventes appear as discrete folds perpendicular to the long axis of the small bowel lumen and are observed in the jejunum and are not observed in the distal ileum. These folds should not exceed 3 mm in thickness.

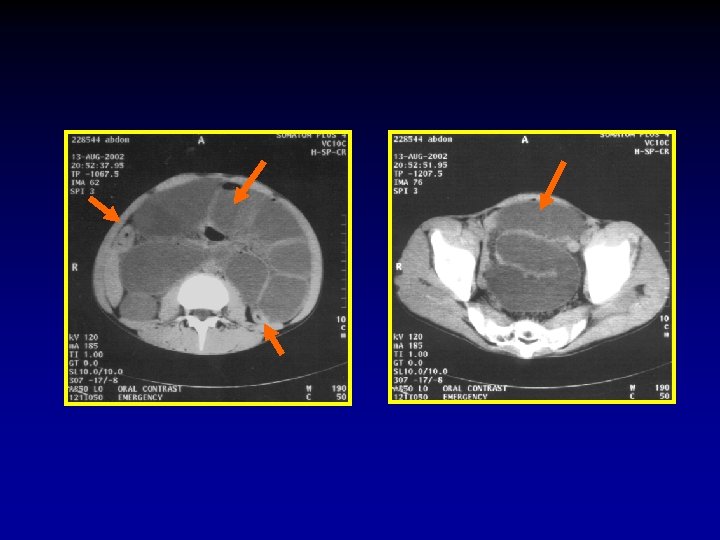
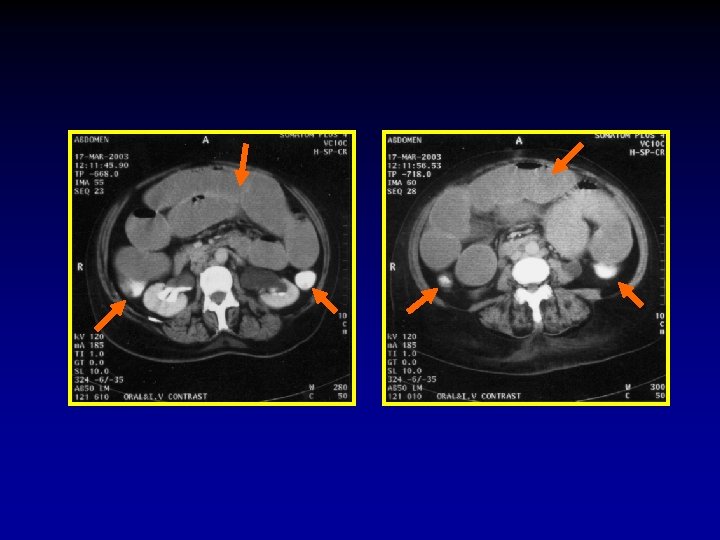
1. Is there intestinal obstruction? 2. If yes, is it mechanical or functional? • The diagnosis of mechanical bowel obstruction by CT relies on the demonstration of marked discrepancy in the caliber of the bowel i. e. the presence of dilated bowel loops followed by collapsed loops (transitional zone). • The diagnosis of functional obstruction is based on the presence of dilated loops with no transitional zone.

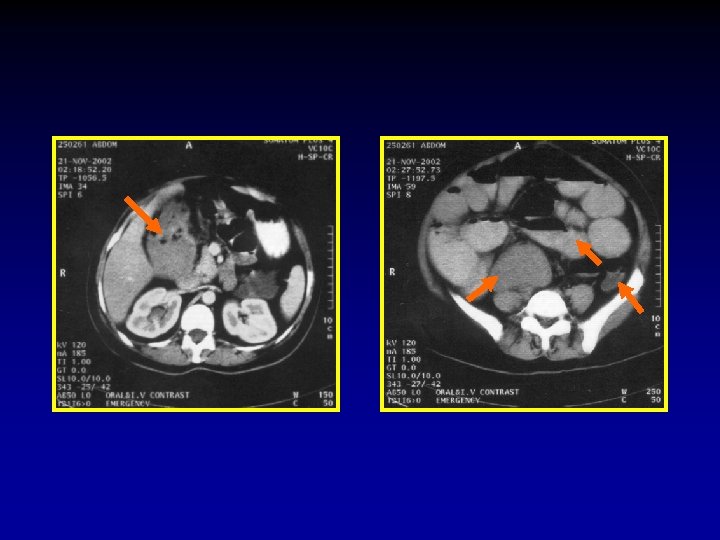
3. What is the level of obstruction? In order to detect the exact level, systematic evaluation should begin at the rectum and proceed towards the caecum. Once the colon is cleared one should attempt to identify the distal ileal loops then proceed up. A common error is to assume that loops in more caudal images are ileal loops and jejunal loops in the proximal images, in fact when the bowel loops dilate they align themselves along the axis of the mesentery thus jejunal loops may appear in the pelvis and ileal loops in the upper abdomen. In small bowel obstruction the transverse colon will not be seen because it is compressed against the anterior abdominal wall by the tensely distended small bowel loops.

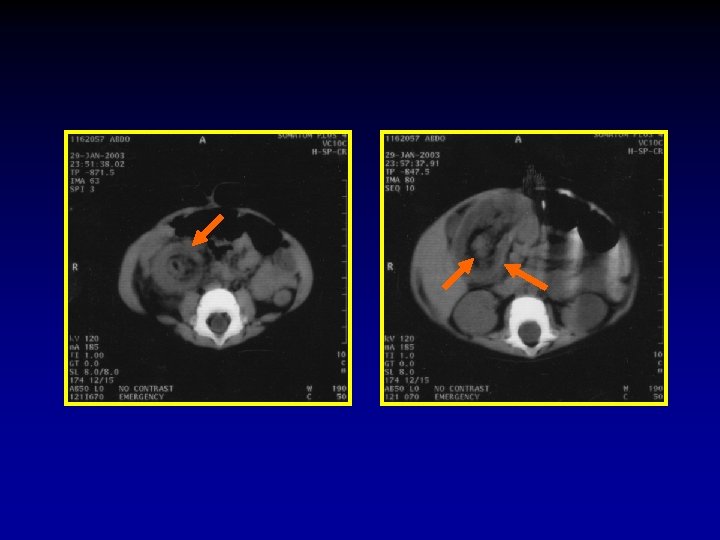
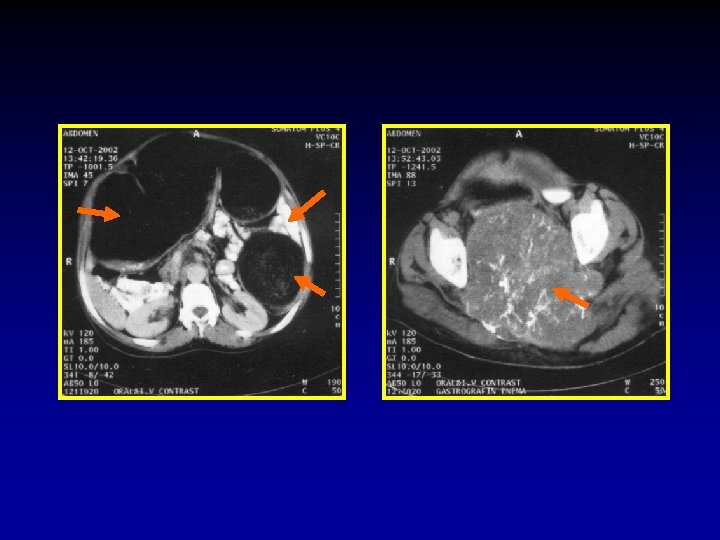
4. What is the cause of obstruction? Causes of mechanical bowel obstruction: Causes of mechanical small bowel obstruction: 1. Adhesions. 2. Hernia. 3. Neoplasms e. g. Lymphoma. 4. Inflammatory e. g. Crohn’s disease. 5. Intramural obstruction e. g. gall stones, food. . etc. 6. Iatrogenic.

Causes of Mechanical large bowel obstruction: 1. Carcinoma. 2. Diverticulitis. 3. Volvulus. 4. Hernia. 5. Inflammatory stricture. 6. Fecal impaction. 7. Foreign body. 8. Extrinsic disease e. g. adhesions, pelvic abscess. . .

Causes of functional bowel obstruction: 1. Post operative ileus. 2. Peritonitis. 3. Metabolic disorders e. g. hypokalemia. 4. Mesenteric vascular occlusion. 5. Drug induced. 6. Systemic disorders e. g. sepsis, shock…. 7. Neurologic disorders.

5. Is the obstruction of the simple type or the closed loop type? Mechanical intestinal obstruction is divided into two types; – – Simple obstruction Closed loop obstruction. In simple obstruction the bowel is occluded at one point along its course.

In closed loop or incarcerated intestinal obstruction, a loop of bowel is occluded at two adjacent points along its course as a result of a single constrictive lesion. Mechanical large bowel obstruction with competent ileocaecal valve can be considered a closed loop obstruction. The subsequent twisting of the involved loop results in Strangulation which is defined as a closed-loop obstruction associated with intestinal ischemia.

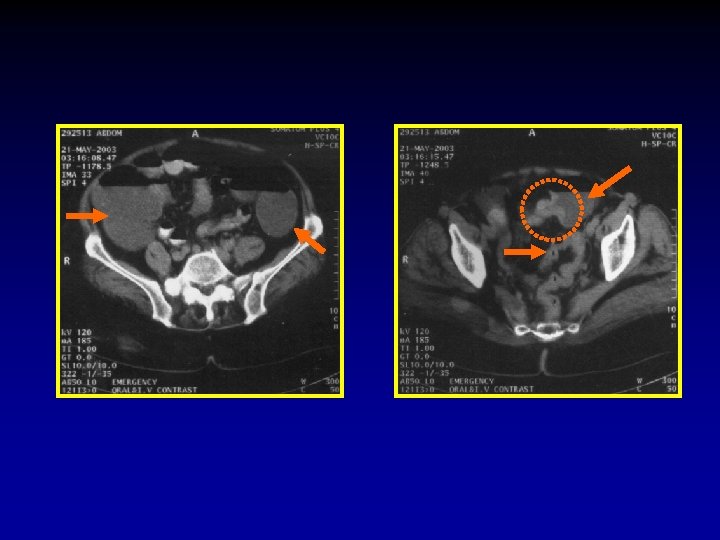
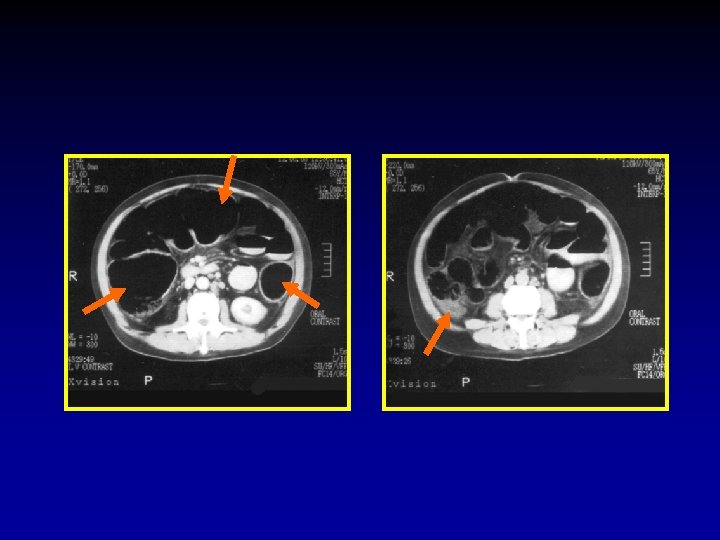
The CT signs of closed loop obstruction of the small intestine are: 1. Evidence of small bowel obstruction. 2. A U-Shaped or radial configuration of the fluid filled dilated loops. 3. At the site of obstruction, a whirl sign, beak sign, triangular loop, or two adjacent collapsed loops.

A At U-Shaped the site Evidence of configuration obstruction of. The small Whirl of two bowel theadjacent sign fluid obstruction. filled collapsed dilatedloops

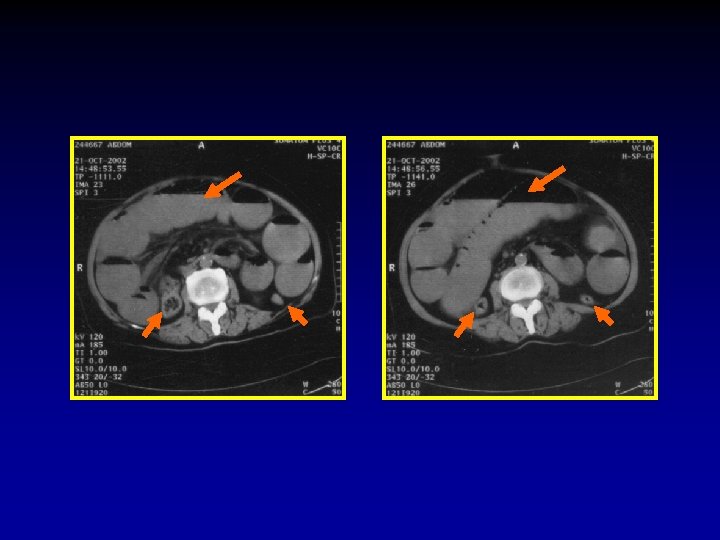
6. Are there signs of threatened bowel wall viability or not? The CT signs of threatened bowel wall viability: 1) Thickening of the bowel wall with or without the target sign. 2) Pneumatosis (Air in the bowel wall). 3) Portal venous gas. 4) Increased density of the bowel wall without intravenous contrast administration. 5) Mesenteric haziness, fluid, or hemorrhage often associated with generalized ascites. 6) On intravenous contrast enhanced CT, non enhancement, or rarely increased enhancement of the bowel.

Thickening of. Pneumatosis Engorgement the bowel Mesenteric Associated wall (Air of with Mesenteric in. Haziness Ascites the or bowel without Vessels wall) the target sign

Conclusions 1. CT is a very accurate tool in diagnosing patients with mechanical bowel obstruction and in differentiating mechanical from non mechanical obstruction of the bowel. 2. CT can detect the site of obstruction (whether it is small or large bowel obstruction) and can accurately predict the exact level of obstruction. 3. CT can identify the cause of obstruction in a high percentage of patients. The accuracy of CT is improved by knowing the patient’s history especially the history of previous operations. 4. CT diagnosis of adhesions as a cause of bowel obstruction is based on being unable to find a cause of obstruction at the transitional zone.

5. CT can differentiate between simple loop and closed loop bowel obstruction. 6. By its ability to image the bowel wall CT can detect signs of threatened bowel wall viability but none of these signs is specific. So the diagnosis of threatened bowel wall viability is based on finding a combination of these signs in a single patient

Thank You
- Slides: 30