Composite Restorations Tooth Preparation Introduction Composite can be

Composite Restorations- Tooth Preparation

Introduction Composite can be used for most clinical applications where a successful bond with enamel and dentin is possible to achieve. Bonding to tooth structure requires an environment isolated from contamination by oral fluids or other contaminants. The ability to isolate the operating area (usually by a rubber dam or cotton rolls) is a major factor in selecting a composite material for a restoration. If the operating area cannot be totally protected from contamination, a nonbonded amalgam restoration may be the material of choice.
2 has indicated the appropriateness of composites for use")
Indications The American Dental Association (ADA)2 has indicated the appropriateness of composites for use as: 1. Class I, III, IV, V, and VI restorations (Moderate sized class I and II) 2. Foundations or core buildups 3. Sealants and preventive resin restorations (conservative composite restorations) 4. Esthetic enhancement procedures Partial veneers Full veneers Tooth contour modifications Diastema closures 5. Cements (for indirect restorations) 6. Temporary restorations 7. Periodontal splinting

The ADA does not support the use of composites in: teeth with heavy occlusal stress, sites that cannot be isolated, or If patients who are allergic or sensitive to composite materials. composites are used as indicated, the ADA further stated, “… the expected lifetime of resin-based composites can be comparable to that of amalgam in Class I, Class II, and Class V restorations. ”

Tooth Preparation for Composite Restorations The tooth preparation for a composite restoration includes the following 1. Removing the fault, defect, old material, or friable tooth structure 2. Creating prepared enamel margins of 90 degrees or greater (>90 degrees usually preferable) 3. Creating 90 -degree (or butt joint) cavosurface margins on root surfaces/ Amalgam vs composite Less outline extension (adjacent suspicious or at-risk areas [grooves or pits] may be “sealed” rather than restored) An axial or pulpal wall (or both) of varying depth (not uniform) Incorporation of an enamel bevel at some areas (the width of which is dictated by the need for secondary retention or esthetics)

Tooth Preparation for Composite Restorations The design of the tooth preparation for composite restoration may vary depending on several factors. There are five basic designs which may be used individually and/or in combination. The designs are (1) conventional, (2) bevelled conventional, (3) modified, (4) box-only, and (5) slot preparation.

Conventional design It’s similar to those used for amalgam restorations. The primary indications for conventional tooth preparation in composite restorations are (1) preparations located on root surfaces (nonenamel areas) and (2) moderate to large Class I or II restorations. In moderate to large Class I or II composite restorations, there may be increased need for resistance form, which the conventional amalgam-like preparation design provides.

Class I or II conventional composite preparations should be prepared with as little faciolingual extension as possible and should not routinely be extended into all pits and fissures on the occlusal surface where sealants may be otherwise indicated.

Beveled Conventional Similar to conventional preparations in the outline form having external boxlike walls, but with some beveled enamel margins. Indicated when a composite restoration is being used to replace an existing restoration (usually amalgam) exhibiting a conventional tooth preparation design with enamel margins or to restore a large area. This design is most typical for Classes III, IV, and V restorations. The beveled conventional preparation design is rarely used for posterior composite restorations.
, Class IV (C and")
Beveled conventional preparation designs for Class III (A and B), Class IV (C and D), and Class V (E and F) restorations

Modified preparation design These preparations have neither specified wall configurations nor specified pulpal or axial depths; appear to have been “scooped out” rather than having the distinct internal line angles characteristic of a conventional preparation design These preparations are highly conservative, preferably have enamel margins, and rely on the composite bond to tooth structure to retain the restoration in the tooth. Indications: primarily for the initial restoration of smaller, cavitated, carious lesions usually surrounded by enamel and for correcting enamel defects. Class III, IV and V
, Class IV (C and D),")
Modified preparation designs for Class III (A and B), Class IV (C and D), and Class V (E and F) restorations

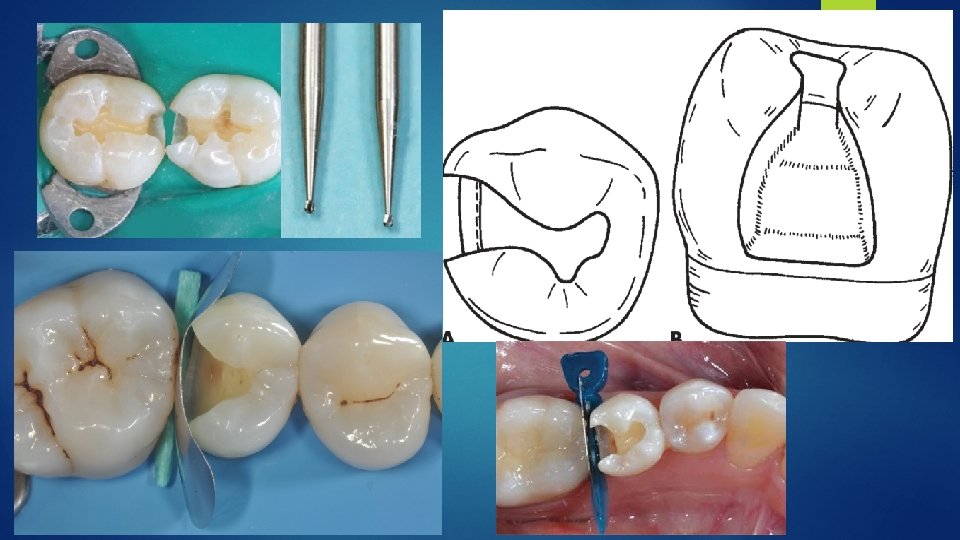
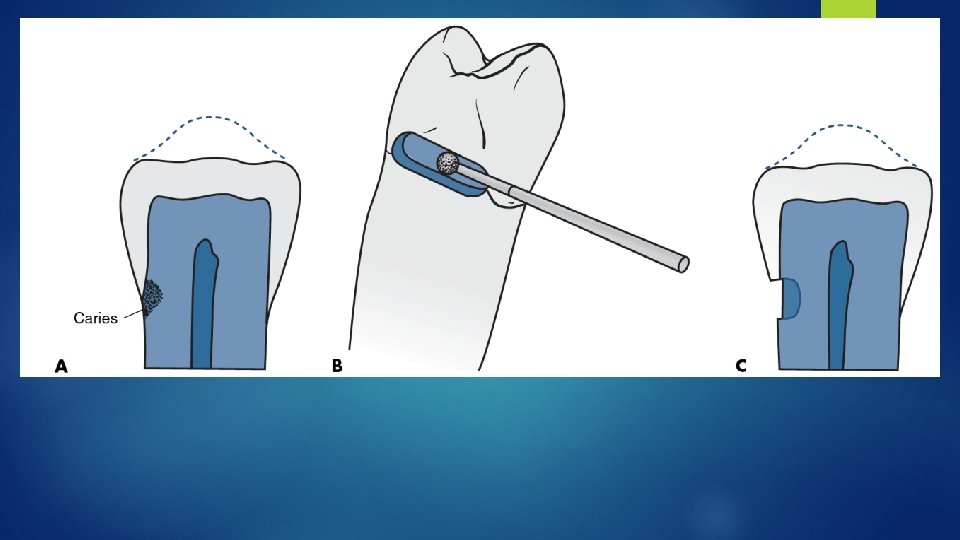
Box-Only Design A modified design, indicated when only the proximal surface is faulty, with no lesions present on the occlusal surface. A proximal box is prepared with an inverted cone or round diamond stone or bur held parallel to the long axis of the tooth crown. The facial, lingual, and gingival extensions are dictated by the fault or caries. Neither beveling nor secondary retention is usually indicated.
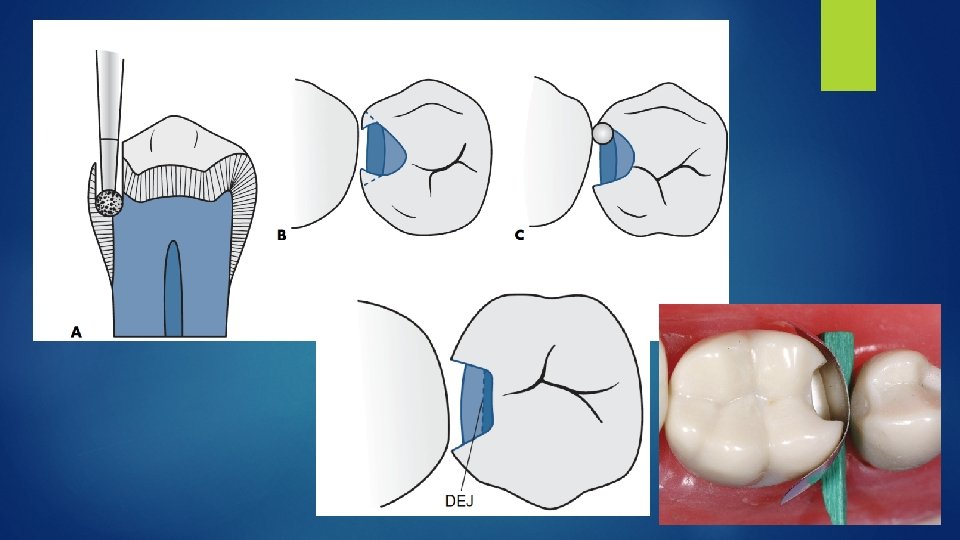

Facial or Lingual Slot Indicated for subcontact lesions on proximal surface which can be approached through a lingual or a buccal approach. Advantage: marginal ridge is preserved. This preparation is similar to a Class III preparation for an anterior tooth The instrument ( round diamond or bur) is oriented at the correct occlusogingival height, and the entry is made with the instrument as close to the adjacent tooth as possible, preserving as much of the facial or lingual surface as possible. Extent of preparation is determined by extent of lesion.

Features Of Composite Restorations Different From Amalgam 1. Less outline extension (adjacent suspicious or at-risk areas [grooves or pits] may be "sealed" rather than restored) 2. An axial and/or pulpal wall of varying depth (not uniform) 3. Incorporation of an enamel bevel at some areas (the width of which is dictated by the need for secondary retention) 4. Tooth preparation walls being rough (to increase the surface area for bonding) 5. Use of a diamond stone (to increase the roughness of the tooth preparation walls)

Guiding principles of adhesive cavities Black’s concept of extension for prevention is no longer valid. The current paradigm is rather prevention of extension. Cavity outline form cavity outline internal and external, is only dictated by the extent of the caries. Once carious dentin is removed, no further removal of tooth substance is required.

Retention Macroretentive interlocking designs have changed to retention by means of micromechanical (interlocking of resin tags into the retentive pattern of etched tooth tissues), submicromechanical (hybrid layer, horizontal branching between dentin tubules, surface roughness of tubules) and chemical adhesion (ion-exchange layer of glass ionomers). Placement of a bevel increases the potential surface area for retention by a more transverse cut of enamel prisms (enhanced etch pattern) and by extending the surface area of the preparation available for bonding. Cervical margins should only be beveled if the margin is well above the cemento-enamel junction
, p 246, 253. Etched dentin")
SEM of Etched Dentin Etched dentin Moist Sturdevant (2002), p 246, 253. Etched dentin Dry
 Total Etch")
Dentin bonding (monomeric resin) Total Etch
 Self-Etch")
Dentin bonding (monomeric resin) Self-Etch

Resistance Resistance of both tooth and restorative material to resist fracture. Loose and fragile enamel rods should be removed, but unsupported tooth structure may be conserved and weakened tooth may be reinforced by the bonded restoration. 90 -degree cavosurface angles are given for GIC. Long bevel design for composite. If the margin is under functional loading the margin in that area might have a cavosurface angle that approaches 60 to 80 degrees. Occlusal bevels should not be utilized for posterior composite preparations. After caries removal, the internal cavity features rounded characteristics, straight internal walls and defined line angles are no longer required for adhesive materials

Amalgam CR Compressive 380 -500 220 -300 Longevity 10+ yr 5+ yr 2° Caries 50 39 Technique sensitive Moisture sensitive Condensation Many Sensitive Corrosion Delayed expansion Very sensitive Retention Microleakage Max Min Tooth prep

Amalgam CR Outline Defects No extension for prevention Defects Retention: undercut Adhesive Etching Resistance • No undermined E • Remaining tooth structure • Sufficient depth, 1. 5 mm • Depth • Bond • Surface area of the etched enamel Convenience Yes

Line Angle Amalgam CR Line angle Def slightly rounded Rationale Retention Resistance (conservative tooth prep)

Margin of Restoration Margin Rationale Amalgam CR 90 degree amalgam margin Resistance Retention Bevel Emargin 45 º Retention Esthetics Resistance
 CR")
Resistance Form Amalgam Tooth Restoration Enamel Rod Dentin support Thickness (1. 5 mm) CR Enamel Rod Bonded surface area Bond strength

Retention of Restoration Amalgam CR Slight convergent Box Retention Undercut Rationale No bonding to tooth structure Adhesive Etching Bonding: E>D, C Preparation
 – polymerization shrinkage (Cfactor)")
Retention of CR Restoration = bonding surface (area and etching) – polymerization shrinkage (Cfactor) + water abs.

Selection of Restorative Materials Amalgam-CR-GIC High caries risk: need F Supragingival margin: moisture sensitive Cementum gingival margin Cervical abrasion: wear Dentin substrate: sclerotic dentin(? ), depth preparation, tubule orientation Abfraction: flexion Pros: retentive wear of

- Slides: 33