Components of the Comprehensive Geriatric AssessmentCGA MAHSA ZAREEI
 MAHSA ZAREEI GERIATRITION IUMS")


: distance vision near vision glare disability night")




 set distance (6, 8,")



 “In the last year,")








 The maximum score for the MIS is 8 • 5")

")
 The scale consists of 30 yes/no questions. normal 0 -9")



: 6 item Toilet Feeding Dressing Grooming (neatness, hair, nails,")

 8 item Ability to Use Telephone Shopping Food")





- Slides: 40
Components of the Comprehensive Geriatric Assessment(CGA) MAHSA ZAREEI GERIATRITION IUMS
Visual Impairment Snellen eye chart Activities of Daily Vision Scale VF-14 VFQ-25 Cataract Symptom Scale
patient to stand 20 ft from the chart and read letters, using corrective lenses. Patients fail the screen if they are unable to read all the letters on the 20/40 line with their eyeglasses (best corrected vision)
the Activities of Daily Vision Scale (ADVS): distance vision near vision glare disability night driving daytime driving Each subscale score between 100 (no visual difficulty) and 0 (inability to perform the activity because of visual difficulty)
Items included in the 17 -item Quality of Life and Vision Function Questionnaire Item no. Description Subscale 1. Does quality of vision prevent you from performing daily activities normally? 2. Are you unhappy about your visual condition? 3. How much are you concerned with a possible worsening 4. Because of your visual problems do you feel less inclined to meet people/friends/relatives? 5. Because of your visual problems do you feel useless or a burden to others? 6. Because of your vision do you have problems crossing a street? 7. Because of your vision do you bump against other people when in crowded areas? 8. Because of your vision do you have problems in perceiving a dip on the ground or step?
9. Because of your vision do you have problems in reading prices in a shop window? 10. Because of your vision do you have problems in recognizing people across the street? 11. Because of your vision do you have problems in recognizing a person in a crowded room? 12. Because of your vision do you have problems in reading an article in a newspaper or names/numbers in the telephone directory? 13. Because of your vision do you have problems in doing a manual activity such as cooking, sewing, cutting your nails? 14. Does your vision deteriorate in bright light? Self-assessment of sensory adaptation (light-dark adaptation, glare) 15. Does your vision deteriorate in dim light? Self-assessment of sensory adaptation (lightdark adaptation, glare) 16. Do you have a driving license? If “YES”: how much is your driving disturbed by the lights of oncoming cars? If “NO”: how much is your vision disturbed by the lights of oncoming cars? Self-assessment of sensory adaptation (light-dark adaptation, glare) 17. How much problem do you have in recognizing colors? Self assessment of color vision
Hearing Impairment Audio scope Single question: “Do you think you have a hearing loss? ” Whisper test Hearing Handicap Inventory for the Elderly
Audio scope
whispering: three to six random words (numbers, words, or letters) set distance (6, 8, 12, or 24 in) from the person’s ear asking the patient to repeat the words. The examiner should be behind the person the opposite ear should be covered or occluded during the examination. Patients fail the screen if they are unable to repeat half of the whispered words correctly.
Hearing Handicap Inventory for the Elderly The higher the HHIE-S score, the greater the handicapping effect of a hearing impairment. referral is recommended for individuals scoring 10 or higher on the inventory.
Malnutrition/Weight Loss Malnutrition Screening Tool, which asks two questions “Have you been eating poorly because of a decreased appetite? ” “Have you lost your weight recently without trying? ) Mini-Nutritional Assessment (MNA)
Mini-Nutritional Assessment
Urinary Incontinence Asking two questions can screen for incontinence: (1) “In the last year, have you ever lost your urine and gotten wet? ” and if so, (2) “Have you lost urine on at least six separate days? ” 3 IQ questionnair
1. During the last 3 mo, have you leaked urine (even a small amount? ) NO YES: 2. During the last 3 mo, did you leak urine: (Check all that apply. ) a. When you were performing some physical activity, such as coughing, sneezing, lifting, or exercise? b. When you had the urge or the feeling that you needed to empty your bladder, but you could not get to the toilet fast enough? c. Without physical activity and without a sense of urgency? 3. During the last 3 mo, did you leak urine most often: (Check only one. ) a. When you were performing some physical activity, such as coughing, sneezing, lifting, or exercise? b. When you had the urge or the feeling that you needed to empty your bladder, but you could not get to the toilet fast enough? c. Without physical activity and without a sense of urgency? d. About equally as often with physical activity as with a sense of urgency? Definitions of type of urinary incontinence are based on response to question 3: Response to Question 3 Type of Incontinence
Balance and Gait Impairments and Falling Timed up and go Gait speed over 10 m Office-based maneuvers: Observed gait Resistance to nudge Tandem/semitandem stand Rising from chair 360° turn Functional reach Short physical performance battery
The timed “up and go” test timed measure of the patients’ ability to rise arm chair, walk 3 m (10 ft), turn, walk back, and sit down again those who take longer than 20 seconds to complete the test should receive further evaluation.
Gait speed is also a helpful marker for recaurrent falls. Patients who take more than 13 seconds to walk 10 m are more likely to have recurrent falls
Functional reach It is reported that a reach of 15 cm may predict a fall.
“ ” Short physical performance battery
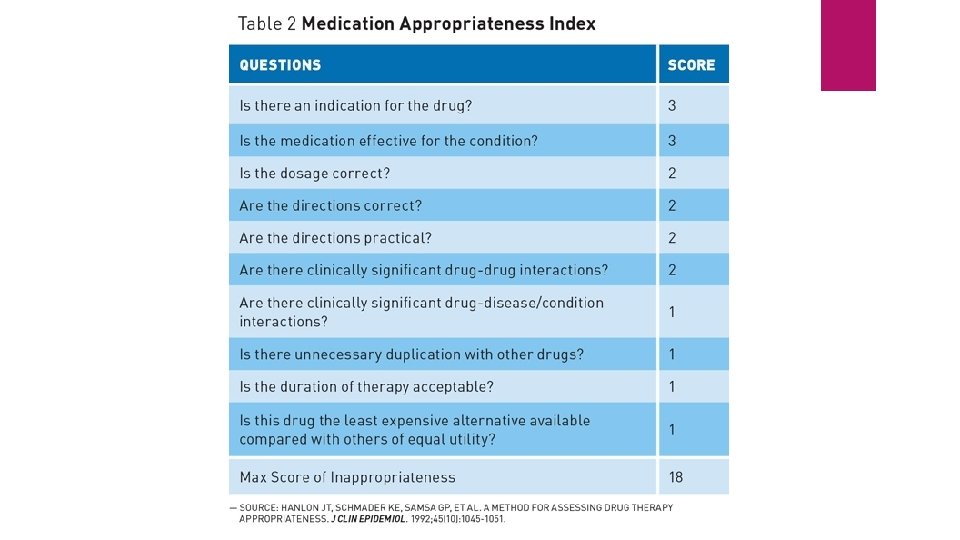
Polypharmacy Beers criteria
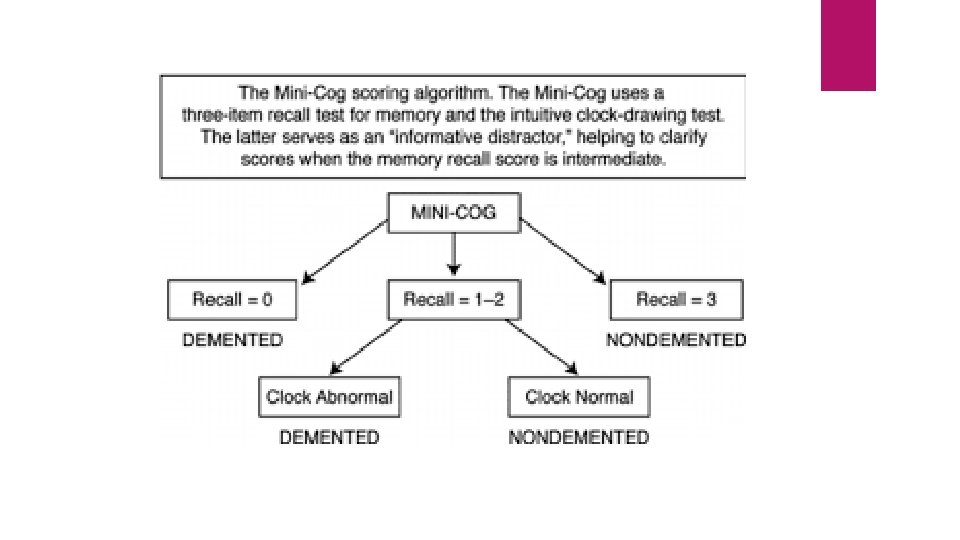
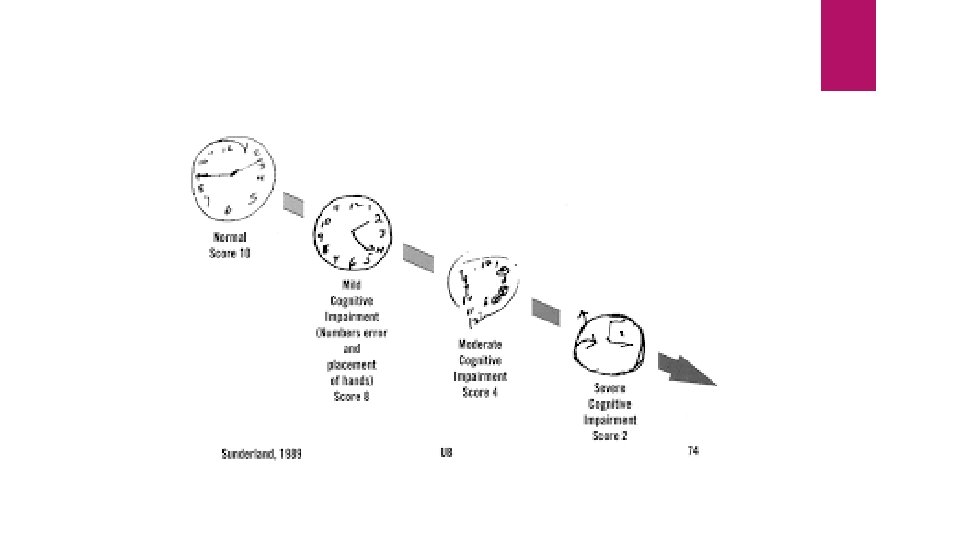
Cognitive Assessment Mini-Cog MIS MMSE Mo. CA
MEMORY IMPAIRMENT SCREEN (MIS) The maximum score for the MIS is 8 • 5 -8 No cognitive impairment • ≤ 4 Possible cognitive impairment
1. Show patient a sheet of paper with the 4 items and ask patient to read the items aloud. 2. Tell patient that each item belongs to a different category. Give a category cue and ask patient to indicate which of the words belongs in the stated category (eg, “Which one is the game? ”). Allow up to 5 attempts. Failure to complete this task indicates possible cognitive impairment. 3. When patient identifies all 4 words, remove the sheet of paper. Tell patient that he or she will be asked to remember the words in a few minutes. 4. Engage patient in distractor activity for 2 to 3 minutes, such as counting to 20 and back, counting back from 100 by 7, spelling WORLD backwards. 5. FREE RECALL — 2 points per word: Ask patient to state as many of the 4 words he or she can recall. Allow at least 5 seconds per item for free recall. Continue to step 6 if no more words have been recalled for 10 seconds. 6. CUED RECALL — 1 point per word: Read the appropriate category cue for each word not recalled during free recall (eg, “What was the game? ”).
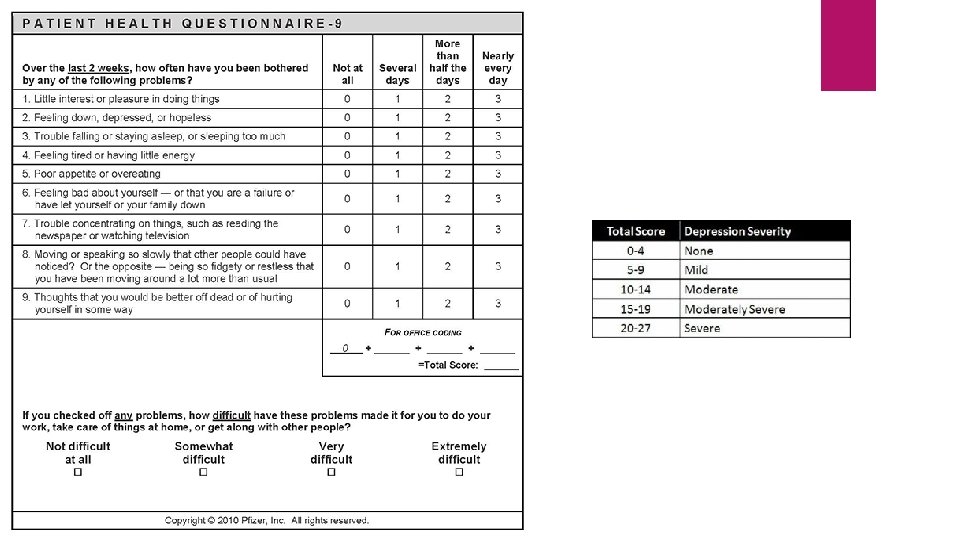
Affective Assessment Geriatric depression scale Patient Health Questionnaire-9 (PHQ-9)
Geriatric depression scale (GDS) The scale consists of 30 yes/no questions. normal 0 -9 mild depressives 10 -19 severe depressives 20 -3
GDS 1. Are you basically satisfied with your life? YES / NO 2. Have you dropped many of your activities and interests? YES / NO 3. Do you feel that your life is empty? YES / NO 4. Do you often get bored? YES / NO 5. Are you hopeful about the future? YES / NO 6. Are you bothered by thoughts you can t get out of your head? YES / NO 7. Are you in good spirits most of the time? YES / NO 8. Are you afraid that something bad is going to happen to you? YES / NO 9. Do you feel happy most of the time? YES / NO 10. Do you often feel helpless? YES / NO 11. Do you often get restless and fidgety? YES / NO 12. Do you prefer to stay at home, rather than going out and doing new things? YES / NO 13. Do you frequently worry about the future? YES / NO 14. Do you feel you have more problems with memory than most? YES / NO
15. Do you think it is wonderful to be alive now? YES / NO 16. Do you often feel downhearted and blue? YES / NO 17. Do you feel pretty worthless the way you are now? YES / NO 18. Do you worry a lot about the past? YES / NO 19. Do you find life very exciting? YES / NO 20. Is it hard for you to get started on new projects? YES / NO 21. Do you feel full of energy? YES / NO 22. Do you feel that your situation is hopeless? YES / NO 23. Do you think that most people are better off than you are? YES / NO 24. Do you frequently get upset over little things? YES / NO 25. Do you frequently feel like crying? YES / NO 26. Do you have trouble concentrating? YES / NO 27. Do you enjoy getting up in the morning? YES / NO 28. Do you prefer to avoid social gatherings? YES / NO 29. Is it easy for you to make decisions? YES / NO 30. Is your mind as clear as it used to be? YES / NO
Assessment of Function ADL IADL AADL
Activity of daily living (ADL): 6 item Toilet Feeding Dressing Grooming (neatness, hair, nails, hands, face, clothing) Physical Ambulation Bathing
Example Toilet : Score 1: 1. Care for self at toilet completely; no incontinence Score 0: 2. Needs to be reminded, or needs help in cleaning self, or has rare (weekly at most) accidents 3. Soiling or wetting while asleep more than once a week 4. Soiling or wetting while awake more than once a week 5. No control of bowels or bladder
Instrumental activity of daily living: (IADL) 8 item Ability to Use Telephone Shopping Food Preparation Housekeeping Laundry Mode of Transportation Responsibility for Own Medications Ability to Handle Finances
• ADLs, the total score ranges from 0 to 6, and for IADLs, from 0 to 8. • In some categories, only the highest level of function receives a 1; in others, two or more levels have scores of 1 because each describes competence that represents some minimal level of function. • These screens are useful for indicating specifically how a person is performing at the present time. When they are also used over time, they serve as documentation of a person's functional improvement or deterioration.
Example Ability to Use Telephone Score 1: 1. Operates telephone on own initiative; looks up and dials numbers. 2. Dials a few well-known numbers. 3. Answers telephone, but does not dial. Score 0: 4. Does not use telephone at all.
Assessment of Social Support family friends neighbors caregivers
Others: Economic Assessment Environmental Assessment safety Spirituality Advance Directives
THANKS FOR YOUR ATTENTION