COMPLICATIONS OF SINUSITIS Dr Nayana V G Senior













 ♦Inflammation extends into the tissues of the")


 ♦Inflammatory process ophthalmic veins")
























- Slides: 43
COMPLICATIONS OF SINUSITIS Dr. Nayana. V. G Senior Resident YMC
Definition Defined as any adverse progression of chronic or acute bacterial infection beyond the paranasal sinuses, or compromise in function of any part of the body due to local or distant effects of the condition.
Specific learning objective • To know the definition of complication of chronc rhinosinusitis and local and distant complications of acute and chronic rhnosinusitis • To learn the orbital complication of sinusitis and know the pathophysiology of intracranial complication of sinusitis and list of the intra cranial complication • To know in brief about bony complication , ear , laryngeal complication and distant complication and mucocele of paranasal sinuses
Classification Acute Frontal Local Ethmoid Maxillary Sphenoid Distant Chronic Orbital Intracranial Bony Septicaemia Toxic shock syndrome Mucocele Pyocele Oroantral fistula
According to the sites involved Ø Orbital Ø Intracranial Ø Bony Ø Nasal Ø Pharyngeal and laryngeal Ø Ear
Orbital complications v Orbital cellulitis v Orbital abscess v Retrobulbar neuritis v Superior orbital fissure syndrome v Orbital apex syndrome
Intracranial v. Meningitis v. Encephalitis v. Extradural abscess v. Subdural abscess v. Brain abscess v. Cavernous sinus thrombosis
Bony v Osteomyelitis v Potts puffy tumor
Nasal v v Chronic rhinitis Secondary atrophic rhinitis Chronic hypertrophic rhinitis Nasal polyposis
Pharyngeal and laryngeal v Lateral wall pharyngitis v Granular pharyngitis v Pharyngo laryngitis v Tonsillitis Ear v Otitis media with effusion v CSOM
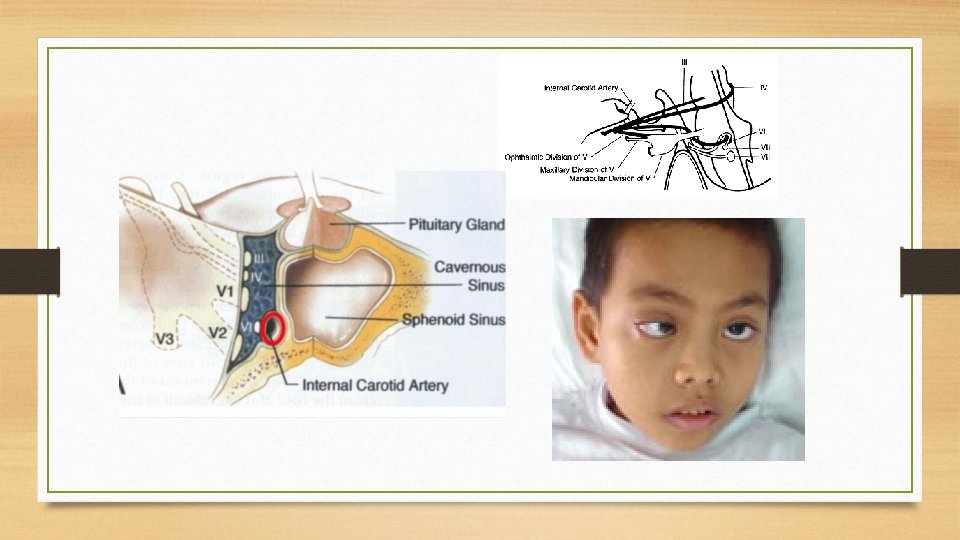
Orbital Complications Pathophysiology ♦Close proximity to PNS especially ethmoid ♦Congenital dehiscence in the lamina papyracea ♦Valve less superior and inferior ophthalmic veins ♦Thrombophlebitis and interference with venous drainage of the orbital contents Microbiology – Strepto / Staph / Anaerobes
Chandler classification 1970 ♦Preseptal cellulitis ♦Orbital cellulitis without abscess formation ♦Orbital cellulitis with subperiosteal abscess ♦Orbital cellulitis with intra periosteal abscess ♦Cavernous sinus thrombosis
Pre septal cellulitis ♦Occurs as a result of impaired venous drainage of the ethmoid vessels which are obstructed by inflammation and pressure. ♦Inflammation does not extend beyond the orbital septum ♦Edema of the lids ♦without tenderness / Visual loss or limitation of extra ocular mobility
Post septal cellulitis (orbital cellulitis without abscess) ♦Inflammation extends into the tissues of the orbit causing diffuse edema of the orbital contents without abscess ♦Eyelid edema, erythema, proptosis and chemosis ♦ limited or no impairment of EOM with normal visual acuity
Subperiosteal abscess ♦Abscess formation deep to orbital periosteum ♦Proptosis ♦Impaired EOM with visual loss
Orbital abscess ♦Abscess formation within the orbit ♦Severe exophthalmos, chemosis, complete ophthalmoplegia ♦Visual impairment – optic neuropathy ♦Irreversible blindness
Orbital Complications Cavernous sinus thrombosis (Both intracranial and orbital complication) ♦Inflammatory process ophthalmic veins into cavernous sinus which thromboses and progress to abscess formation ♦Abrupt onset , Bilateral eye involvement. ♦Fever with chills & rigor ♦Rapidly progressive severe chemosis & proptosis ♦ 3, 4, 5, 6, nerve involvement , Loss of vision, dilated &fixed/sluggishly reacting pupil ♦Severe retinal engorgement. congestion & edema of optic disc ♦Meningitis-death
Orbital Complications –Radiography
Superior orbital fissure syndrome ♦Sphenoid sinusitis affects-superior orbital fissure ♦Deep orbital pain , frontal headache, progressive paralysis of 3, 4, 5 a&6
Orbital apex syndrome Superior orbital fissure syndrome & optic nerve with maxillary division of trigeminal nerve involvement
Intracranial complications Pathophysiology v v Close relation of paranasal sinuses to anterior and middle skull base Routes of spread -hematogenous or direct extension Retrograde septic thrombophlebitis Direct extension 1. Preformed routes like congenital or traumatic dehiscence 2. Sinus wall erosion 3. Existing neurovascular foramina like for optic and olfactory nerves, infraorbital foramen
Clinical features • History of recent URI with fever and symptoms of raised intracranial pressure. • Frontal or retroorbital head ache, nausea , vomiting, altered mental status • Nuchal rigidity, papilledema • Late finding- seizures, hemiparesis
Intracranial complications 1. Meningitis 2. Encephalitis 3. Epidural abscess 4. Subdural abscess 5. Intracerebral abscess 6. Venous sinus thrombosis
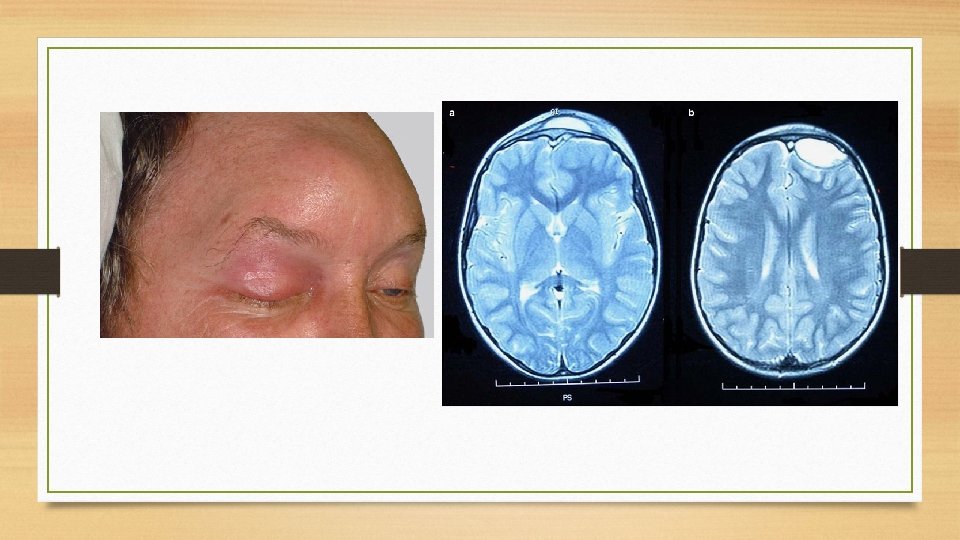
MRI- Focal defects of enhancement with decreased cavernous carotid artery flow void MR angiogram MR venogram studies
Bony complications -Osteomyelitis • Infection of bone marrow. • Involve maxilla or frontal bone 1. Osteomyelitis of frontal bone Adults not in children or infants where frontal bone not developed. Direct or venous spread Pus form externally as pott’s puffy tumour/ internally as extradural abscess Treatment: Antibiotic, drainage of abscess, trephination of frontal bone , removal of necrotic bone or sequestra,
2. Osteomyelitis of maxilla{Second premolar and first molar dental root } Seen in infants and children because of spongy bone in anterior wall of maxilla 1. Secondary to dental infection – most common cause 2. Primary maxillary sinus infection Clinical features: Erythema, Swelling of cheek, oedema of lower lid, purulent nasal discharge and fever Subperiosteal abscess followed by fistula in infraorbital region, alveolus, palate/zygoma, Epiphora , Dental abscess Treatment: antibiotic, drainage of abscess, removal of sequestra
Chronic complications - Mucocoele • Chronically expanding cystic lesion of the paranasal sinuses , lined by pseudostratified or low columnar epithelium containing goblet cells resulting in bony erosion and subsequent extension beyond the sinuses • Etiology 1. Due to chronic obstruction of sinus ostium 2. Dilatation of mucus gland
Clinical features Fronto ethmoid -89% due to complexity of drainage Ethmoid-8% Sphenoid-2% Maxillary sinus-1% <5% bilateral and or multi loculated
Frontal mucocele ♦Superomedial quadrant of orbit Cystic & nontender swelling with eggshell crackling ♦Frontal headache ♦Deep nasal or periorbital pain ♦Proptosis and Diplopia-due to orbital displacement in a downward, outward &lateral direction ♦Xray - Clouding of sinus, loss of scalloped outline & sclerosis
Ethmoid mucocele ♦Expansion of medial wall of the orbit with forward& lateral displacement ♦Bulge in the middle meatus orbital
Sphenoid mucocoele ♦Headache with occipital, vertex or deep nasal pain ♦Exophthalmos ♦ 3, 4, 6, along with ophthalmic &maxillary division of trigeminal - Ophthalmoplegia, diplopia, visual field disturbances v Pituitary disturbances
Maxillary mucocele ♦Usually asymptomatic ♦Symptomatic when natural ostium gets blocked ♦Sinus fills with mucus &expansion of the bony wall ♦Radiological finding ♦CT or MRI
Mucus retention cyst of maxillary sinus Usually does not cause bone erosion Air shadow will be present
Pyocele ♦Mucocele when infected becomes pyocoele ♦Contents are purulent ♦Stapylococcus, H influenzae, streptococcus pnuemoniae ♦Pyocele on rupturing causes-fistula through upper eyelid ♦Proptosis ♦Optic nerve stretching - causes blindness
Oroantral fistula ♦Communication between antrum & oral cavity ♦Situated on the alveolus or gingivobuccal sulcus ♦Regurgitation of food ♦Foul smelling discharge through the nose & through fistula ♦Inability to build positive or negative pressure
Distant complications Toxic shock syndrome ♦Fever, hypotension, rash with desquamation ♦Multisystem failure Septicaemia ♦Hyperventillation, disorientation, confusion ♦Manifestations of encephalopathy
Associated conditions Or descending infection Cystic fibrosis/bronchiectasis Nasal ♦Chronic rhinitis ♦Secondary atrophic rhinitis ♦Chronic hypertrophic rhinitis ♦Nasal polyposis
Pharyngeal&laryngeal 1. Laryngitis 2. Lateral pharyngitis -hypertrophy of lateral lymphoid bands behind posterior pillar 3. Tonsillitis Ear 1. OME 2. CSOM
Summary ♦ Orbit –most common structure involved CT with contrast of the sinuses and orbit > study of choice to evaluate orbital complications ♦ MRI with contrast – of brain and orbit is the study of choice for intracranial complications ♦ Common organism - strep pneumoniae, staph aureus, H – influenzae, moraxella, gram negative rods ♦ Intracranial complications are often poly microbial ♦ CVST- bilateral orbital pain, chemosis, proptosis and ophthalmoplegia ♦ Most common intracranial complications- meningitis- strep pneumoniae ♦ Intracranial abscess are associated with high mortality , neurological and developmental sequelae ♦ Osteomyelitis of frontal bone-----, potts puffy tumour ♦
Reference. . 1. Disease of Ear, Nose, Throat &Head and Neck surgery – PL Dhingra, Shruthi Dhingra Acknowledgement Images from google images and text book(Disease of Ear, Nose, Throat &Head and Neck surgery – PL Dhingra, Shruthi Dhingra)
Thank you