Complications of fractures Done by Selena abboud Rand

Complications of fractures Done by: Selena abboud Rand Alshayeb Rahaf Hasanain

COMPLICATIONS OF FRACTURES General Local Early Late

General complications 1 - Blood loss 2 - Shock *Hypovolemic or hemorrhagic shock. *Septic shock. *Neurogenic shock. 3 - Fat embolism. 4 - Pulmonary embolism. 5 - Crush syndrome. 6 - Multiple organs failure syndrome (MOFS). 7 - Thrombo-embolism.

shock • follows a mismatch of metabolic demand to oxygen delivery at tissue level, leading to cellular hypoxia and (if uncorrected) to tissue and organ failure. • The causes of circulatory shock can be classified as abnormalities of cardiac output, of systemic vascular resistance, or a combination of both • HYPOVOLAEMIC SHOCK: Reduced circulating volume causing a reduction in venous return and cardiac output (e. g. haemorrhage) • Neurogenic shock : when spinal cord injury at a cervical or high thoracic level leads to loss of sympathetic tone and peripheral vasodilatation, venous pooling and reduced venous return.

*Management -ABC -Oxygen -fluids -Inotropes/vasopressors: if the patient remains hypotensive despite adequate fluid resuscitation -systemic support for other organs

Fat embolism • Circulating fat globules occlude small blood vessels, occur after closed fractures of long bones and traces of fat can be found in the lungs and other internal organs. • Source : bone marrow • more common in patients with multiple fractures. *Clinical features • Early warning signs of fat embolism (usually within 72 hours of injury) are 1 - slight rise of temperature and pulse rate. 2 - breathlessness , mental confusion , restlessness. 3 - Pathognomonic signs are petechiae on the trunk, neck, axillae and conjunctiva. 4 - Severe cases: respiratory distress and coma, due to brain emboli and hypoxia from involvement of the lungs. The features at this stage are essentially those of ARDS.

• There is no test for fat embolism ABG and Urinalysis • Management -supportive -oxygen -stabilization of long-bone fractures -analgesia -corticosteroids for severe multiple injuries(methylpredinosolone to maintain oxygen tension) -heparin or dextran ( improve capillary flow)

Crush syndrome • when a limb is compressed for extended periods – underperfusion - myonecrosis release of toxic metabolites – reperfusion injury - Membrane damage and capillary fluid reabsorption failure – swelling - may lead to compartment syndrome - more tissue damage from ischaemia. • The compromised limb is pulseless , red, swollen , blistered; sensation and muscle power may be lost. • prevention. • high urine flow is encouraged with alkalization of the urine with sodium bicarbonate, prevents myoglobin precipitating in the renal tubules. • If compartment syndrome develops, and is confirmed by pressure measurements, then a fasciotomy is indicated. Excision of dead muscle must be radical to avoid sepsis. (( open wound then this should be managed)). (( no open wound and compartment pressures are not high, risk of infection is lower if early surgery is avoided))
 is the clinical appearance of a poorly controlled")
Multiple organ failure syndrome • (MODS) is the clinical appearance of a poorly controlled severe systemic inflammatory reaction, following a triggering event such as infection, inflammation or trauma. • the classical form of MODS appears to progress through four clinical phases: 1. Shock (hypoperfusion). 2. Period of active resuscitation. 3. Stable hypermetabolism (systemic inflammatory response). 4. Organ failure • Management: Prevention, remove risk factors, oxygen, treat underlying cause

Local complications - Early 1. 2. 3. 4. 5. 6. 7. 8. 9. Visceral injury Vascular injury. Nerve injury. Compartment syndrome. Haemoarthrosis. Infection. Gas gangrene. Fracture blisters. Plaster and pressure sores

VISCERAL INJURY * Fractures around the trunk are often complicated by injuries to underlying viscera. 1) rib fractures : A. pneumothorax - penetration of the lung B. Spleen trauma C. Liver injury 2) pelvic fractures - rupture of the bladder or urethra. *These injuries require emergency treatment.

VASCULAR INJURY * The fractures most often associated with damage to a major artery are those around the knee and elbow, and those of the humeral and femoral shafts. * The artery may be cut, torn, compressed or contused either by the initial injury or subsequently by jagged bone fragments. * Even if its outward appearance is normal, the intima may be detached and the vessel blocked by thrombus, or a segment of artery may be in spasm. *The effects vary -transient diminution of blood flow -profound ischaemia -tissue death -peripheral gangrene.

Injury First rib fracture/clavicle artery Shoulder dislocation Humeral supracondylar fracture Elbow dislocation Pelvic fracture internal iliac artery Femoral supracondylar fracture Knee dislocation Proximal tibial its branches Temporal/ parietal Vessel Subclavian Axillary artery Brachial artery Presacral and Femoral artery Popliteal artery or middle

Clinical features - paraesthesia or numbness in the toes or the fingers. -The injured limb is cold, pale, or slightly cyanosed. -pulse is weak or absent. -paralysis -pain • If a vascular injury is suspected an angiogram should be performed immediately; if it is positive, emergency treatment must be started without further delay Treatment � � � All bandages/splints removed The fracture re X-Rayed Circulation reassessed for next half hour If no improvement, do vessels exploration Suture torn vessels, vein grafting, if thrombosed do endarterectomy Aim: to restore blood flow

NERVE INJURY * Nerve injury is particularly common with fractures of the humerus or injuries around the elbow or the knee. Closed nerve injuries -The nerve is seldom severed. -spontaneous recovery awaited – occurs in 90% within 4 months. If no recovery by the expected time, and if nerve conduction studies fail to show evidence of recovery, the nerve should be explored. - By sharp edge of a bone Open nerve injuries -Nerve injury is more likely to be complete. -The nerve should be explored at the time of debridement and repaired at the time or at wound closure. -by agent causing fracture Acute nerve compression -Distinct from a direct injury, with fractures or dislocations around the wrist. Complaints of numbness or paraesthesia in the distribution of the median or ulnar nerves should be taken seriously and the patient monitored ; if there is no improvement within 48 hours of fracture reduction or splitting of bandages around the splint, nerve should be explored and decompressed

Nerve Trauma Effect Axillary Dislocation of shoulder Deltoid paralysis Radial Fracture of humerus Wrist drop Median radial Ulnar Humeral Supracondylar fracture Pointing index Humeral Fracture of medial epicondyle dislocation of hip Claw hand Knee dislocation Foot drop Sciatic Common peroneal Foot drop

COMPARTMENT SYNDROME • Fractures of the arm or leg can cause ischaemia, even if there is no damage to a major vessel. • Bleeding, oedema or inflammation (infection) may increase the pressure within one of the osseofascial compartments- reduced capillary flow - muscle ischaemia – oedema - greater pressure - more profound ischaemia • swelling of a limb inside a tight plaster cast. – a vicious circle that ends after 12 hours or less, in necrosis of nerve and muscle within the compartment. • Nerve is capable of regeneration but muscle, once infarcted, can never recover and is replaced by inelastic fibrous tissue (Volkmann’s ischaemic contracture). • High-risk injuries are fractures of the 1 - elbow 2 - forearm bones 3 - proximal third of the tibia 4 - multiple fractures of the hand or foot 5 - crush injuries and circumferential burns. 6 - operation (usually for internal fixation) 7 - infection
, altered")
• The earliest of the ‘classic’ features are pain ( ‘bursting’ sensation), altered sensibility and paresis (weakness in active muscle contraction). -Skin sensation repeatedly checked- • Ischaemic muscle is highly sensitive to stretch. (pain) When the toes or fingers are passively hyperextended, there is increased pain in the calf or forearm. • Confirmation of the diagnosis is by measuring the intra compartmental pressures. • A differential pressure (ΔP) – the difference between diastolic pressure and compartment pressure – of less than 30 mm. Hg is an indication for immediate compartment decompression • A split/ wick catheter

• • Nerve damage may result in motor and sensory loss. In extreme case gangrene Treatment -Decompression of the compartment. - Casts, bandages and dressings must be completely removed. -The limb should be nursed flat (elevating the limb causes a further decrease in end capillary pressure and aggravates the muscle ischaemia). -The ΔP monitored; if it falls below 30 mm. Hg, immediate open fasciotomy is performed. In the case of the leg, ‘fasciotomy’ means opening all four compartments through medial and lateral incisions. The wounds should be left open and inspected 2 days later: if there is muscle necrosis, debridement can be carried out; if the tissues are healthy, the wounds can be sutured (without tension) or skin-grafted. • if the clinical signs are ‘soft’, the limb should be examined at 30 -minute intervals and if there is no improvement within 2 hours of splitting the dressings, fasciotomy should be performed. • Muscle will be dead after 4– 6 hours of total ischaemia.
")
HAEMARTHROSIS • Fractures involving a joint , leads to accumulation of blood. • (features) The joint is swollen and tense and the patient resists any attempt at moving it. The blood should be aspirated before dealing with the fracture.

INFECTION • Open fractures may become infected; closed fractures hardly ever do unless they are opened by operation. • Post-traumatic wound infection is now the most common cause of chronic osteitis. • Wound becomes inflamed and starts draining seropurulent fluid. • Infection may be superficial, moderate (osteomyelitis), severe (gas gangrene).

Treatment: -Antibiotic -Excising all devitalized tissue -If there is pus formation : tissue around the fracture should be opened & drained

GAS GANGRENE especially Clostridium welchii Produced by anaerobic organisms : Clostridium sp infections. These organisms can survive and multiply in ↓ O 2 tension Toxins produced will destroy the cell wall and leads to tissue necrosis Clinical features: within 24 hr. Patient complains from : - intense pain - swelling around the wound - brownish discharge - gas formation - little or no pyrexia - characteristic smelling - toxaemic coma death • the prime site for infection is a dirty wound with dead muscle that has been closed without adequate debridement • •

• Gas gangrene ---characterized by myonecrosis • Anaerobic cellulitis in which superficial gas formation is abundant but toxaemia usually is slight. • Failure to recognize the difference may lead to unnecessary amputation for the non-lethal cellulitis

swelling around the wound, brownish discharge gas formation

Prevention Deep, penetrating wounds in muscular tissue are dangerous; they should be explored, all dead tissue should be completely excised and, if there is the slightest doubt about tissue viability, the wound should be left open. There is no effective antitoxin against C. welchii. Treatment -early diagnosis. -fluid replacement -intravenous antibiotics -Hyperbaric oxygen has been used for limiting the spread of gangrene. -mainstay of treatment is prompt decompression of the wound and removal of all dead tissue. In advanced cases, amputation may be essential

FRACTURE BLISTERS • Two distinct blister types are seen after fractures: clear fluid-filled vesicles and blood-stained ones. • Both occur during limb swelling and are due to elevation of the epidermal layer of skin from the dermis. • There is no advantage to puncturing the blisters (it may even lead to increased local infection) and surgical incisions through blisters, whilst generally safe, should be undertaken only when limb swelling has decreased

PLASTER AND PRESSURE SORES • Plaster sores occur where skin presses directly onto bone. • They should be prevented by padding the bony points and by moulding the wet plaster so that pressure is distributed to the soft tissues around the bony points. • While a plaster sore is developing the patient feels localized burning pain. A window must immediately be cut in the plaster, or warning pain quickly abates and skin necrosis proceeds unnoticed. • careless selection of ring size, excessive fixed traction, and neglect can lead to pressure sores around the groin and iliac crest

Late complications • 1 -DELAYED UNION • 2 -NON-UNION • 3 -MALUNION • 4 -AVASCULAR NECROSIS • 5 -GROWTH DISTURBANCE • 6 -BED SORES • 7 -MYOSITIS OSSIFICANS • 8 -TENDON LESIONS • 9 -NERVE COMPRESSION • 10 -MUSCLE CONTRACTURE • 11 -JOINT INSTABILITY • 12 -JOINT STIFFNESS • 13 -COMPLEX REGIONAL PAIN SYNDROME (ALGODYSTROPHY) • 14 -OSTEOARTHRITIS

DELAYED UNION • If the time in which a fracture may be expected to unite and consolidate is prolonged, the term ‘ delayed union ’ is used. It must never be relied upon in deciding when treatment may be discontinued. • As a general rule , union is deemed to be delayed if the fracture is still freely mobile after 3 or 4 months. If a state of delayed union persists for many months it will eventually pass into a state of non-union • Causes can be summarized as : 1 - biological 2 - biomechanical 3 - patient-related

1 - Biological cause : A- Inadequate blood supply A badly displaced fracture of along bone will cause tearing of both the periosteum and interruption of the intramedullary blood supply. The fracture edges will become necrotic and dependent on the formation of an ensheathing callus mass to bridge the break. If the zone of necrosis is extensive, as might occur in highly comminuted fractures, union may be interrupted. B- Severe soft tissue damage Severe damage to the soft tissues affects fracture healing by: (1) reducing the effectiveness of muscle splintage ; (2) damaging the local blood supply and (3) diminishing or eliminating the osteogenic input from mesenchymal stem cells within muscle. • C- Periosteal stripping over-enthusiastic stripping of periosteum during internal fixation is an avoidable cause of delayed union.
")
2 - Biomechanical cause : A- Imperfect splintage. Excessive traction (creating a fracture gap) or excessive movement at the fracture site will delay ossification in the callus. In the forearm and leg a single-bone fracture may be held apart by an intact fellow bone. B- Over-rigid fixation. Contrary to popular belief, rigid fixation delays rather than promotes fracture union. It is only because the fixation device holds the fragments so securely that the fracture seems to be ‘uniting’. Union by primary bone healing is slow, but provided stability is maintained throughout, it does eventually occur. C- Infection. Both biology and stability are affected by active infection: not only is there bone lysis, necrosis and pus formation, but implants which are used to hold the fracture tend to loosen.

3 - Patient related : There are patients who are : • Immovable. • Impossible. • Age. • Associated systemic illness. • Smoking.

• Clinical features : • Fracture tenderness persists and, if the bone is subjected to stress, pain may be acute. • On x-ray, the fracture line remains visible and there is very little or incomplete callus formation or periosteal reaction. However, the bone ends are not sclerosed nor atrophic. The appearances suggest that , although the fracture has not united, it eventually will.

• Treatment : • CONSERVATIVE or OPERATIVE 1 - conservative : • The two important principles are: (1) to eliminate any possible cause of delayed union and (2) to promote healing by providing the most appropriate environment. Immobilization (whether by cast or by internal fixation) should be sufficient to prevent shear at the fracture site, but fracture loading is an important stimulus to union and can be enhanced by: (1) encouraging muscular exercise and (2) by weightbearing in the cast or brace ? . The watchword is patience; however , there comes a point with every fracture where the illeffects of prolonged immobilization outweigh the advantages of nonoperative treatment.

2 - Operative : • each case should be treated on its merits; however, if union is delayed for more than 6 months and there is no sign of callus formation, internal fixation and bone grafting are indicated. The operation should be planned in such a way as to cause the least possible damage to the soft tissues.

NON-UNION • In a minority of cases delayed union gradually turns into non-union that is it becomes apparent that the fracture will never unite without intervention. • Causes: • When dealing with the problem of non-union, four questions must be addressed. They have given rise to the acronym CASS: • 1. Contact– Was there sufficient contact between the fragments? • 2. Alignment – Was the fracture adequately aligned , to reduce shear? • 3. Stability – Was the fracture held with sufficient stability? • 4. Stimulation – Was the fracture sufficiently ‘stimulated’? (e. g. by encouraging weightbearing).

• There are, of course, also biological and patient-related reasons that may lead to non-union: • (1) distraction and separation of the fragments, sometimes the result of interposition of soft tissues between the fragments (there is muscle or ligament covering the broken ends and preventing them from touching each other) • (2) excessive movement at the fracture line (the two ends are still mobile ). • (3) poor soft tissues (from either the injury or surgery). • (4) poor local blood supply ( avascular necrosis ). • (5) infection (particularly osteomyelitis ). • (6) associated drug abuse, anti-inflammatory or cytotoxic immunosuppressant medication. • (7) non-compliance on the part of the patient. • (8) surgical intervention, If fill-judged, is another cause.

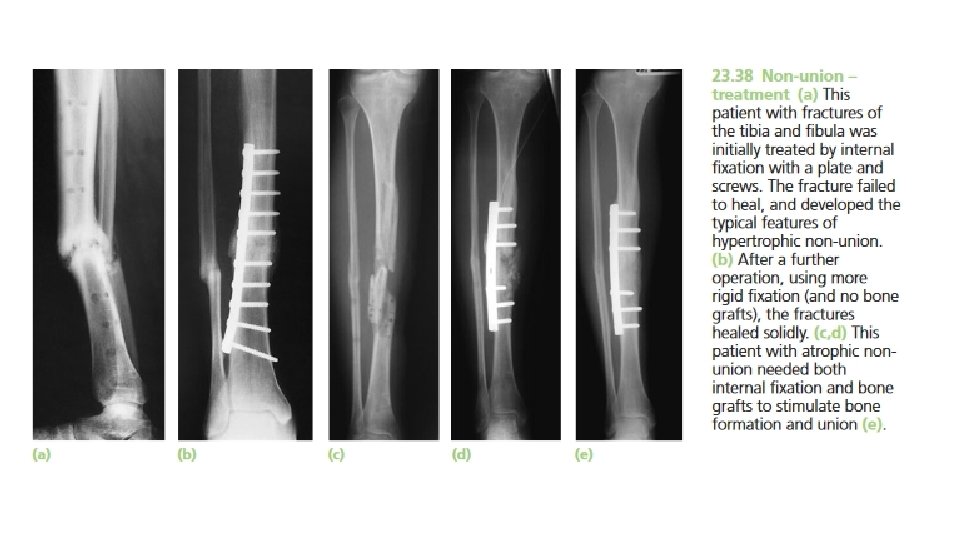
• Clinical features : • Movement can be elicited at the fracture site and pain diminishes ; the fracture gap ( cavity between the bone ends ) becomes a type of pseudoarthrosis. • X-ray The fracture is clearly visible but the bone on either side of it may show either exuberant callus or atrophy. This contrasting appearance has led to non-union being divided into hypertrophic and atrophic types. In hypertrophic non-union the bone ends are enlarged, suggesting that osteogenesis is still active but not quite capable of bridging the gap. In atrophic non-union, osteogenesis seems to have ceased. The bone ends are rounded with no suggestion of new bone formation.


• Treatment : • CONSERVATIVE or OPERATIVE 1 - Conservative : • Non-union is occasionally symptomless, needing no treatment as it might cause slight instability and is best left untreated , or at most, (a) a removable splint. Even if symptoms are present, operation is not the only answer; with hypertrophic non-union, (b) functional bracing may be sufficient to induce union, but splintage often needs to be prolonged. (c) Pulsed electromagnetic fields and low-frequency, pulsed ultrasound can also be used to stimulate union. • 2 - Operative : • More often , non-union of a fracture is disabling and surgical treatment is desirable , With hypertrophic non-union and in the absence of deformity, very rigid fixation alone (internal or external) may lead to union. With atrophic non-union, fixation alone is not enough. Fibrous tissue in the fracture gap, as well as the hard, sclerotic bone ends is excised and bone grafts are packed around the fracture. If there is significant ‘die-back’, this will require more extensive excision and the gap is then dealt with by bone advancement using the Ilizarov technique.

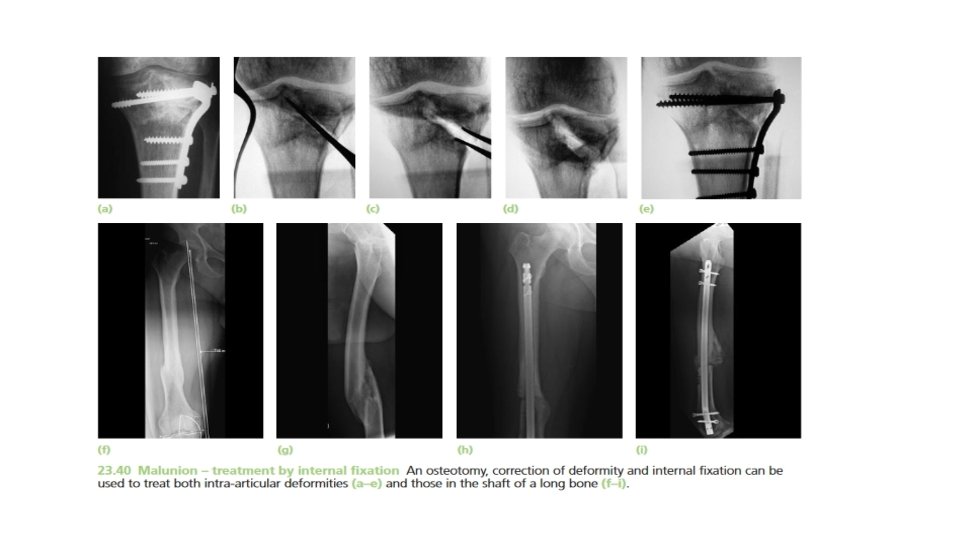
MALUNION • When the fragments join in an unsatisfactory position (unacceptable angulation, rotation or shortening) the fracture is said to be malunited. • Causes are • (a) failure to reduce a fracture adequately. • (b) failure to hold reduction while healing proceeds. • (c) gradual collapse of comminuted bone. • (d) osteoporotic bone.

• Clinical features : • The deformity is usually obvious, but sometimes the true extent of malunion is apparent only on x-ray. Rotational deformity of the femur, tibia, humerus or forearm may be missed unless the limb is compared with its opposite fellow. Rotational deformity of a metacarpal fracture is detected by asking the patient to flatten the fingers onto the palm and seeing whether the normal regular fanshaped appearance is reproduced. • X-rays are essential to check the position of the fracture while it is uniting. This is particularly important during the first 3 weeks, when the situation may change without warning. At this stage it is sometimes difficult to decide what constitutes ‘malunion’ ; acceptable norms differ from one site to another.

• Treatment : • Incipient malunion may call for treatment even before the fracture has fully united; the decision on the need for re-manipulation or correction may be extremely difficult. A few guidelines are offered: • 1. In adults, fractures should be reduced as near to the anatomical position as possible. Angulation of more than 10– 15 degrees in a long bone or a noticeable rotational deformity may need correction by remanipulation, or by osteotomy and fixation. • 2. In children, angular deformities near the bone ends (and especially if the deformity is in the same plane as that of movement of the nearby joint) will usually remodel with time; rotational deformities will not.

• 3. In the lower limb, shortening of more than 2. 0 cm is seldom acceptable to the patient and a limb length equalizing procedure may be indicated. • * The patient’s expectations (often prompted by cosmesis) may be quite different from the surgeon’s; they are not to be ignored. • - Early discussion with the patient, and a guided view of the x-rays, will help in deciding the need for treatment and may prevent later misunderstanding. • - Very little is known of the long-term effects of small angular deformities on joint function. However, it seems likely that malalignment of more than 15 degrees in any plane may cause asymmetrical loading of the joint above or below and the late development of secondary osteoarthritis; this applies particularly to the large weightbearing joints.

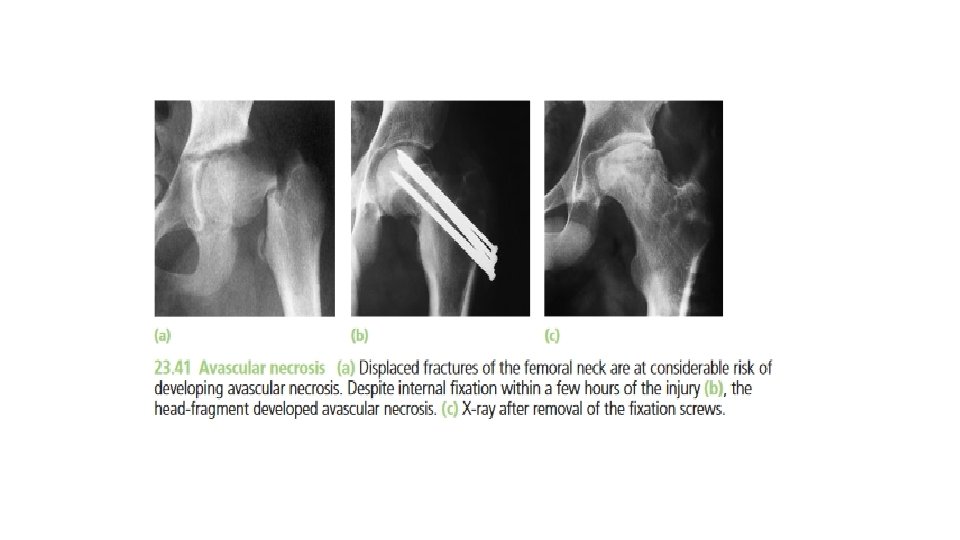
AVASCULAR NECROSIS • Death of a bone from a deficient blood supply. • Certain regions are known for their propensity to develop ischaemia and bone necrosis after injury. They are: • (1) the head of the femur (after fracture of the femoral neck or dislocation of the hip) • (2) the proximal part of the scaphoid (after fracture through its waist); • (3) the lunate (following dislocation) • (4) the body of the talus (after fracture of its neck). • Accurately speaking, this is an early complication of bone injury, because ischaemia occurs during the first few hours following fracture or dislocation. However , the clinical and radiological effects are not seen until weeks or even months later , the avascular bone gradually loses its rigid trabecular structure , in this state the bone crumbles easily and under stress imposed by the muscular tone or body weight it will eventually collapse which may be sometimes very slow.

• Clinical features : • Avascular necrosis causes : intractable non union , disabling osteoarthritis or total disorganization of a joint. • There are no symptoms associated with avascular necrosis, but if the fracture fails to unite or if the bone collapses the patient may complain of pain. • X-ray shows the characteristic increase in x-ray density , which occurs as a consequence of two factors: (a) disuse osteoporosis in the surrounding parts gives the impression of ‘increased density’ in the necrotic segment, and (b) collapse of trabeculae compacts the bone and increases its density. Where normal bone meets the necrotic segment a zone of increased radiographic density may be produced by new bone formation.

• Treatment : • Treatment usually becomes necessary when joint function is threatened. In old people with necrosis of the femoral head an arthroplasty (reconstruction or replacement of a joint ) is the obvious choice; in younger people, realignment osteotomy (or, in some cases, arthrodesis (immobilization of a joint by fusion of the bones) ) may be wiser. Avascular necrosis in the scaphoid or talus may need no more than symptomatic treatment, but arthrodesis of the wrist or ankle is sometimes needed.
 may")
GROWTH DISTURBANCE • In children, damage to the physis ( growth plate ) may lead to abnormal or arrested growth , over 10 per cent of fractures involve injury to the growth plate (or physis). Because the physis is a relatively weak part of the bone. • Mechanism of injury: • Physeal fractures usually result from falls or traction injuries. They occur mostly in road accidents and during sporting activities or playground tumbles.

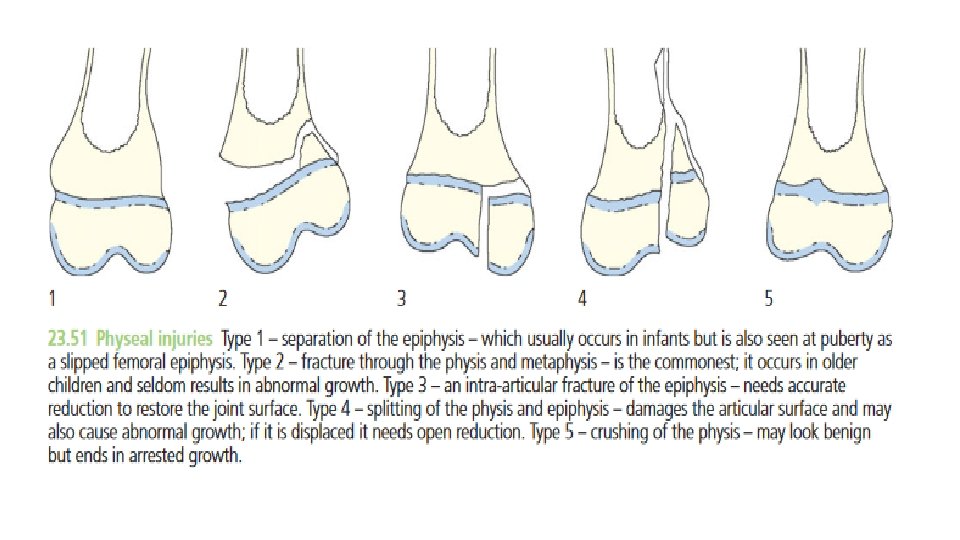
• Classification: • The most widely used classification of physeal injuries is that of Salter and Harris (Salter and Harris, 1963), which distinguishes five basic types of injury: • • Type 1 – A transverse fracture through the hypertrophic or calcified zone of the plate. Even if the fracture is quite alarmingly displaced, the growing zone of the physis is usually not injured and growth disturbance is uncommon. • • Type 2– This is essentially similar to type 1, but towards the edge the fracture deviates away from the physis and splits off a triangular metaphyseal fragment of bone (sometimes referred to as the Thurston–Holland fragment).

• • Type 3 – A fracture that splits the epiphysis and then swerves off transversely to one or the other side , through the hypertrophic layer of the physis. Inevitably it damages the ‘reproductive’ layers of the physis (as these layers are closer to the epiphysis than the metaphysis) and may result in growth disturbance. • • Type 4 – As with type 3, the fracture splits the epiphysis, but it extends into the metaphysis. These fractures are liable to displacement and a consequent misfit between the separated parts of the physis, resulting in asymmetrical growth. • • Type 5– A longitudinal compression injury of the physis. There is no visible fracture but the growth plate is crushed and this may result in growth arrest.
 has added a Type 6, an injury to the")
• Rang (Rang, 1969) has added a Type 6, an injury to the perichondrial ring (the peripheral zone of Ranvier), which carries a significant risk of growth disturbance. The diagnosis is made usually in retrospect after development of deformity.

• Clinical features : • These fractures are more common in boys than in girls and are usually seen either in infancy or between the ages of 10 and 12. Deformity is usually minimal, but any injury in a child followed by pain and tenderness near the joint should arouse suspicion, and x-ray examination is essential. • X-rays : • The physis itself is radiolucent and the epiphysis maybe incompletely ossified; this makes it hard to tell whether the bone end is damaged or deformed. The younger the child, the smaller the ‘visible’ part of the epiphysis and thus the more difficult it is to make the diagnosis; comparison with the normal side is a great help. Telltale features are widening of the physeal ‘gap’, tilting of the epiphyseal axis. If there is marked displacement the diagnosis is obvious, but even a type 4 fracture may at first be so little displaced that the fracture line is hard to see; if there is the low suspicion of a physeal fracture, a repeat x-ray after 4 or 5 days is essential. Types 5 and 6 injuries are usually diagnosed only in retrospect.
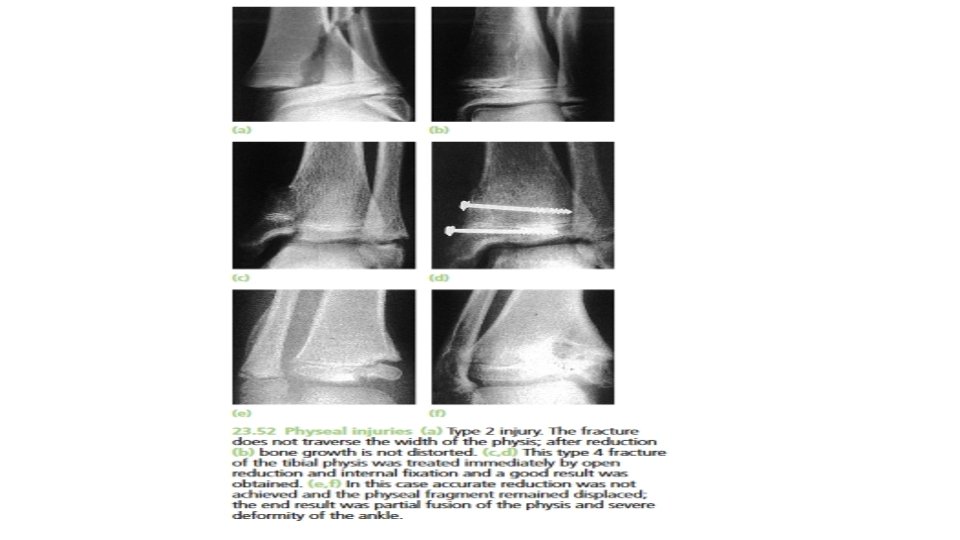

• Treatment : • Undisplaced fractures may be treated by splinting the part in a cast or a close-fitting plaster slab for 2– 4 weeks (depending on the site of injury and the age of the child). However, with undisplaced types 3 and 4 fractures, a check x-ray after 4 days and again at about 10 days is mandatory in order not to miss late displacement. • Displaced fractures should be reduced as soon as possible. With types 1 and 2 this can usually be done closed; the part is then splinted securely for 3– 6 weeks. Types 3 and 4 fractures demand perfect anatomical reduction. An attempt can be made to achieve this by gentle manipulation under general anaesthesia; if this is successful, the limb is held in a cast for 4– 8 weeks (the longer periods for type 4 injuries). If a type 3 or 4 fracture cannot be reduced accurately by closed manipulation, immediate open reduction and internal fixation with smooth K-wires is essential. The limb is then splinted for 4– 6 weeks, but it takes that long again before the child is ready to resume unrestricted activities.

• Complications : • Types 1 and 2 injuries, if properly reduced, have an excellent prognosis and bone growth is not adversely affected. Exceptions to this rule are injuries around the knee involving the distal femoral or proximal tibial physis; both growth plates are undulating in shape , so a transverse fracture plane may actually pass through more than just the hypertrophic zone but also damage the proliferative zone. Complications such as malunion or non-union may also occur if the diagnosis is missed and the fracture remains unreduced • Types 3 and 4 injuries may result in premature fusion of part of the growth plate or asymmetrical growth of the bone end.

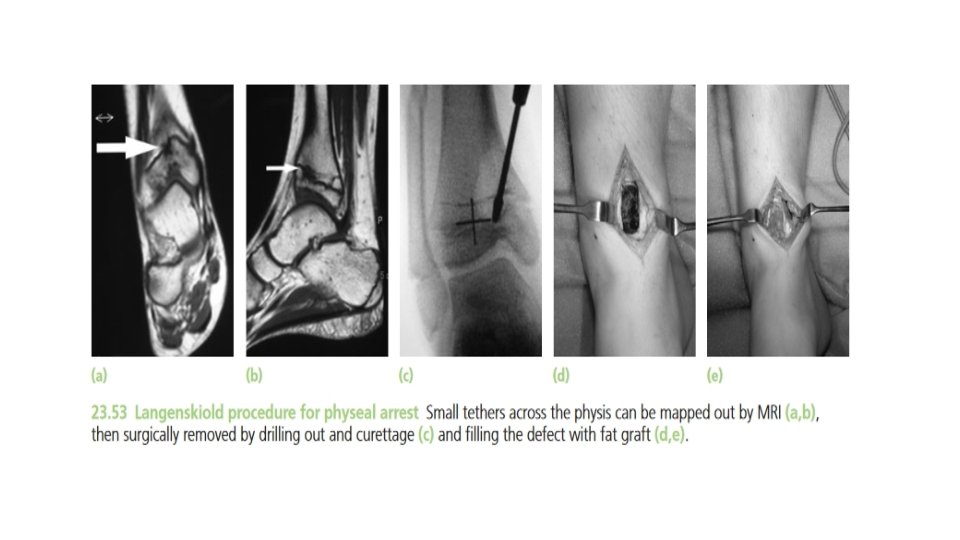
• Types 5 and 6 fractures cause premature fusion and retardation of growth. The size and position of the bony bridge across the physis can be assessed by tomography or magnetic resonance imaging (MRI). If the bridge is relatively small (less than one-third the width of the physis) it can be excised and replaced by a fat graft, with some prospect of preventing or diminishing the growth disturbance. However, if the bone bridge is more extensive the operation is contraindicated as it can end up doing more harm than good. Established deformity, whether from asymmetrical growth or from malunion of a displaced fracture should be treated by corrective osteotomy. If further growth is abnormal , the osteotomy may have to be repeated.
 • are injuries to skin and underlying tissue resulting from")
BED SORES (pressure ulcers) • are injuries to skin and underlying tissue resulting from prolonged pressure on the skin. Bedsores most often develop on skin that covers bony areas of the body (Sacrum, heels, elbow , shoulder and head). • Bed sores occur in elderly or paralyzed patients. • once they have developed, treatment is difficult. • Clean the wound , Apply dressings, use antibiotic. • it may be necessary to excise the necrotic tissue and apply skin grafts.
 • Heterotopic ossification in the muscles. • In cases of")
MYOSITIS OSSIFICANS (post-traumatic ossification) • Heterotopic ossification in the muscles. • In cases of severe injury to a joint, and especially when the capsule and periosteum have been stripped from the bones and blood collects under the stripped soft tissue forming a hematoma and then invaded by osteoblasts. • Pain, Tenderness , Focal swelling, and Joint/muscle contractions.

• X-ray is normal but a bone scan may show increased activity. • Over the next 2– 3 weeks the pain gradually subsides, but joint movement is limited; x-ray may show fluffy calcification in the soft tissues. • By 8 weeks the bony mass is easily palpable and is clearly defined in the xray. • In early stages of treatment rest is advised and NSAIDS may help to reduce pain and rest for 3 -4 weeks avoid muscle-stretching activity because might provoke further bleeding beneath the soft tissues. • later Physiotherapy is prescribed to regain movements. • Months later, Ultra sound In some cases and surgical excision of myositic mass is done and radiotherapy to prevent recurrence.

TENDON LESIONS • Tendinitis and tendon rupture. • Pain on moving, tender, swelling, difficulty in move the area. • resting or elevating the tendon, medications, wrapping the area and doing stretches and exercises.

• It should be prevented by reduction. • Rupture of the extensor pollicis longus tendon may occur 6– 12 weeks after a fracture of the lower radius. • Direct suture is seldom possible and the resulting disability is treated by transferring the extensor indicis tendon to the distal stump of the ruptured thumb tendon
 • pain, tingling, numbness, reduced flexibility, muscle weakness and difficulty")
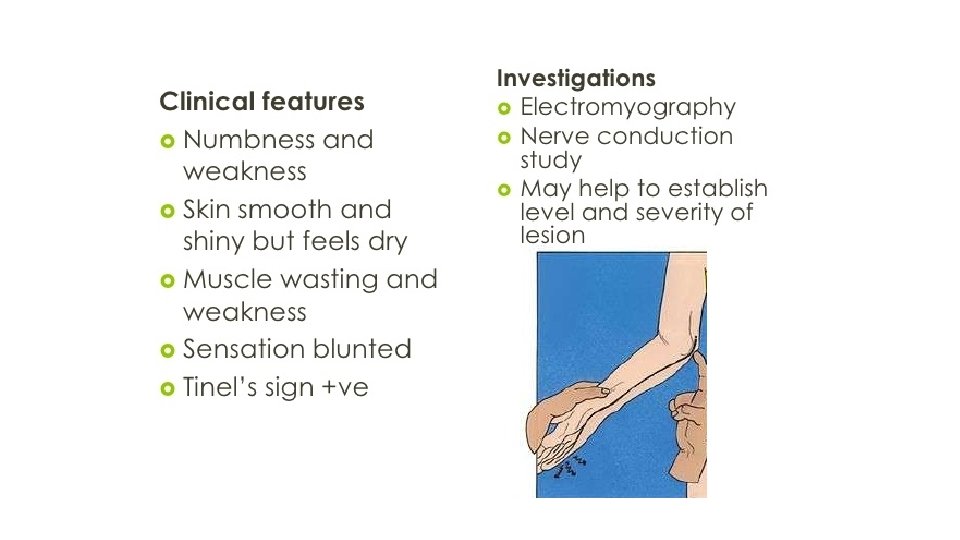
NERVE COMPRESSION (entrapment neuropathy) • pain, tingling, numbness, reduced flexibility, muscle weakness and difficulty with certain movements. • The symptoms affect just one particular part of the body, depending on which nerve is affected. • Surgery (early decompression of the nerve) , Physical therapy and NSAIDs.
 the ulnar nerve, due to elbow injury. • (2)")
Common sites are: • (1) the ulnar nerve, due to elbow injury. • (2) the median nerve, following injuries around the wrist. • (3) the posterior tibial nerve, following fractures around the ankle.
 • Following arterial injury or compartment syndrome. • The")
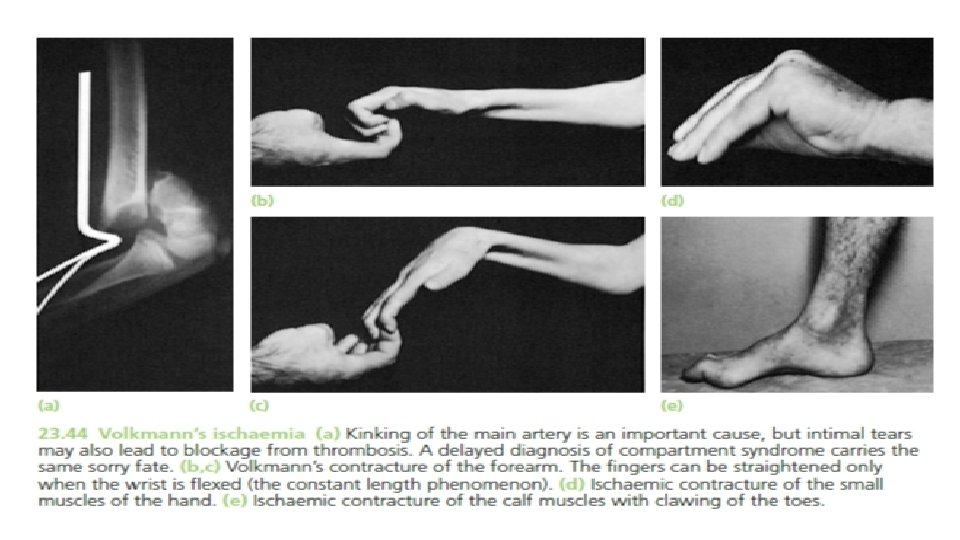
MUSCLE CONTRACTURE (Volkmann’s ischemic contracture) • Following arterial injury or compartment syndrome. • The ischemic muscles are replaced by fibrous tissue. • If the peripheral nerves are also affected, sensory or motor paralysis may happen. • Clinical features: Marked atrophy, Flexion deformity, Nails shows atrophic changes and Skin becomes dry and scaly.

• Treatment: Detachment of the flexor muscles at their origin and along the interosseous membrane in the forearm may improve the deformity, but function is no better if sensation and active movement are not restored. • Nerve grafts may provide protective sensation in the hand, and tendon transfers (wrist extensors to finger and thumb flexors) will allow active grasp. In less severe cases, median nerve sensibility may be quite good and, with appropriate tendon releases and transfers, the patient regains a considerable degree of function.
. 2 -Muscle weakness. 3 -Bone loss.")
JOINT INSTABILITY • Causes: 1 -Ligamentous laxity (hypermobility). 2 -Muscle weakness. 3 -Bone loss. Injury may also lead to recurrent dislocation. The commonest sites are: (1) the shoulder (2) the patella
 small")
JOINT STIFFNESS • occurs in the knee, elbow, shoulder and (worst of all) small joints of the hand. • the joint itself has been injured; a haemarthrosis forms and leads to synovial adhesions. More often the stiffness is due to oedema and fibrosis of the capsule, ligaments and muscles around the joint, or adhesions of the soft tissues to each other or to the underlying bone. These patients are at great risk of developing a complex regional pain syndrome.

• Worsen by prolong immobilization. • The best treatment is prevention – by exercises that keep the joints mobile from the outset and physiotherapy. • Occasionally, adherent or contracted tissues need to be released by operation.
 • painful osteoporosis of the hand, and stiffness. •")
COMPLEX REGIONAL PAIN SYNDROME (ALGODYSTROPHY) • painful osteoporosis of the hand, and stiffness. • for many years it was called Sudeck’s atrophy. • The cause and exact nature of the condition are unknown, but it probably results from a disturbance of centrally mediated autonomie regulation with consequent increased stimulation of sympathetic and motor efferent fibres.

2 months after the injury the symptoms start, At first there is local swelling, redness and warmth, as well as tenderness and moderate stiffness of the nearby joints. As the weeks go by the skin becomes pale and atrophic with hair loss, movements are increasingly restricted and the patient may develop fixed deformities. X-rays characteristically show patchy rarefaction of the bone.

, this type")
• Type 1. Also known as reflex sympathetic dystrophy syndrome (RSD), this type occurs after an illness or injury that didn't directly damage the nerves in your affected limb. About 90 percent of people with complex regional pain syndrome have type 1. • Type 2. Once referred to as causalgia, this type has similar symptoms to type 1, But type 2 complex regional pain syndrome follows a distinct nerve injury. • Elevation and active exercises are important. • anti-inflammatory drugs and adequate analgesia are helpful with prolonged and dedicated physiotherapy, is the mainstay of treatment. • Guanethidine to produce regional sympathetic blockade.
 • A fracture involving a joint may severely damage the articular")
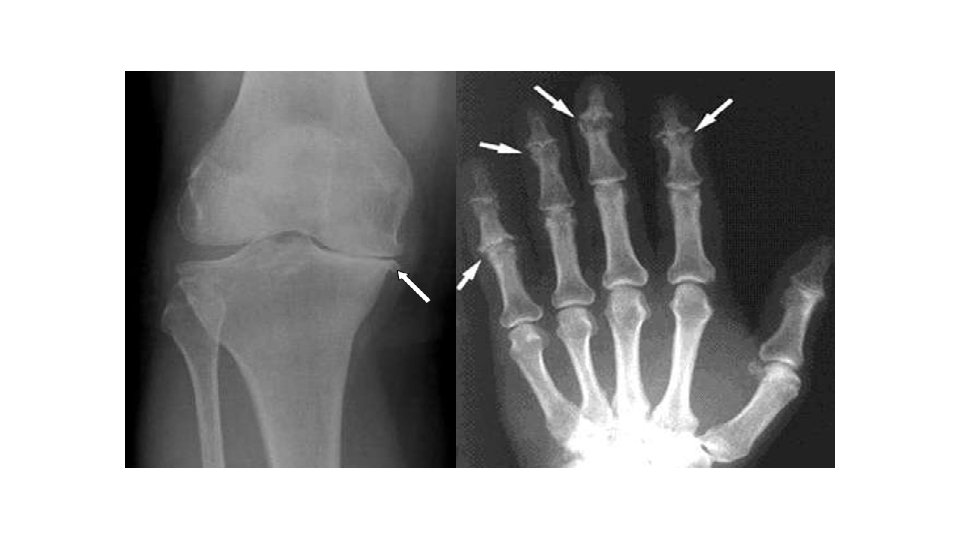
OSTEOARTHRITIS (degenerative arthritis) • A fracture involving a joint may severely damage the articular cartilage and accelerate tear and wear change that give rise to posttraumatic osteoarthritis within a period of 6 -9 months. • Even if the cartilage heals, irregularity of the joint surface may cause localized stress and so predispose to secondary osteoarthritis years later.

• greater risk in the weight bearing joints • Osteoarthritis cannot be cured, but it can be treated • The goal of every treatment for arthritis is to: 1. reduce pain and stiffness, 2. allow for greater movement, and 3. slow the progression of the disease • Anti-Inflammatory Medication
- Slides: 83