Complications of Extraction of Impacted Teeth Outline I



























 -Atrumatic surgical extraction (clean incisions, gentle management of")



 Cause -Lysis of a fully formed blood clot before")

- Slides: 38
Complications of Extraction of Impacted Teeth
Outline I. Soft Tissue Injuries II. Complications with the Tooth Being Extracted III. Injuries to Adjacent Teeth IV. Injuries to Osseous Structures V. Injuries To Adjacent Structures VI. Oroantral Communications VII. Postoperative Bleeding VIII. Delayed Healing & Infection
I. Soft Tissue Injuries
1. Tearing Mucosal Flap Causes Due to an inadequately sized flap which is retracted beyond the tissue`s ability to stretch. As with a short envelope flap when the area of surgery is at the apex.
Prevention -Adequately sized flaps -Gentle Retraction Management Reposition the flap & suture If the tear is jagged, trim it before suturing
2. Puncture Wound of Soft Tissue Cause Instrument Slippage Prevention Controlled force Management Suturing to prevent infection & allow healing to occur
3. Stretch or Abrasion Injury Cause Bur shank or retractor injury Prevention Care Management Keep it moist ( ointment ) Heals within 5 – 10 days
II. Complications with the tooth Being Extracted
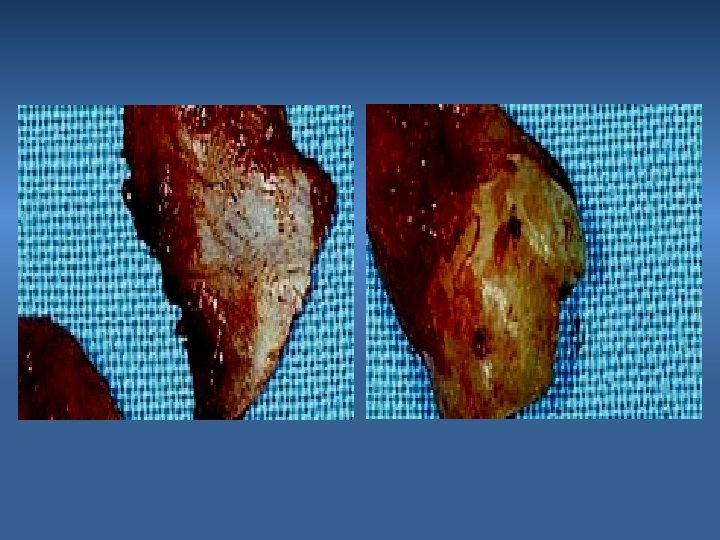
1. Root Fracture Cause Long, curved, divergent roots Excessive force during extraction Prevention Proper exposure & bone removal
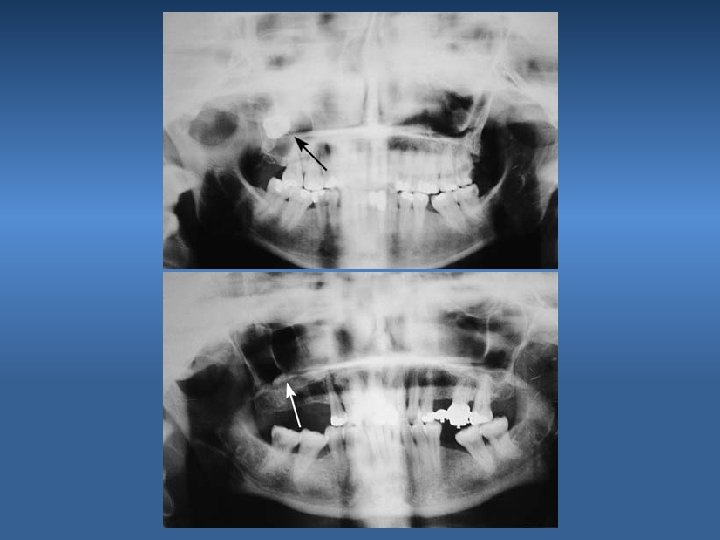
2. Root Displacement Into: • Mandibular Canal • Lingual Pouch • Infratemporal Space • Maxillary Sinus
III. Injuries to Adjacent Teeth 1. Luxation of Adjacent Teeth 2. Fracture of Adjacent Restoration Cause Carelesness Prevention Judicious use of elevators
IV. Injuries to Osseous Structures
1. Fracture of Alveolar Process Fracture of the Buccal or Lingual Cortex Cause Inadequate exposure & excessive force Prevention Adequate bone removal & eposure
2. Fracture of Maxillary Tuberosity Cause Excessive force Prevention Proper support and controlled force Management If still attached; dissect and remove the tooth If detached; smooth bone edges & suture
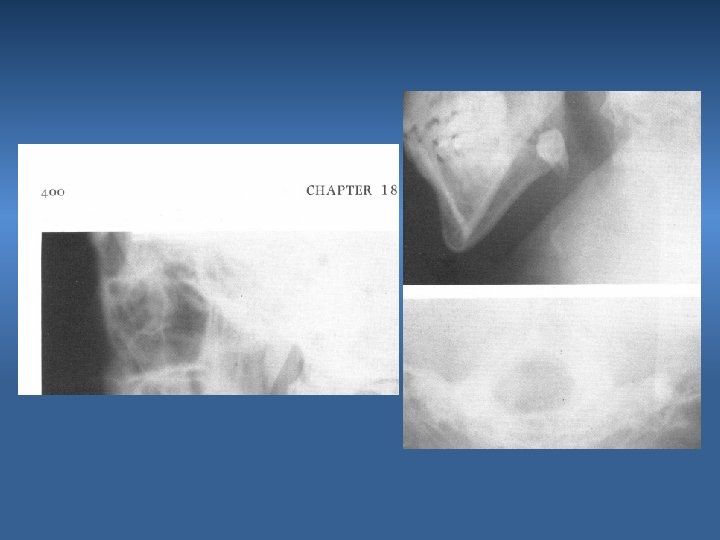
3. Fracture of the Mandible Cause Excessive force Prevention Proper bone removal & controlled force
Photoelastic model of the mandible, showing the development of stress during a luxation attempt of the third molar when insufficient bone has been removed from the tooth peripherally
V. Injuries to Adjacent Structures
1. Injury to Inferior Alveolar Nerve Cause -Excessive extraction force in case of curved roots -Sectioning the tooth all the way inferiorly Prevention -Proper exposure & bone removal -Controlled force -Careful setioning, leaving a shell of the tooth
2. Injury to the Lingual Nerve Cause -Placement of the retromolar incision far lingually -Sectioning the tooth all the way to the lingual cortex Prevention -Proper incision -Careful sectioning, leaving a shell of the tooth
3. Injury to the TMJ Cause Inadequate support of the mandible during extraction Prevention Use of bite block Management Reduction
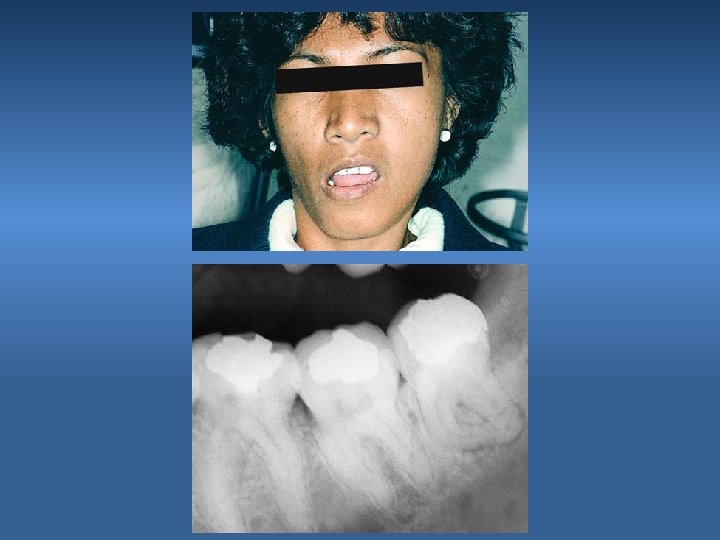
Vi. Oroantral Communication Cause During extraction of an impacted maxillary canine -Excessive bone removal -Failure to locate the tooth Prevention -Proper preoperative radiographic evaluation -Proper bone removal -Controlled force
VII. Postoperative Bleeding Cause -Bleeding at wound margins -Bleeding at a bony foramen within the socket -Medical Problem
Prevention -Good history taking (coagulopathy, medications…etc) -Atrumatic surgical extraction (clean incisions, gentle management of soft tissues, smoothen bony specules, curette granulation tissue) -Obtain good homeostasis at surgery - Postoperative instructions
Management Local Measures • Pressure packs • Suturing • Ligate bleeding vessels • Burnish bone • Apply material to aid in hemostasis (surgicell, collaplug)
VIII. Delayed Healing & Infection
1. Infection Cause Debris left under the flap Prevention Irrigation Management Debridement & Drainage
2. Dry Socket (Alveolar Ostitis) Cause -Lysis of a fully formed blood clot before the clot is replaced with granulation tissue. -Higher incidence with smokers & patients taking oral contaceptives. Prevention -Presurgical irrigation with antimicrobial agents , e. g: chlorhexidine -Intraoperative irrigation with saline
Management – Irrigate with warm saline – Remove old clots – Place sedative dressing – Prescribe mild analgesics – Reassess after 24 to 48 hours