Complications of diabetes Mohsen Eledrisi MD FACE FACP

Complications of diabetes Mohsen Eledrisi, MD, FACE, FACP Department of Medicine Hamad Medical Corporation Doha, Qatar www. eledrisi. com

Session objectives • Describe the various complications of diabetes • Discuss the classification & management of diabetic neuropathy • Elaborate on the detection & management of albuminuria • Discuss the benefits of glucose control on the risk of complications of diabetes
")
Complications of diabetes Macrovascular “Macro” = large Disease of the large vessels (Cardiovascular disease) Microvascular “Micro” = smal Disease of the small vessels

Complications of diabetes Stroke Eye disease Heart disease Kidney disease Peripheral arterial disease Nerve disease

Microvascular complications of DM Eye Kidney Nerves Retinopathy Cataract Glaucoma Nephropathy Neuropathy - Albuminuira - Peripheral Blindness Chronic kidney disease - Autonomic Disability/Death Amputation Quality of life
 •")
Diabetic neuropathy: the facts • Most common complication of DM (~ 50 %) • At diagnosis of diabetes, 30 % already have neuropathy • 15 % of all patients will have an ulcer in their life • Diabetes accounts for 75 % of non-traumatic amputations • 1500 % risk of amputations compared with non-diabetics • Up to 50 % of peripheral neuropathies are asymptomatic ADA statement. Diabetes Care 2017; 4: 136
 Diffuse neuropathy A) Distal symmetric polyneuropathy (DSPN): most common")
Classification of diabetic neuropathies 1) Diffuse neuropathy A) Distal symmetric polyneuropathy (DSPN): most common B) Autonomic: cardiovascular, gastrointestinal, urogenital, sudomotor dysfunction, hypoglycemia unawareness, abnormal pupillary function 2) Mononeuropathy: Isolated cranial or peripheral nerve (e. g. , CN III, ulnar, median, femoral, peroneal), mononeuritis multiplex 3) Radiculopathy or polyradiculopathy : Lumbosacral polyradiculopathy, proximal motor amyotrophy, thoracic radiculopathy ADA statement. Diabetes Care 2017; 4: 136
 Cardiovascular: Reduced heart rate variability, Resting tachycardia, Orthostatic hypotension,")
Autonomic neuropathies in diabetes 1) Cardiovascular: Reduced heart rate variability, Resting tachycardia, Orthostatic hypotension, Sudden death (malignant arrhythmia) 2) Gastrointestinal: Diabetic gastroparesis (gastropathy), Diabetic enteropathy, (diarrhea), Colonic hypomotility (constipation) 3) Urogenital: Diabetic cystopathy (neurogenic bladder), Erectile dysfunction, Female sexual dysfunction 4) Sudomotor dysfunction Distal hypohydrosis/anhidrosis, , Gustatory sweating 5) Hypoglycemia unawareness 6) Abnormal pupillary function

Pain distribution in diabetic neuropathies

Complications of DSPN • Wounds/Ulcers • Infections • Charcot arthropathy • Dislocation and stress fractures • Amputation

Differential diagnosis of diabetic neuropathies • Hypothyroidism • Nutritional deficiency (vitamin B 12, thiamine, pyridoxine, postgastroplasty) • Chronic kidney disease • Medications: hydralazine, amiodarone, isoniazid, phenytoin, metronidazole, colchicine • Alcohol • Vasculitis, paraproteinemia, amyloidosis • Infections: HIV, hepatitis B, Lyme disease
 - History & comprehensive foot exam: • Type")
Screening for diabetic neuropathy (distal symmetric) - History & comprehensive foot exam: • Type 2 DM : At the time of diagnosis then every year • Type 1 DM : Start 5 years after diagnosis then every year - Inspect feet each visit for high risk American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151

Diabetic neuropathy: the history • Up to 50% of patients may experience symptoms of DSPN • The most common early symptoms are pain and dysesthesias (unpleasant sensations of burning) • Pain is usually burning, lancinating, tingling, or shooting (electric shock-like) & worse at night • May be accompanied by an exaggerated response to painful stimuli (hyperalgesia) and pain evoked by contact with socks, shoes, bedclothes (allodynia).

Foot examination - Inspect the feet: Integrity of the skin Deformities Callus Wounds/ulcers Infections (tinea)

Foot care • Comprehensive exam yearly • Self-care education • Visual inspection (every visit for high risk patients) • Vibration, temperature, or pinprick sensation • 10 -gram monofilament test • Assess pedal pulses (refer for Ankle-brachial index if ↓) American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151

10 -gram monofilament test Patient closes eyes Apply pressure at 90 enough to bend for 2 seconds Avoid ulcer/callus areas ≥ 8 points of 10 = Normal
 Compare to")
Testing for vibration sensation Use 128 Hz tuning fork 2 techniques 1) Compare to examiner (mostly used) 2) Compare patient’s big toe to his wrist

Vibration test - Compare patient’s big toe to his wrist - Does it feel the same? - While feeling on wrist, move to big toe. Can the patient still feel?

Testing vibration sensation

Testing vibration Explain what you are doing to the patient Put vibrating fork first on wrist or sternum; patient to close eyes; does he feel vibrations? If yes, proceed Close eyes. Put fork on bony part of big toe Examiner to put index finger below big toe Patient to tell you once he cannot feel vibrations any more If examiner can still feel vibrations, that is abnormal

Management of DSPN Glucose control Lifestyle changes Foot care Pain control ADA statement. Diabetes Care 2017; 4: 136
 Gabapentin can be")
Drug therapy for neuropathic pain Pregabalin or Duloxetine (evidence level A) Gabapentin can be also considered (evidence level B) 2 nd line: Tricyclic antidepressants, venlafaxine, carbamazepine, topical capsaicin Opioids are not recommended as 1 st or 2 nd line American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151
 Also an antidepressant Starting dose: 30 mg qd Usual effective")
Duloxetine ® (Cymbalta ) Also an antidepressant Starting dose: 30 mg qd Usual effective dose: 60 -120 mg qd Dizziness, nausea, headache, insomnia, somnolence Expensive ADA statement. Diabetes Care 2017; 4: 136 Bril V, et al. Neurology 2011; 76: 1758.
 Pregabalin (Lyrica Starting dose: 50 -75 mg (1 -3 times/day) Usual")
® (Lyrica ) Pregabalin (Lyrica Starting dose: 50 -75 mg (1 -3 times/day) Usual effective dose: 150 -300 mg bid Dizziness, headache, sedation, somnolence, ataxia Withdrawal (if suddenly stopped): headache, confusion, seizures, sweating Expensive ADA statement. Diabetes Care 2017; 4: 136 Zaccara G, et al. Epilepsia 2011; 52: 826.
 Starting dose: 100 -300 mg (1 -3 times/day) Usual effective")
Gabapentin ® (Neurontin ) Starting dose: 100 -300 mg (1 -3 times/day) Usual effective dose: 900 -3600 mg/day Dizziness, ataxia, somnolence Generic available. Low cost Effective, but dose may be limited by side effects ADA statement. Diabetes Care 2017; 4: 136 Bril V, et al. Neurology 2011; 76: 1758.
 at bedtime")
Tricyclic antidepressants Amitriptyline mostly used Start 25 mg (10 mg for elderly) at bedtime Usual effective dose: 50 -100 mg/day Dry mouth, dizziness, sedation, urine retention, blurred vision, cardiac ischemia May not be suitable for the elderly Nortriptyline & desipramine have less side effects Low cost ADA statement. Diabetes Care 2017; 4: 136

DM & the kidneys • Diabetes is the commonest cause of CKD & dialysis • Check Urine albumin-to-creatinine ratio (UACR) yearly • Serum creatinine e. GFR at least once yearly • Serum K+ periodically if on ACEI, ARB or diuretics

Screening for diabetic kidney disease Urine albumin: creatinine ratio • Type 2 DM: - At the time of diagnosis then yearly • Type 1 DM: - Start 5 years after diagnosis then yearly American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151

Diabetic kidney disease • Albuminuria and/or • Low e. GFR • Patients usually have: – Long duration of DM – Retinopathy (usually in type 1 DM) • Some patients have low e. GFR with no albuminuria American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151

Urine albumin: creatinine ratio • If high: – Repeat • Causes of transient high UACR: – Exercise within 24 hours, infection, fever, menses, heart failure, marked hyperglycemia, uncontrolled B. P. • Albuminuria: 2 out of 3 abnormal within 3 -6 months American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151

Management of Albuminuria • Glucose control • Blood pressure control • ACEI or ARB • Combination of ACEI & ARB is not recommended • Follow UACR & electrolytes • ACEI/ARB are not recommended for primary prevention of diabetic kidney disease (normal B. P. & normal UACR) American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151

When to refer to nephrology? • Uncertainty about the etiology of kidney disease • Active urinary sediment (RBC, WBC or cellular casts) • Rapidly increasing albuminuria • Nephrotic syndrome, rapidly decreasing e. GFR • Advanced kidney disease (e. GFR < 30) • Difficult management issues (anemia, secondary hyperparathyroidism, metabolic bone disease, resistant hypertension or electrolyte disturbances) American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151
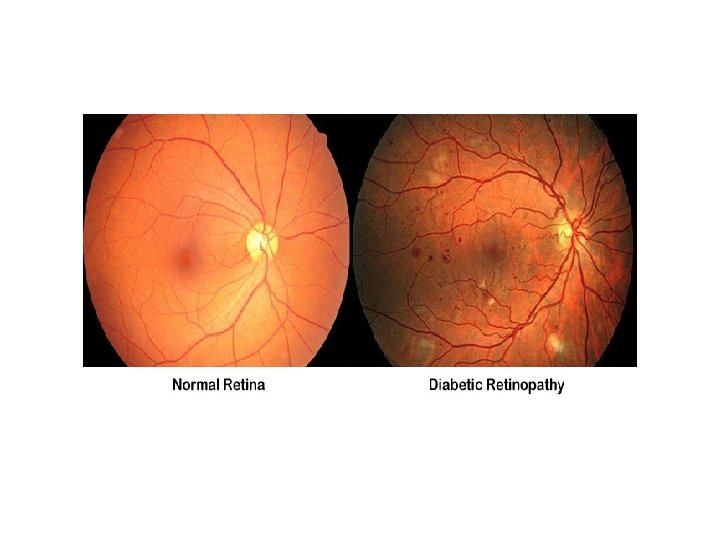

Diabetes and the eyes • Diabetic retinopathy is the major cause of blindness in adults – A silent disease – When symptoms occur, treatment becomes difficult • Risk of cataract & glaucoma • Hypertension is a risk factor for macular edema American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151

Screening for diabetic retinopathy Dilated eye examination • Type 2 DM: - At the time of diagnosis then yearly • Type 1 DM: - Start 5 years after diagnosis then yearly American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151

Measures for diabetic retinopathy • Glucose control • BP control • Lipid control • Aspirin is not contraindicated. – It does not risk of retinal bleeding American Diabetes Association. Diabetes Care 2021; 44 (suppl 1): S 151
 in diabetes • 3 times increased risk compared with non-diabetics •")
Erectile dysfunction (ED) in diabetes • 3 times increased risk compared with non-diabetics • 50 -86% of patients older than 50 years • Risk increases with hypertension, CAD • Under-reported by patients • Under-recognized, less attention by physicians Giuliano F, et al. Urology 2004; 64: 1196

Physical examination • B. P. • Vascular • Neurologic • Asses hair distribution • Look for gynecomastia • Genital exam.

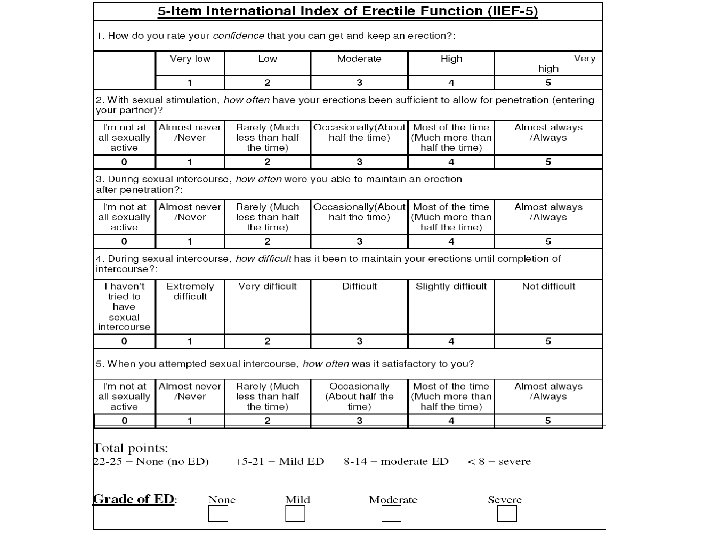
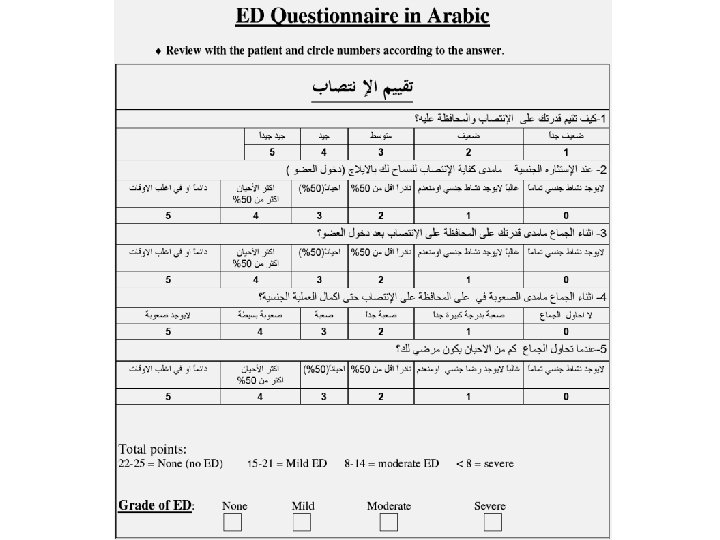
How do we assess if the patient has ED? International Index of Erectile Function (IIEF-5)

Laboratory evaluation • AM total testosterone • If abnormal, order – Prolactin – LH European Association of Urology 2014

Management of ED in diabetes Control glucose did not improve erections Control B. P & lipids did not improve erections Weight loss (1/3 of patients improved) Stop smoking Change offending medications
, Tadalafil (Cialis®), Vardenafil (Levitra®)")
Drug therapy for ED • PDE-5 inhibitors: - Sildenafil (Viagra®), Tadalafil (Cialis®), Vardenafil (Levitra®) - 1 st line treatment - They facilitate, but do not initiate an erection - Efficacy 60 -70 % • If no response, refer to urology (intracorporal injections, pellets) Hatzimouratidis K, et al. Eur Urol 2010; 57: 804 Jannini E, et al. J Sex Med 2009; 6: 2547

Can complications of diabetes be prevented?

DCCT Diabetes Control and Complication Trial • • Can tight glucose control affect complications? Study started in 1977 1441 patients with type 1 DM Divided into 2 groups Conventional therapy (insulin 2/day) Intensive therapy (insulin 3 -4/day or pump)
 Conventional therapy Intensive therapy Mean A 1 c =")
Results of DCCT (announced 1993) Conventional therapy Intensive therapy Mean A 1 c = 9 % Mean A 1 c = 7. 2

Effect of intensive glucose control in DCCT 63 % Retinopathy DCCT Research Group. N Engl J Med. 1993; 329: 977. 54 % Nephropathy 60 % Neuropathy

DM 1 and cardiovascular disease • Intensive group had 44 % less risk of: • Myocardial infarction Cumulative incidence of MI, stroke, CVD death 0. 08 • Stroke • Death from CVD 0. 06 Conventional therapy 0. 04 P<0. 001 0. 02 Intensive therapy 0 0 2 4 6 8 10 Years DCCT/EDIC Study Research Group. N Engl J Med 2005; 353: 2643 12 14 16 18
")
How about type 2 DM? UKPDS (United Kingdom Prospective Diabetes Study)

UKPDS • • Glucose control & complications in type 2 DM 5102 patients with type 2 DM Divided into 2 groups Diet then oral drugs then insulin Conventional therapy Intensive therapy (usual care) (aim at normal levels) Had mean A 1 c 7. 9 Had mean A 1 c 7. 0

Results of UKPDS Effect of Hb. A 1 c by 1 % 14 % Myocardial infarction 12 % 21 % stroke 37 % Microvascular disease (kidney, eye, nerve) Stratton et al. BMJ 2000; 321: 405 Any complication 43 % Amputations
 Treat complications /prevent recurrence (Secondary prevention)")
Goals in diabetes Prevent complications (Primary prevention) Treat complications /prevent recurrence (Secondary prevention)

Keys of diabetes care The diabetes team Patient Physician Educator/ dietitian Pharmacist, Podiatrist, Social worker, Psychiatrist Bergenstal R. Endo Practice 2006; 12(Supp 1): 98

Summary: key points • Diabetes causes micro- & macrovascular complications • Macrovascular (coronary artery disease, stroke, PAD) • Microvascular (eye, kidney, nerves) • Glucose control can reduce the risk of complications • Screening for complications is vital
- Slides: 57