Complication of brachial artery access for the recanalization

Complication of brachial artery access for the recanalization of severe bilateral SFA lesion Jihun Ahn Soonchunhyang university Gumi Hospital
> I have no relevant financial relationships Examples of relationships")
<First Name> <Last Name>, <Degree(s)> I have no relevant financial relationships Examples of relationships are: Advisory Board/Board Member, Consultant, Honoraria, Research Support, Speaker’s Bureau, Stockholder Please list full company name

Case Report Sex/ Age : F/85 C/C : Small ulcer on great foot Rt. P/Hx : HTN (+) DM (-) Bipolar hemiarthroplasty femur Rt.

Lower extremity CT

Target : Right SFA & BTK Left femoral approach

Right Brachial Approach 6 Fr. Shuttle sheath

Right side angiogram

We have just one cath-room STEMI pts was admitted to our hospital We postpone the procedure a hour later after agreement of the patients and her family Maintain the brachial sheath

Balkin sheath Terumo wire -> Connect

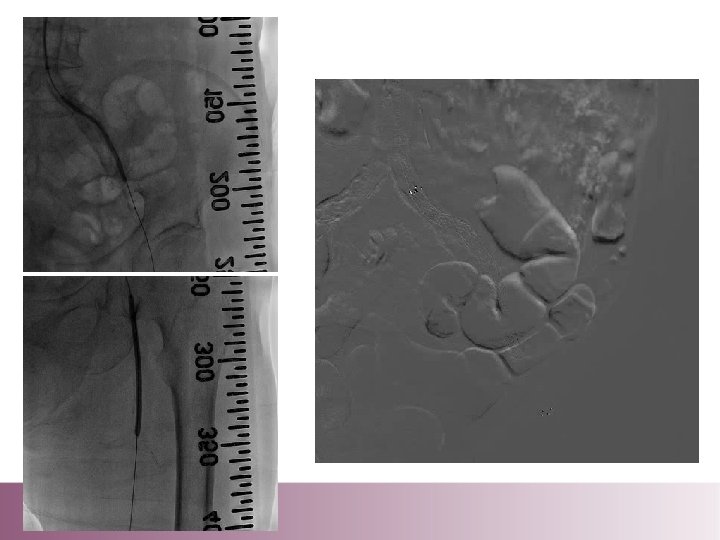
POBA of peroneal artery

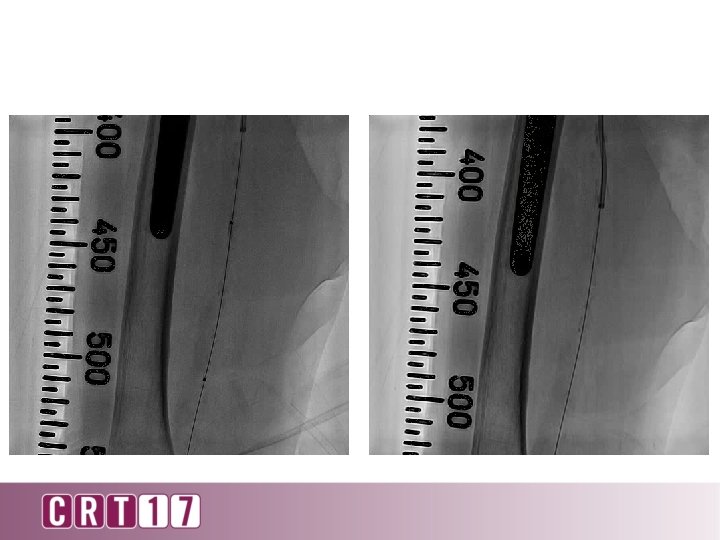
SFA stenting

A day after procedure Painful swelling of Rt. Forearm -> Puncture site (Even persistent compression)

Rt. Feroral approach Micro puncture set 6 Fr. JR 4 Catheter
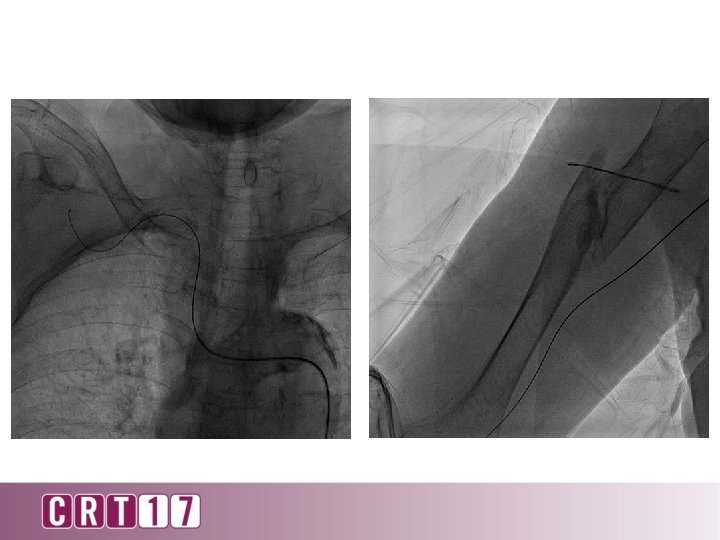

Angiogram

Mannual comppresion for 30 minutes

Balloon compression

Surgical correction was done

The patient was transferred to intensive care unit And expired cause of ARDS with pneumonia

• Brachial artery access is necessary for complex endovascular procedures and can be achieved in most patients safely. • Mannual hand compression is still gold-standard hemostasis. Sometimes compression in difficult because the artery is very movable and have a tendency to roll beneath the finger. • Micro-puncture set & Sono-guided puncture is sometimes helpful. • Access site complication is reported 6 -11%. • Female gender & long sheath is related with complication. • Surgical correction is required frequently compare with other access site complication.
- Slides: 22