Compartment Syndrome Introduction Acute Compartment Syndrome occures when














- Slides: 20
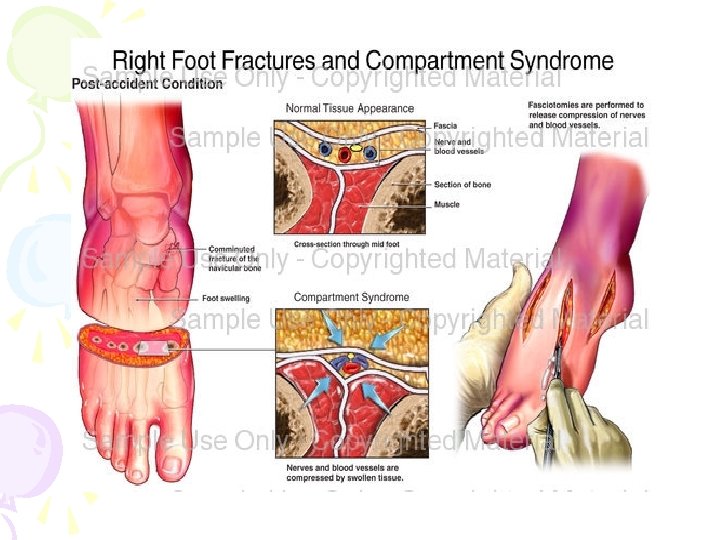
Compartment Syndrome: Introduction Acute Compartment Syndrome: occures when pressure rises in a compartment, resulting in a critical reduction of blood flow to the tissue.
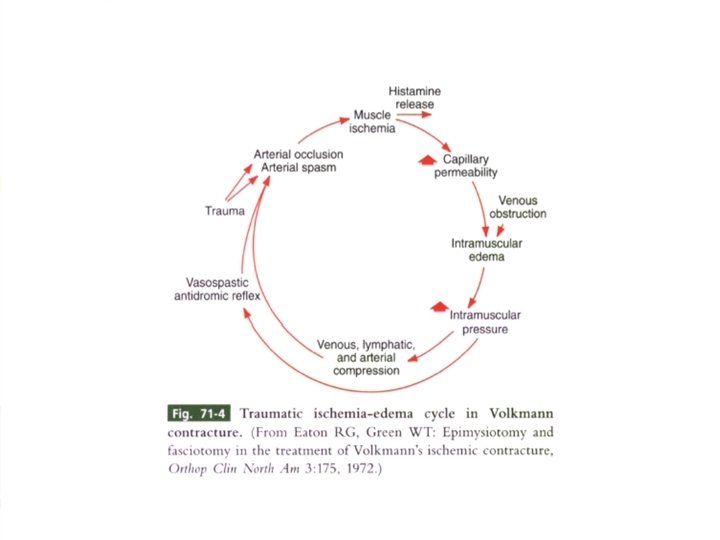
Volkmann`s ischemic contracture Is the end stage of neglected acute compartment syndrom with irreversible muscle necrosis leading to ischemic contractures.
The crush syndrome: The systeic result of muscle necrosis caused by prolonged external compression of an Extremity.
Epidemiology The underlying condition causing it : MOST COMMONLY: a fracture 2 nd most common cause: Soft tissue injury (crush type injury)
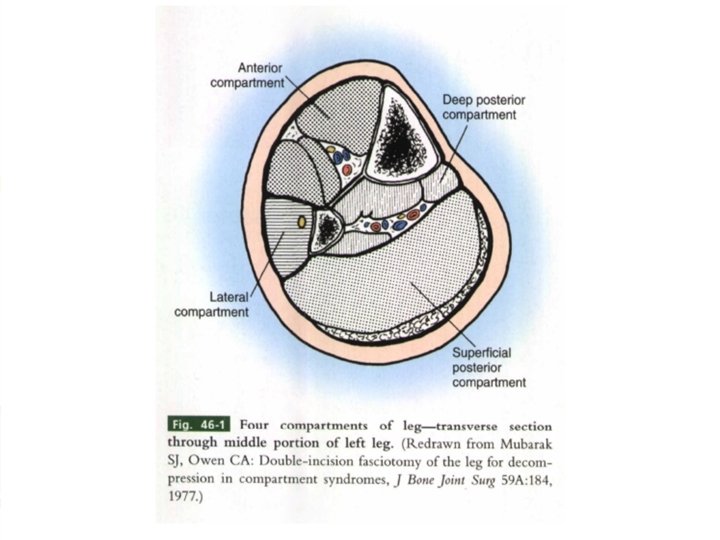
Effects of raised tissue pressure on: Muscles erve Nerve one
Reperfusion injury: Is a group of complications following reestablishment of blood flow to the ischemic tissue. Can occur after fasciatomy & restoration of muscle blood flow.
Clinical DX: Pain Paresthesia Paralysis of limb & hyposthesia Swelling Absence of peripheral pulses Parasis & paralysis
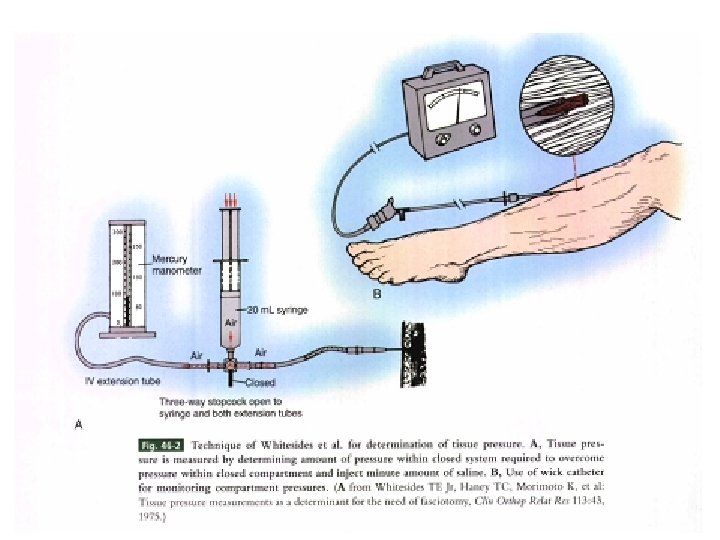
Compartment pressure monitoring: Needle manometer method wick catheter lit catheter
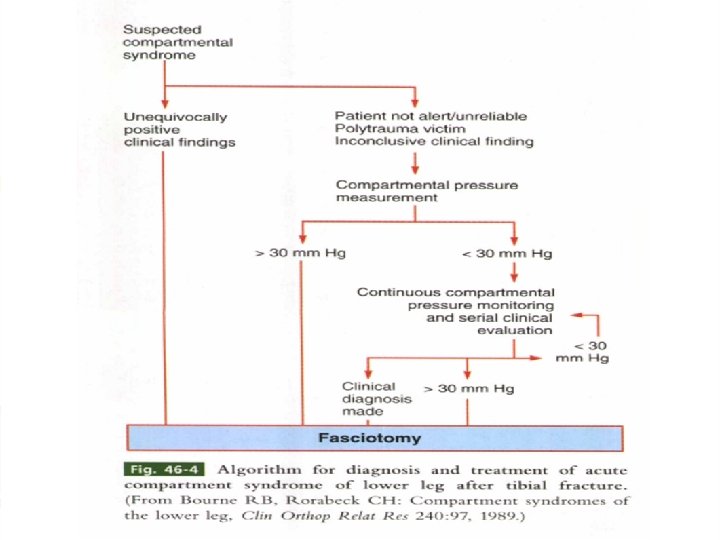
Timing: Time factors are also important in making the decision to proceed to faciotomy.
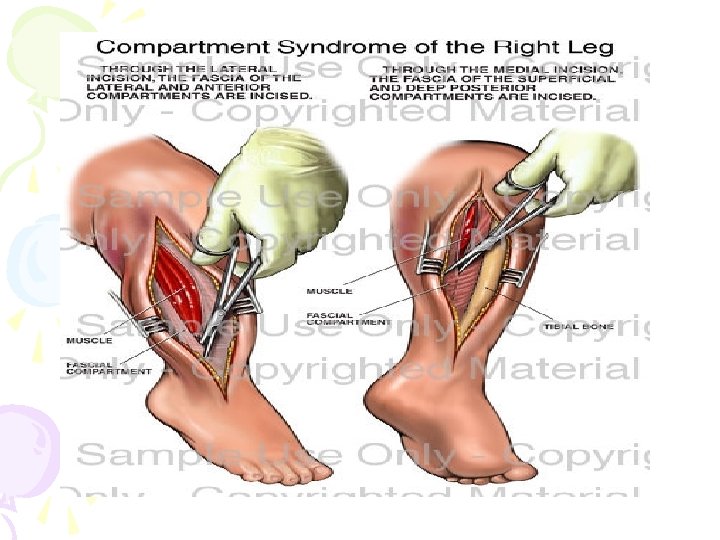
Treatment: The single most effective treatment for acute compartment syndrome is: Fasciotomy ( single/ double incision)
Management of Fasciotomy wounds: Incisions must never be closed primarily because this may result in persistent elevation of ICP. 48 h after, a” 2 nd look “ procedure should be undertaken to ensure the viability of all muscles. The wounds may then be closed by delayed primary closure if possible.
Complications list for Compartment Syndrome: Muscle contracture Muscle weakness Sensory loss Infection fractures
Late diagnosis: Delay in Dx has been cited as the single reason for failure in the management of acute compartment syndrome. Delay to fasciotomy of more than 6 hs is likely to cause significant complications.