Compartment syndrome Fat embolism AVNAvascular Necrosis Malunion non




סיבוכים מאוחר / מיידי הלם Compartment syndrome Fat embolism AVN=Avascular Necrosis Malunion / non union


Rest Immobilization Compression Elevation







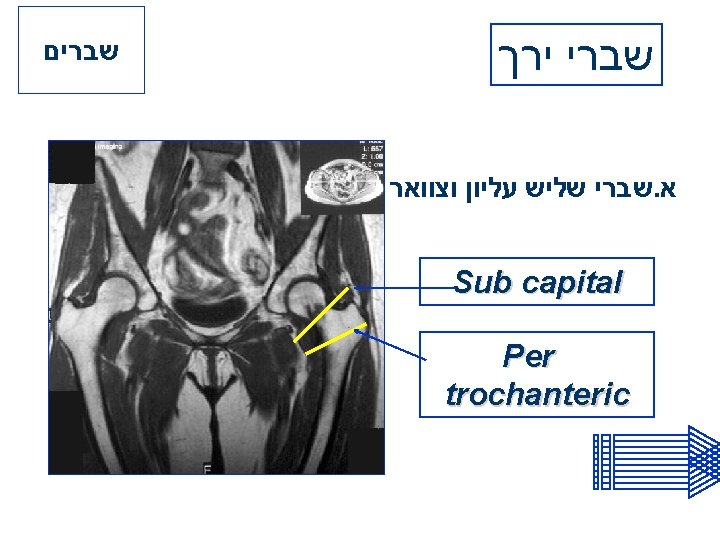


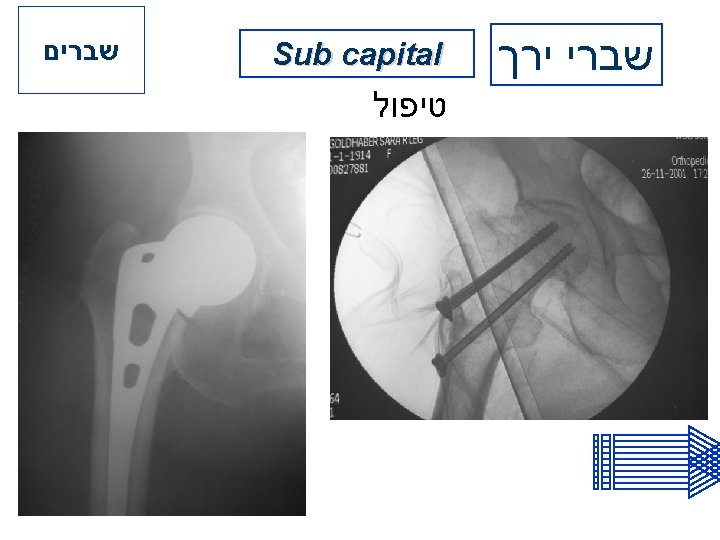
שברים Sub capital שברי ירך GARDEN’S classification

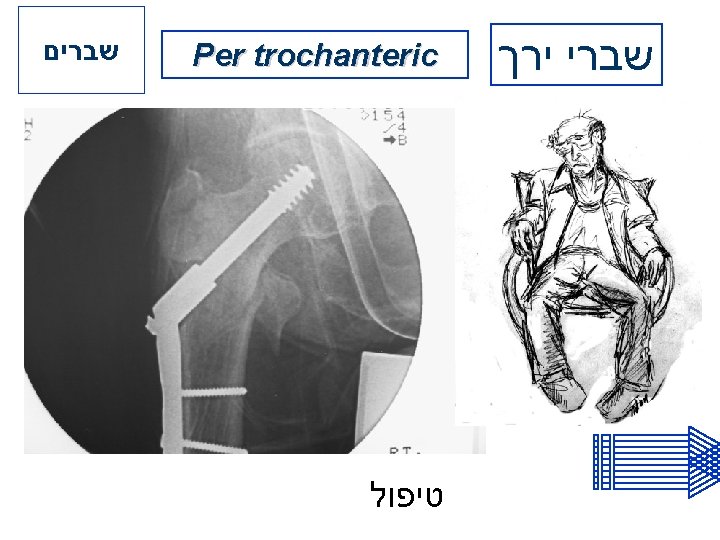
שברים Per trochanteric שברי ירך












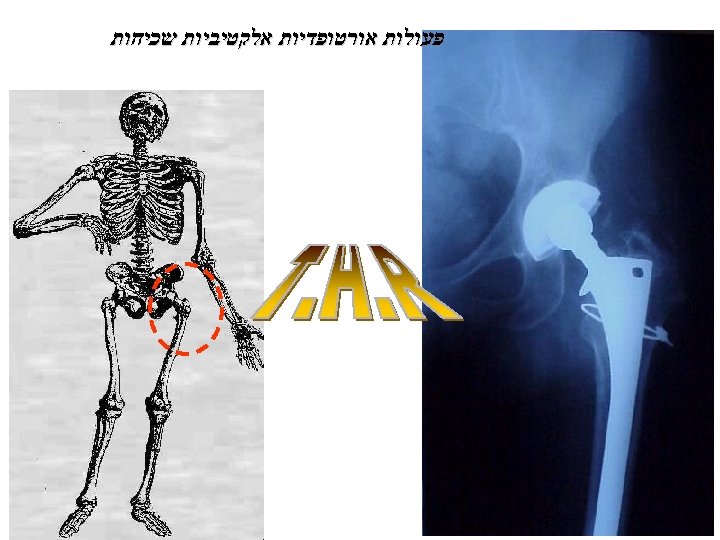

do we total replacements? restricts not When only work andconsider recreation, buthip also the ordinary activities of daily living pain is not relieved by anti-inflammatory medicine, pain is not relieved by the use of a cane vere arthritic conditions significant stiffness of the ays show advanced arthritis, or other problems: hip fractures aseptic necrosis over 55 years of age

What can be expected of a total hip replacement? Pain relief in 90 to 95 percent of patients. Allow patients to carry out many normal activities of daily living. Most patients with stiff hips before surgery will regain near-normal motion, and nearly all have improved motion

The risks of total hip replacement? Total hip replacement is a major operation. The effect of most complications is simply that the patient stays in the hospital longer. The most common complications are not directly related to the hip and do not usually affect the result of the operation. These include:

Vein thrombosis in the leg Urinary infections or difficulty urinating Pulmonary emboli

Complications that affect the hip are less common, but in these cases, the operation may not be as successful: difference in leg length stiffness dislocation of hip infection in hip

A few of the complications, such as infection or dislocation, may require reoperation. Infected artificial hips sometimes have to be removed, leaving a short (by one to three inches), somewhat weak leg, but one that is usually reasonably comfortable and one on which he can walk with the aid of a cane or crutches.

How do artificial hips stand up over time? 90 to 95 percent of hip replacements are successful up to 10 years. The major long-term problem is loosening of the prosthesis. By 10 years, 25 percent of all artificial hips will look loose on x-ray. Somewhat less than half of these (about 5% to 10% of all artificial hips) will be painful and require revision.

Charnley 18 Y post op

Preparing for Surgery Preparing for a total hip replacement begins several weeks ahead of the actual surgery date. Maintaining good physical health before operation is important. Activities which will increase upper body strength will improve patient’s ability to use a walker or crutches after the operation.

Post Surgery There are some precautions, mostly to prevent dislocation, which is more likely to occur the first six to eight weeks after surgery. These precautions include: using 2 -3 pillows between the legs and not crossing the legs not bending forward 90 degrees using a high-rise toilet seat

Initial rehabilitation The first day after surgery the patient will be assisted to a reclining chair, and physical therapy may begin. The patient will gradually begin to take steps, walk, and learn to climb stairs with the aid of a walker or crutches.

This initial rehabilitation generally takes 5 -7 days. During this time, discomfort may be experienced while walking and exercising. Pain medication will be ordered as needed. Most patients are relieved of their painful pre-surgical hip condition.

Therapy and rehabilitation program Following surgery, the patient will work with a physical therapist to become independent in walking, going up and down stairs, getting in and out of bed, and doing exercises to improve the range of motion and strength of his hip.

The patient will be instructed by his physical therapist in a specific home exercise program to meet his needs. If an exercise is causing pain that is lasting, the patient should reduce his intensity. If it continues to cause pain, he should contact his physical therapist or physician.

Home Exercises Range of motion exercises Active hip and knee flexion: Lying on your back with legs straight, toes pointed toward the ceiling; arms by your side. Keeping the heel in contact with the bed, bend your hip and knee. Return to starting position. Progress to 20 repetitions, 2 times a day.
 under your")
Active Abduction: Place a smooth surface (card table, plywood sheet, etc. ) under your legs. Begin with your legs together, then move the operated leg out to the side as far as you can. Keep your toes pointed toward the ceiling. Return to the starting position. Progress to 20 repetitions, 2 times a day.

Strengthening Exercises Quadriceps Setting: Tighten the muscles on the top of your thigh, pushing the back of your knee downward into the bed. The result should be straightening of your leg. Hold for 5 seconds, relax 5 seconds. Progress to 20 repetitions, 2 times a day.

Gluteal Setting: Lie either on your back with your legs straight and in contact with the bed. Tighten your buttocks in a pinching manner and hold the isometric contraction for 5 seconds, relax 5 seconds. Progress to 20 repetitions, 2 times a day.


estrict not only work but also When doand werecreation, consider total kneethe replacements? living pain is not relieved by anti-inflammatory medicine, pain is not relieved by the use of a cane vere arthritic conditions significant stiffness of the x-rays show advanced arthritis, or other problems: aseptic necrosis over 55 years of age

What can be expected of a total knee replacement? Pain relief in 90 to 95 percent of patients. Allow patients to carry out many normal activities of daily living. Most patients with stiff knees before surgery will regain improved motion




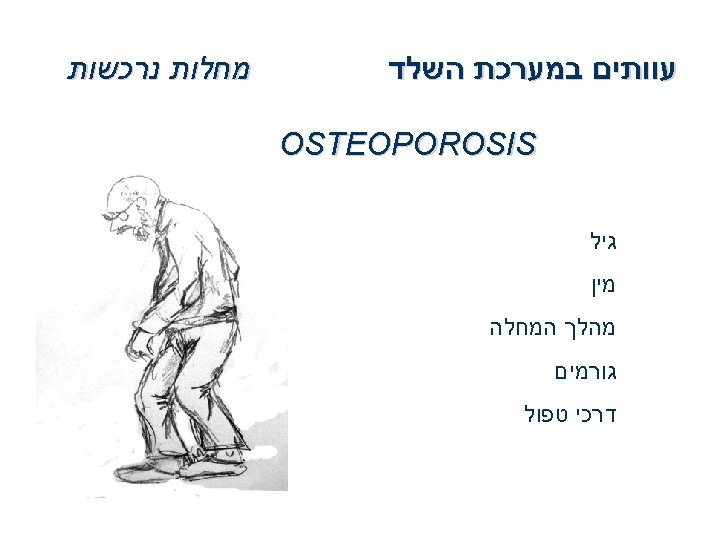
מחלות נרכשות Bunionectomy Keller Chevron עוותים במערכת השלד HALLUX HAMMER +VALGUS TOE


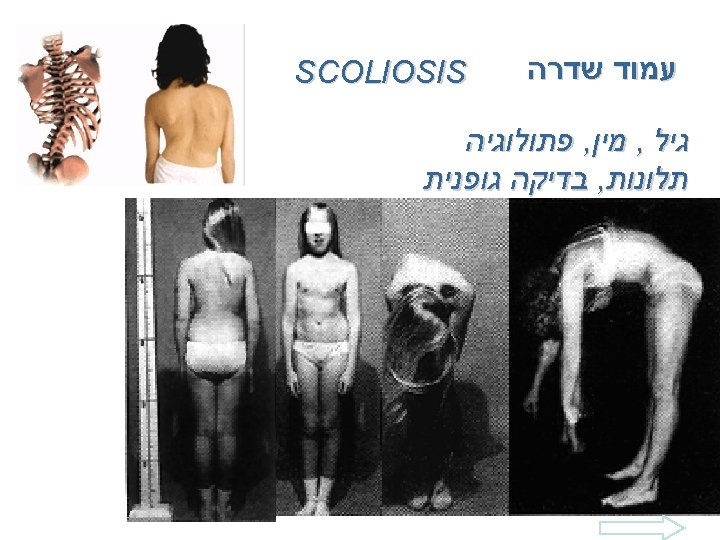

SCOLIOSIS

Pseudo-Scoliosis Antalgic Postural Scoliosis ?

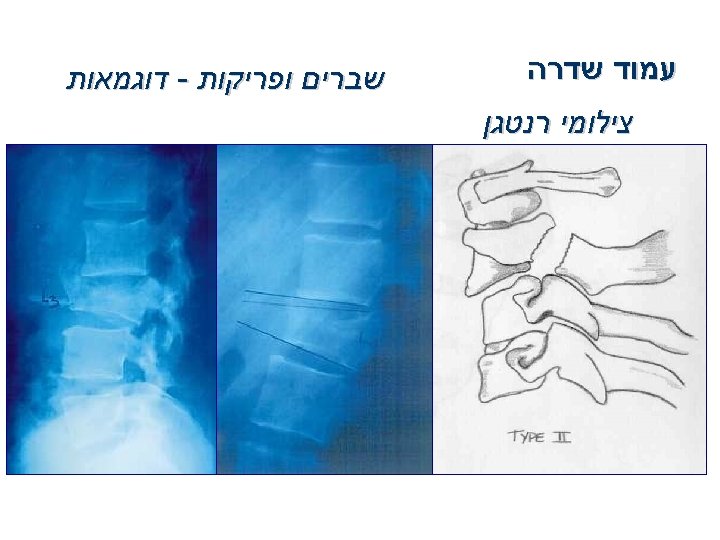

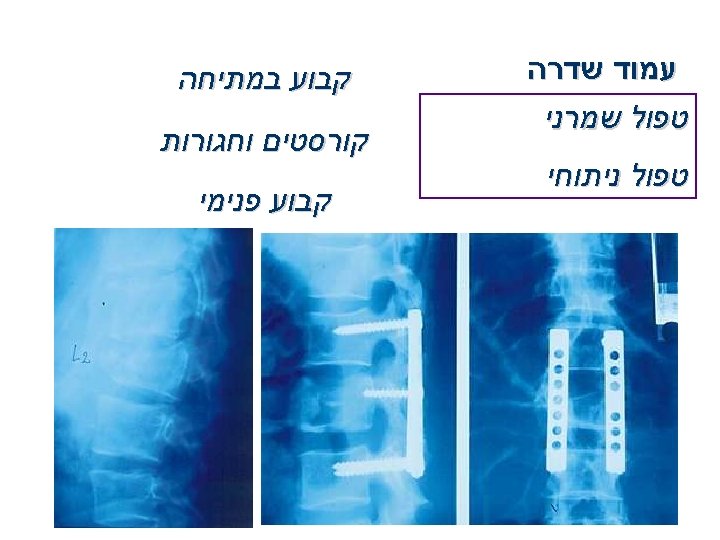


שברי עמוד שדרה Pathologic Other than Osteoporotic MM

Nerve Compression syndromes

Nerve Compression syndromes Median Nerve

Nerve Compression syndromes Ulnar Nerve


- Slides: 96