CommunityAcquired Pneumonia CommunityAcquired Pneumonia A 67 yearold woman

















































- Slides: 54
Community-Acquired Pneumonia
Community-Acquired Pneumonia • A 67 -year-old woman with mild Alzheimer’s disease who has a 2 -day history of • Productive cough • Fever • Increased confusion • No recent hospitalizations • No recent use of antibiotic agents Transferred from a nursing home to ED.
Community-Acquired Pneumonia A 67 -year-old woman………… • • • Temp 38. 4°C blood pressure is 145/85 mm Hg respiratory rate is 30 breaths per minute, heart rate is 120 beats per minute, oxygen saturation is 91% Crackles are heard in both lower lung fields.
Community-Acquired Pneumonia THE CLINICAL PROBLEM • Forgotten killer. • WHO estimates that lower respiratory tract infection is the most common infectious cause of death in the world • Third most common cause overall The top 10 causes of death. Geneva: World Health Organization, 2013 (http: // www. who. int/mediacentre/factsheets/ fs 310/en/index. html).
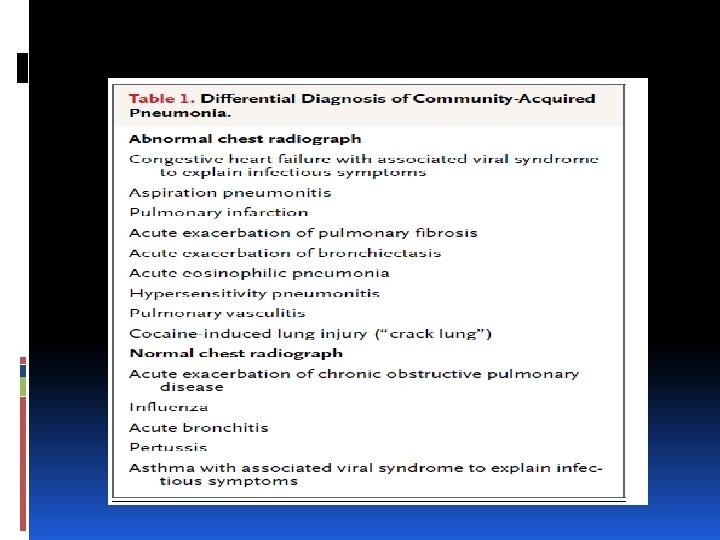
Community-Acquired Pneumonia STRATEGIES AND EVIDENCE DIAGNOSIS • The diagnosis in patients who do not have underlying cardiopulmonary disease. • In patients with lung cancer, pulmonary fibrosis or other chronic infiltrative lung disease, or congestive heart failure, the diagnosis of community-acquired pneumonia can be very difficult.
Community-Acquired Pneumonia Key Clinical points • The majority of hospitalized patients can be treated with either a respiratory fluoroquinolone or a combination of cephalosporin and a macrolide.
Community-Acquired Pneumonia Key Clinical points Alternative antibiotic should be based on the presence of multiple risk factors • specific risks (e. g. , structural lung disease) • uniquely characteristic syndromes (e. g. , the toxin-mediated • community-acquired, methicillin-resistant Staphylococcus aureus syndrome). • recent antibiotic use
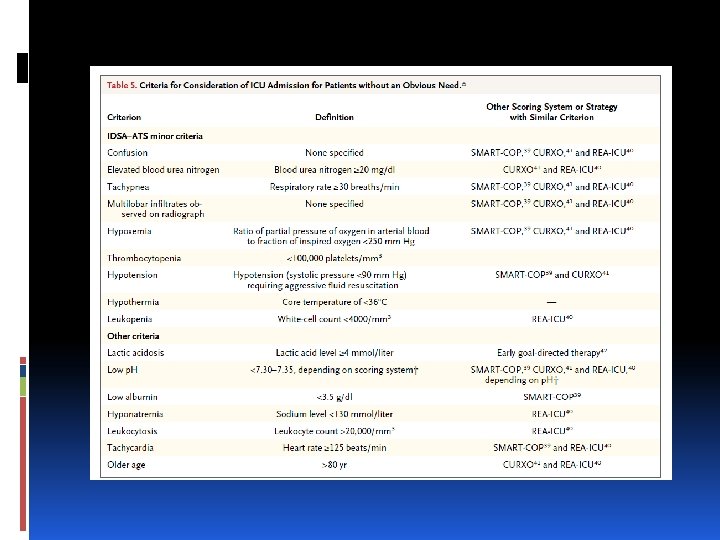
Community-Acquired Pneumonia Key Clinical points • Patients with three or more minor criteria for severe community-acquired pneumonia (e. g. , elevated blood urea nitrogen, confusion, and a high respiratory rate) should receive extensive intervention in the emergency department and be considered for admission to the intensive care unit.
Community-Acquired Pneumonia A triad accurately identifies a patient with community-acquired pneumonia • evidence of infection (fever or chills and leukocytosis), • signs or symptoms localized to the respiratory system (cough, increased sputum production, shortness of breath, chest pain, or abnormal pulmonary examination), and • a new or changed infiltrate in xray
Community-Acquired Pneumonia • Confusion may be the only presenting symptom in elderly patients, leading to a delay in diagnosis. Waterer GW, Kessler LA, Wunderin RG. Delayed administration of antibiotics and atypical presentation in communityacquired
Community-Acquired Pneumonia • Infiltrates on radiographs may also be subtle • Two radiologists reading the same chest radiograph disagree in 10% of cases. Albaum MN, Hill LC, Murphy M, et al. Interobserver reliability of the chest radiograph in community-acquired pneumonia. Chest 1996; 110: 343 -50.
Community-Acquired Pneumonia INITIAL MANAGEMENT Choice of Antibiotic Therapy • Choice of antibiotic therapy • Extent of testing to determine the cause of the pneumonia • Appropriate location of treatment (home, inpatient floor, or ICU).
Community-Acquired Pneumonia • The key to appropriate therapy is adequate coverage of Streptococcus pneumoniae and the atypical bacterial pathogens (mycoplasma, chlamydophila, and legionella).
Community-Acquired Pneumonia • For outpatients, the coverage of atypical bacterial pathogens is most important, especially for young adults. • Macrolides, doxycycline, and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens.
Community-Acquired Pneumonia • recommend first-line treatment with either a respiratory fluoroquinolone (moxifloxacin at a dose of 400 mg per day or levofloxacin at a dose of 750 mg per day) or the combination of a second-generation or third-generation cephalosporin and a macrolide.
Community-Acquired Pneumonia • Although S. pneumoniae remains the most common cause of severe communityacquired pneumonia requiring ICU admission, combination therapy consisting of a cephalosporin with either a fluoroquinolone or a macrolide is recommended. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44: Suppl 2: S 27 -S 72.
Community-Acquired Pneumonia • for patients in shock; antibiotics should be given within the first hour after the onset of hypotension. • An observational study involving patients with septic shock showed a decrease in survival rates of 8% for each hour of delay. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006; 34: 1589 - 96.
Community-Acquired Pneumonia Duration of Antibiotic Treatment • The currently recommended duration of antibiotic therapy for community-acquired pneumonia is 5 to 7 days. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44: Suppl 2: S 27 -S 72.
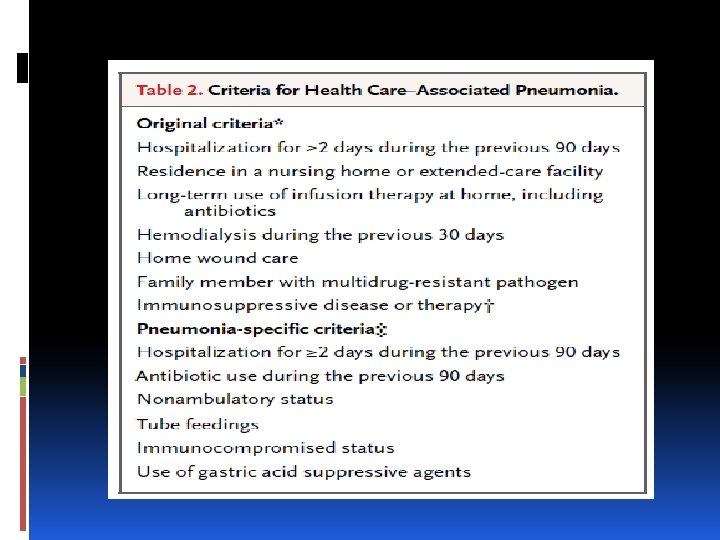
Community-Acquired Pneumonia TREATMENT OF PATIENTS AT RISK FOR RESISTANT ORGANISMS • Health care–associated pneumonia has been categorized as a discrete entity, with the goal of identifying patients with pneumonia that develops outside the hospital yet is caused by pathogens usually associated with hospital-acquired pneumonia or even ventilator-associated pneumonia, including methicillin-resistant Staphylococcus aureus (MRSA) and multidrug-resistant (MDR) gram-negative pathogens.
Community-Acquired Pneumonia TREATMENT OF PATIENTS AT RISK FOR RESISTANT ORGANISMS • Empirical broad-spectrum therapy with dual coverage for Pseudomonas aeruginosa and routine MRSA coverage American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcareassociated pneumonia. Am J Respir Crit Care Med 2005; 171: 388 -416.
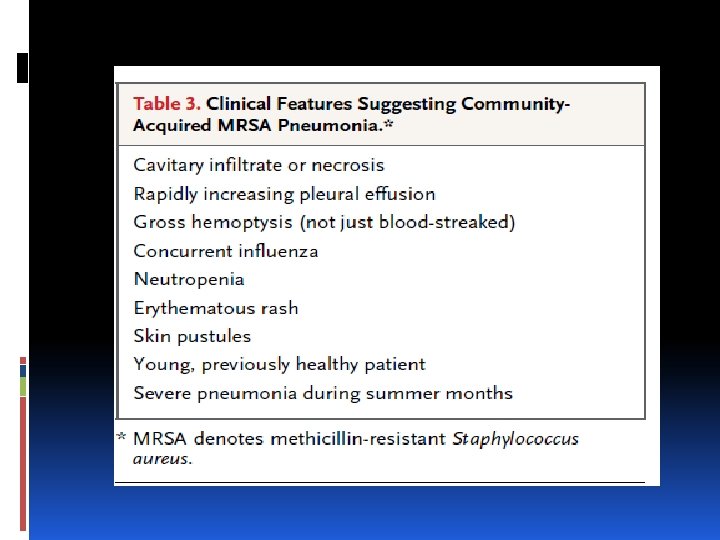
Community-Acquired Pneumonia • MRSA • Exotoxin production by this strain (as well as by the methicillin-sensitive variant) results in characteristic presenting features (Table 3).
Community-Acquired Pneumonia • MRSA • Treatment is recommended with antibiotics that suppress toxin production, such as linezolid or clindamycin (added to vancomycin); these regimens have been associated with reduced mortality. Sicot N, Khanafer N, Meyssonnier V, et al. Methicillin resistance is not a predictor of severity in community-acquired Staphylococcus aureus necrotizing pneumonia: results of a prospective observational study. Clin Microbiol Infect 2013; 19: E 142 -E 148.
Community-Acquired Pneumonia in Older Children and Adults: Outpatient Treatment CLINICAL SETTING ANTIBIOTIC REGIMEN COMMENTS Doxycycline Preferred for adolescent/young 100 mg PO adult when likelihood of mycoplasma is high; variable Previously bid healthy, no level III evidence activity vs. S. pneumoniae. antimicrobi • For typical bacterial and atypical. als in last Variety of dosing regimens: 3 mo Azithromycin 500 mg once then 250 mg od for * 4 500 mg PO daily for 3 days level I evidence) 2 g extended release suspen. once. • Can substitute clarithromycin.
Community-Acquired Pneumonia in Older Children and Adults: Outpatient Treatment CLINICAL SETTING ANTIBIOTIC REGIMEN COMMENTS Comorbidities, Levofloxacin level I Can substitute moxifloxacin or or antimicrobials 750 mg PO daily gemifloxacin. in last 3 mo for 5 days Treats common typical and atypical bacterial pathogens; active vs. DRSP. Use if recently received β-lactam or macrolide. level 1 Use if recently received Cefpodoxime fluoroquinolones. Can substitute 200 mg PO bid + cefdinir, cefprozil, or azithromycin amoxicillin/clavulanate for cefpodoxime. 500 mg PO daily Variable activity against DRSP.
Community-Acquired Pneumonia in Older Children and Adults: Inpatient Antimicrobial Treatment CLINICAL SETTING ANTIBIOTIC REGIMEN COMMENTS level I Could substitute Community-acquired, Ceftriaxone 1 g q 24 h + cefotaxime, ampicillinnonimmunocompromis azithromycin 500 mg sulbactam, or ed q 24 h IV or PO ertapenem for ceftriaxone. Respiratory Treats most common fluoroquinolone bacterial and atypical (levofloxacin 750 mg IV pathogens. Active vs. q 24 h or moxifloxacin DRSP. 400 mg IV q 24 h)
Community-Acquired Pneumonia in Older Children and Adults: Inpatient Antimicrobial Treatment CLINICAL SETTING ANTIBIOTIC REGIMEN COMMENTS Ceftriaxone 1 g IV q 24 h + levofloxacin Severe 750 mg IV q 24 h + pneumonia (ICU) vancomycin 1 g IV q 12 h Can substitute cefotaxime, cefepime, ertapenem, or β-lactam/β-lactamase inhibitor for ceftriaxone. Can substitute moxifloxacin for levofloxacin. Can substitute linezolid for vancomycin. Health care– associated pneumonia or severe pneumonia with neutropenia, bronchiectasis (risk for Pseudomonas) Can substitute other antipseudomonal βlactam, such as piperacillin-tazobactam, imipenem, or meropenem, for cefepime. Can substitute aminoglycoside plus macrolide for ciprofloxacin. Cefepime 2 g IV q 12 h + ciprofloxacin 500 mg IV q 12 h + vancomycin 1 g IV q 12 h
Community-Acquired Pneumonia in Older Children and Adults: Inpatient Antimicrobial Treatment CLINICAL SETTING ANTIBIOTIC REGIMEN COMMENTS Add ceftriaxone to TMP/SMX if severe, until PCP confirmed. Alternatives for sulfa allergy Trimethopriminclude pentamidine + third. Presumed PCP sulfamethoxazole 240/1200 mg IV q 6 h generation cephalosporin; clindamycin + primaquine; or atovaquone + ceftriaxone.
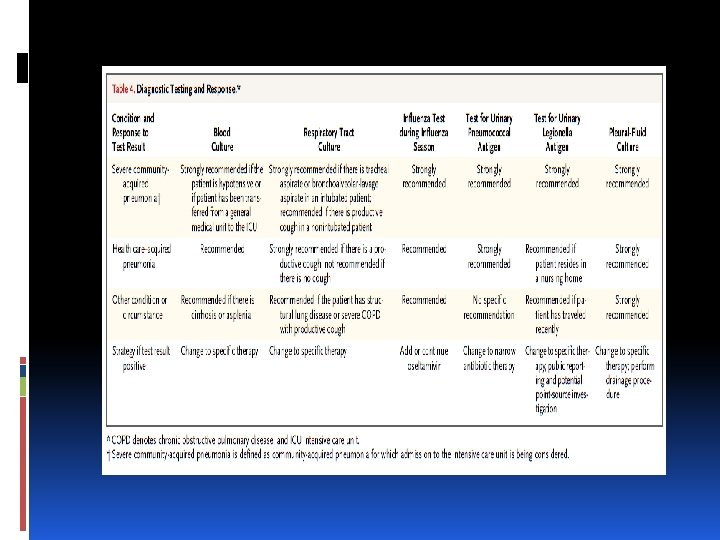
Community-Acquired Pneumonia DIAGNOSTIC TESTING • The extent of testing that is warranted to identify the causative microorganism in community acquired pneumonia is controversial. • Because the recommended antibiotic regimens are effective for the majority of patients, diagnostic testing will rarely affect therapy.
Community-Acquired Pneumonia • Influenza testing in the appropriate season is the diagnostic test that is most likely to affect treatment. • Depending on current local influenza rates, antiviral treatments may be started empirically and stopped if testing is negative, or they may be started only in response to a positive test.
Community-Acquired Pneumonia SITE OF CARE Hospital Admission
Community-Acquired Pneumonia • Scoring systems that predict short-term mortality, such as the Pneumonia Severity Index (PSI)35 and the CURB-65 scores • Use of the PSI results in fewer admissions of patients with mild illness, with no increase in adverse outcomes. • calculating the PSI score is complex Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med 2005; 143: 881 -94. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumoniaseverity on presentation to hospital: an international derivation and validation study. Thorax 2003; 58: 377 -82.
Community-Acquired Pneumonia CURB-65 score (which assigns 1 point each for • Confusion • Uremia [blood urea nitrogen ≥ 20 mg/dl] • respiratory rate ≥ 30 breaths per minute, • SBP <90 mm Hg or DBP ≤ 60 mm Hg • age ≥ 65 years score ≥ 3 indicating the need for hospitalization • Easy to remember and calculate but has not been as well validated as the PSI score.
Community-Acquired Pneumonia • Individual decisions that are inconsistent with the score are often made for legitimate reasons • …. . objective (e. g. , low arterial saturations) • …. . subjective (e. g. , unreliable home support and concern regarding adherence to therapy).
Community-Acquired Pneumonia ICU Admission • Decisions regarding initial admission to the ICU of patients with community-acquired pneumonia and questionable cardiopulmonary stability probably have the greatest potential effect on mortality.
Community-Acquired Pneumonia • A quality-improvement study showed that increased attention in the emergency department resulted in a decrease in mortality (from 23 to 6%) Lim HF, Phua J, Mukhopadhyay A, et al. IDSA/ATS minor criteria aided pre-ICU resuscitation in severe community-acquired pneumonia. Eur Respir J 2013 October 31 (Epub ahead of print).
Community-Acquired Pneumonia Potentially useful interventions include • Aggressive fluid resuscitation • Prompt initiation of appropriate antibiotics • Lactate measurement for borderline hypotension • Treatment of coexisting illnesses (e. g. , administration of bronchodilators for asthma and COPD) • Reassessment after such interventions Lim HF, Phua J, Mukhopadhyay A, et al. IDSA/ATS minor criteria aided pre-ICU resuscitation in severe community-acquired pneumonia. Eur Respir J 2013 October 31 (Epub ahead of print).
Pneumonia Criteria for severe community-acquired pneumonia. • • • RR 30 breaths/min Pa. O 2/Fi. O 2 ratio 250 Multilobar infiltrates Confusion/disorientation Uremia (BUN level, 20 mg/d. L) • Leukopeniac (WBC <4000 cells/mm 3) • platelet count, <100, 000 cells/mm 3) • Hypothermia (<36 C) • Hypotension • Invasive mechanical ventilation • Septic shock with the need for vasopressors
Community-Acquired Pneumonia • Presence of one MRSA-specific risk factor (prior MRSA infection or colonization, longterm hemodialysis, or heart failure) may warrant MRSA coverage (but not dual antipseudomonal antibiotics) Shindo Y, Ito R, Kobayashi D, et al. Risk factors for drug-resistant pathogens in community-acquired and healthcareassociated pneumonia. Am J Respir Crit Care Med 2013; 188: 985 -95
Community-Acquired Pneumonia • A 67 -year-old woman with mild Alzheimer’s disease who has a 2 -day history of • Productive cough • Fever • Increased confusion • No recent hospitalizations • No recent use of antibiotic agents Transferred from a nursing home to ED.
Community-Acquired Pneumonia A 67 -year-old woman………… • • • Temp 38. 4°C blood pressure is 145/85 mm Hg respiratory rate is 30 breaths per minute, heart rate is 120 beats per minute, oxygen saturation is 91% Crackles are heard in both lower lung fields.
Community-Acquired Pneumonia • A 67 -year-old woman with mild Alzheimer’s disease who has a 2 -day history of • Productive cough • Fever • Increased confusion • No recent hospitalizations • No recent use of antibiotic agents Transferred from a nursing home to ED.
Community-Acquired Pneumonia A 67 -year-old woman………… • • • Temp 38. 4°C blood pressure is 145/85 mm Hg respiratory rate is 30 breaths per minute, heart rate is 120 beats per minute, oxygen saturation is 91% Crackles are heard in both lower lung fields.
CONCLUSIONS AND RECOMMENDATIONS A 67 -year-old woman………… • CURB-65 score of 4 • Benefit from inpatient therapy. • She has at least four minor criteria for severe CAP (confusion, respiratory rate ≥ 30 breaths per minute, multilobar infiltrates, and uremia).
CONCLUSIONS AND RECOMMENDATIONS A 67 -year-old woman………… As a nursing home resident, • She meets the current criteria for health care –associated pneumonia. • no pneumonia-specific MDR risk factors but does have risk factors for severe CAP, • we would initiate treatment with ceftriaxone and azithromycin.
CONCLUSIONS AND RECOMMENDATIONS • Influenza testing if she has presented during the appropriate season. • Empirical oseltamivir started if the local influenza rate is high. • No blood cultures nor sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for CAP.
Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults CURB-65 Pneumonia Severity Index (PSI), can be used to identify patients with CAP who may be candidates for outpatient treatment. (Strong recommendation; level I evidence. )
Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults Early treatment (within 48 h of the onset of symptoms) with oseltamivir or zanamivir is recommended for influenza A. (Strong recommendation; level I evidence. )
Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults Use of oseltamivir and zanamivir is not recommended for patients with uncomplicated influenza (level I evidence), These drugs may be used to reduce viral shedding in hospitalized patients or for influenza pneumonia. (Moderate recommendation; level III evidence. )
Thank you