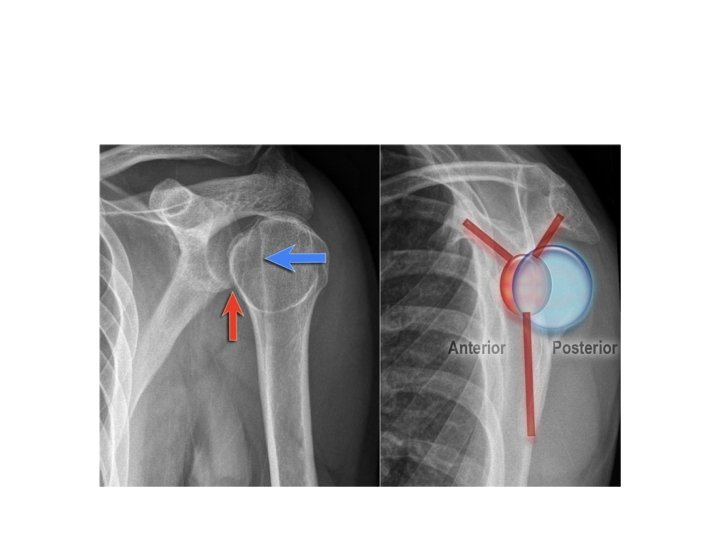
Common pediatric fracture SHOULDER DISLOCATION IN CHILDREN Traumatic













: Type I: undisplaced. Type II:")
















: Closed or open reduction and casting")



- Slides: 44
Common pediatric fracture
SHOULDER DISLOCATION IN CHILDREN -Traumatic is very rare. -Atraumatic can be voluntary or involuntary. -generalized laxity & and child may have glenoid dysplasia. -The shoulder may sublaxate in any direction on examination ( multidirectional instability). Treatment: Some children may have behavioral problems & that is where the Rx should be directed. Prolonged exercise program may help.
Glenoid dysplasia
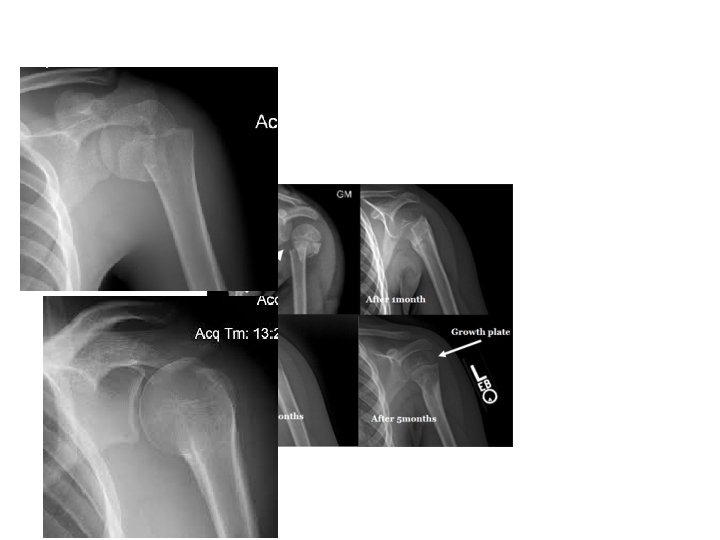
Proximal humerus injuries in children • At birth: brachial plexus injury should be considered. • Infancy: physis separation (Salter-Harris I) may occur, consider child abuse • Older children: metaphysical fx or type II physeal fx occur. displacement & angulation may be accepted; because of the marked growth & remodeling potential of the proximal humerus, treatment most of the cases arm sling only • Pathological fx: • are usual as the proximal humerus is a common site of bone cyst & tumors in children.
Humeral shaft injuries in children Fx are uncommon in children. In children <3 years of age, child abuse should be considered Arm sling for most cases Older children require short plaster splint. Very rare, needs surgery with eleastic nails
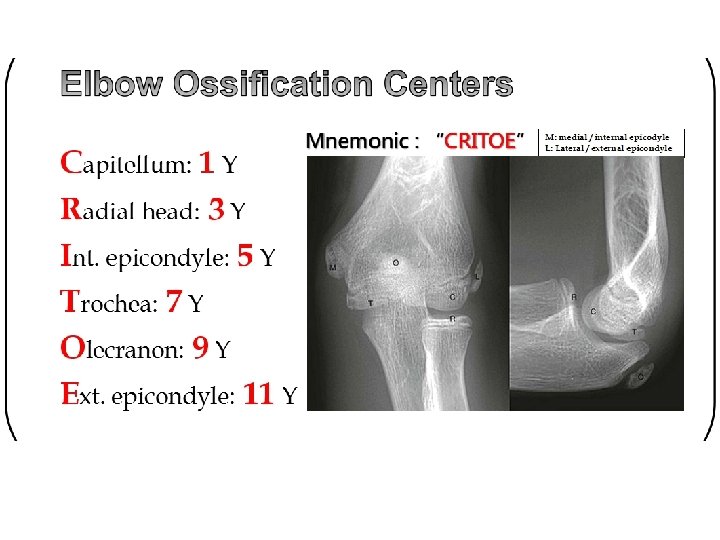
Fx around the elbow in children -2 nd to the distal forearm fractures in frequency. -Most are supracondylar, then condylar, epicondylar, proximal radial or proximal ulnar fx. -Boys are injured more than girls, -usually under 10 yrs -The most common is falling onto the outstretched hand with the elbow forced into valgus or varus. -rarely it is caused by direct injury
ELBOW FRACTURE EXAMINATION • Check neurovascular status ØPalpate brachial and radial pulses. Ø Capillary refill in fingers. Ø Flex and extend fingers and wrist. Ø Oppose thumb and little finger. • Immobilize elbow before radiographs to avoid further injury from sharp fragments. • Don’t reduce before XR 1/21/2022 9
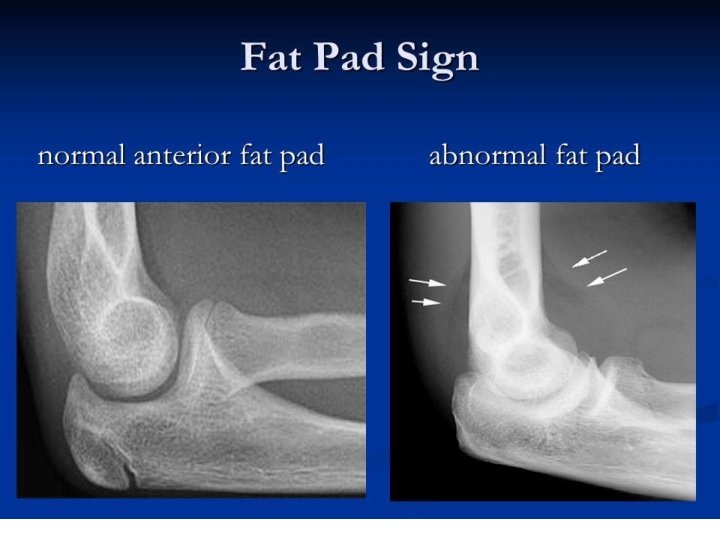
Anterior humeral line: radiographic line that is drawn down the anterior margin of the humerus and through the middle third of the capitellum. 1/21/2022 11
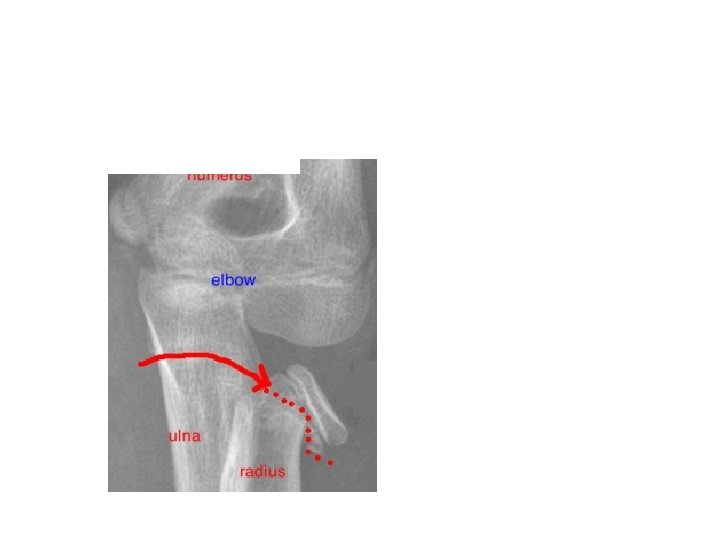
• The radiocapitellar line is made by a line passing through the middle of the radius where it should pass through the capitellum 1/21/2022
• Baumann’s angle: angle between the longitudinal axis of the humeral shaft & the coronal axis of the capitular physis (<80°).
Supracondylar fx in children The distal fragment is displaced posteriorly or anteriorly. 1. Dorsal Angulation or displacement(95%): Hyperextension injury usu. a fall on the stretched hand. The distal fragment is pushed backwards or dorsally The proximal fragment may injure the brachial artery or median nerve. 2. Volar Displacement: Rare. Flexion type Due to direct injury with the joint in flexion.
Supracondylar fx
Extension and flexion types
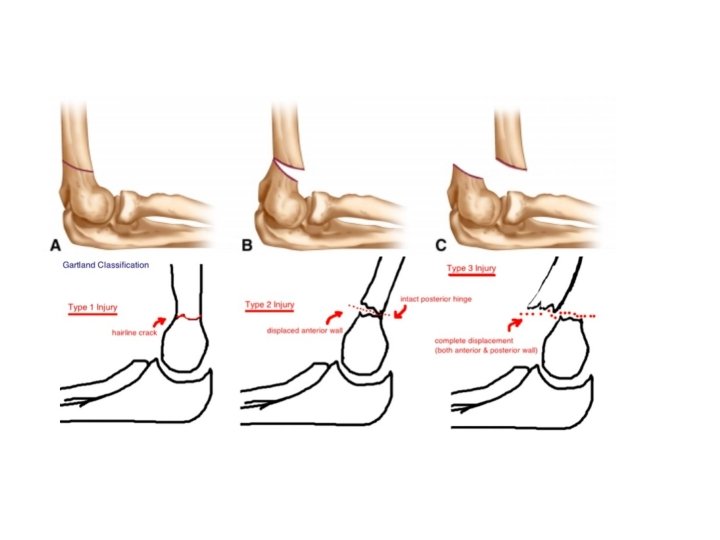
Classification: According to severity & displacement ( Wilking, 1984): Type I: undisplaced. Type II: angulated fx with post. cortex still in continuity: Type II A: less severe & merely angulated. Type II B: more severe & both angulated & mal-rotated. Type III: completely displaced.
Type 1
Type 2
Type 3
• Check N. V • Check capillary refill and pulses • Anterior interosseous neurapraxia is the most common nerve palsy occurring with supracondylar fractures. • The patient will not be able to make an “OK” sign or bend the tip of his index finger. • Ulnar nerve maybe injured especially with flexion type with abdcution –adduction of fingers • Check for compartment syndrome
Check sensation
Treatment • Type one: Nonoperative treatment is usually indicated. splinting or casting the elbow for a duration of 3 -4 weeks Don’t flex the elbow in the splint or cast beyond 90° in order to avoid vascular compromise and compartment syndrome. • Type two can be treated with cast or surgically according to degree od displacement • Type three always needs surgical treatment with reduction and fixation ( closed reduction better than open) and K. Wires
lateral condyle fractures • Falling on the outstretched hand & the elbow is forced into varus. • The condylar epiphysis is largely cartilaginous & the bone fragment may look small on X-ray. • Displacement can be marked due to muscle pull. • The fx is serious: -May damage the growth plate. -It always involves the joint. -Nonunion can happen due to synovial fluids -Malunion can occur (cubitus valgus)
Clinical features: The elbow is swollen & deformed. Tenderness over the lateral condyle. Passive flexion of the wrist may be painful. X-ray: -AP, lateral and oblique views which is the best to evaluate the displacement -2 types of fx: 1 -Fx lateral to the trochlea : humero-ulnar joint is not : involved & is stable. 2 -Fx through the middle of the trochlea: trochlea more common, the elbow is unstable & may dislocate. .
lateral condyle fracture
RX: No or minimal displacement: gap less then 2 ml Splintage for 3 -4 weeks then exercises are encouraged. Keep XRs every week to check that the fracture dose not displace or get nonunited Displaced fx (gap >2 mm): Closed reduction & percutaneous pins can be tried. If fails, open reduction & internal fixation. Then immobilization for 3 -4 weeks of cast
Separation of distal humeral physis -Distal humeral epiphysis may separate With severe violence as in birth injuries or child abuse. Usually very young(less than one yr old) -Painful swollen elbow. -X-ray: May look normal in very young children. -Rx: Like supracondylar fx.
Fx of the neck of radius Mech. of injury & pathology: Fall on the outstretched hand forcing the elbow into valgus & pushing the radial head against the capitulum. Fx through the neck of radius compared to the head in adults. Children: neck (N: N) Adult: Head (D: D) Clinical features: Sign of fracture with Pain on rotating the forearm.
Management -less than 30°radial head tilt & upto 3 mm of transverse displacement are acceptable. Casting for 2 -3 weeks then ROM -If >30° reduction either closed or open, internal fixation is not necessary. After operation 90°splintage in flexion for 2 -3 weeks then ROM
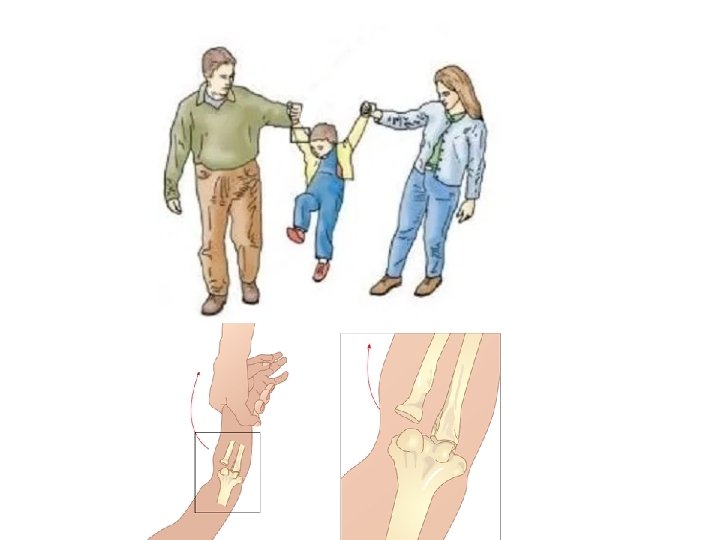
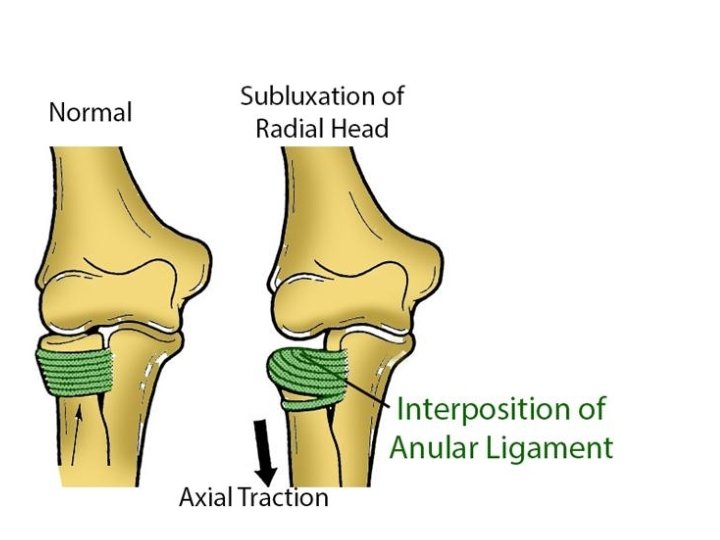
Pulled elbow -Due to pulling on the arm with the forearm extended and pronated. -subluxation of the radial head, but in fact it’s a subluxation of the orbicular ( annular) ligament Clinical features: -Painful arm and irritable child -Hx of the child being hold from the arm & crying -The forearm is held in pronation & extension. -No X-ray changed. Management: supination and hyper- flexion of the elbow
Distal forearm fx � The Most Common sites of childhood fx. �Fracture of radius or both radius and ulna �Rarely Ulna alone �Fall on outstretched hand. �Usually dorsal displacement �Usually metaphyseal fracture
• ttt: • Physeal fx (Salter Harris): Closed or open reduction and casting +- wire fixation • Buckle fx: casting for 2 -3 weeks, no reduction needed • Green stick fx: Closed or open reduction and casting +- wire fixation • Plastic deformation: manipulation , if not successful the open surgery to cut the bone and correct the alignment • Complete fx: Closed or open reduction and casting +- wire fixation
Physis fracture
Buckle , Greenstick , , , plastic defo 1/21/2022 42
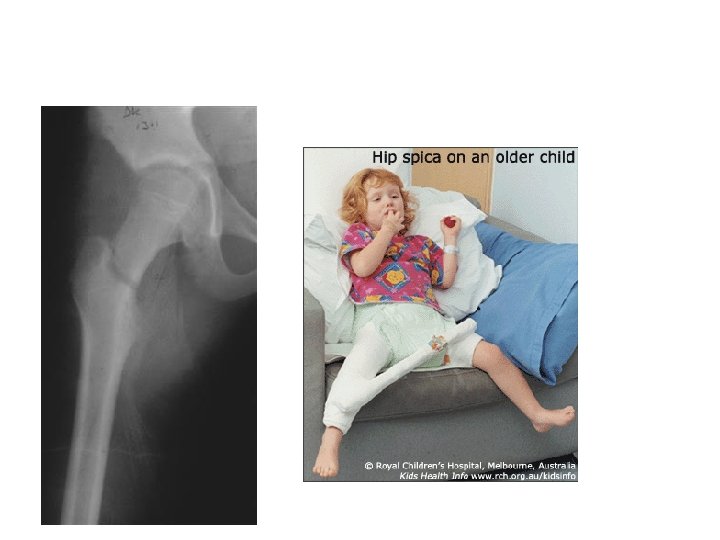
Hip fracture � Rare but serious � trauma that causes hip fracture in children is high energy trauma (RTA or Falling from Hight) �Always role out other associated injuries �If the trauma is not significant then Role out pathological fracture �Can Be: Head, Neck , inter-trochanter or sub trochanter �The fracture pattern may disrupt the blood supply of the proximal femoral head. Like adults? ? AVN �Head and neck are worse than inter-troch and sub-troch �Management: closed reduction and hip spica +- fixation �Avoid injury to the proximal femoral physis when fixing.