Common Musculoskeletal MSK Presentations in Primary Care Dr
 Presentations in Primary Care. Dr Neil Langridge MSc MMACP Consultant Physiotherapist")




 MRI -")































- Slides: 40
Common Musculoskeletal (MSK) Presentations in Primary Care. Dr Neil Langridge MSc MMACP Consultant Physiotherapist
Aims. • To introduce the most common MSK conditions seen in primary care. • To introduce the common signs/symptoms of these conditions. • To introduce the relevancy of physical testing. • To introduce the relevance of investigations.
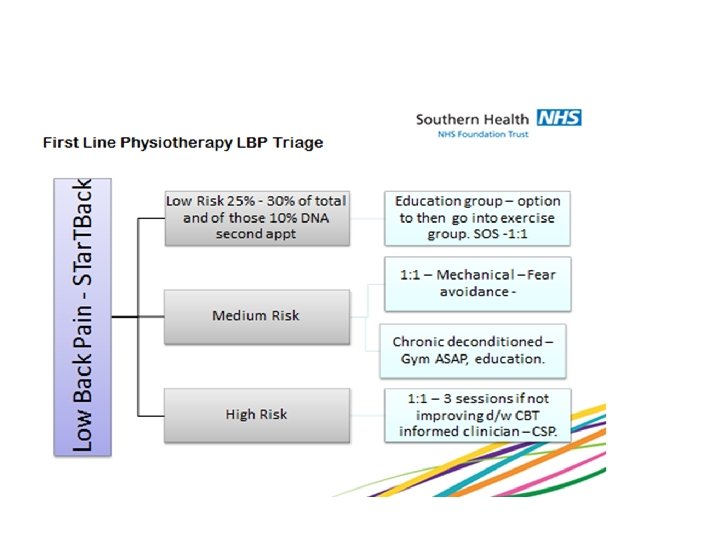
Low back pain • Common benign condition. • 85% Mechanical • 5%-15% Associated with radiculopathy (Sciatica) • < 5% serious
The most challenging patient!
What are the key features of disability in LBP? History • • Depression Poor sleep Anxiety Catastrophizing Maladaption Previous LBP Work/social issues assoc with LBP Clinical Exam • • • Widespread hyperalgesia Non-mechanical features Allodynia Dysaesthesia Latent response
Use of imaging for LBP X- ray – unhelpful (unless ? Fracture) MRI - Unless ? Serious pathology CT – For Surgical opinions (or non-MRI) Early use of MRI increases chances of disability, reduces a return to work and increases chances of surgery. • Surgery for LBP – outcome no different than rehab • •
What are the key red flags? • • • History of Ca – Breast, prostate, Lung Severe night pain New onset LBP over 55 Young spine CES – poorly interpreted. Weight loss, night sweats, constant
Useful Tests • • • Observation – deformity ROM Clear the HIP Neurological testing Palpation
Management Advice to stay active. Simple analgesia – taken regularly. Try to remain at work. No need to seek medical support unless increased analgesia needed. • Use STar. TBack to inform. • •
Sciatica • Leg pain – generally below the knee, with potentially Pins and Needles/Numbness. • Average time – 6 -8 weeks • Highly disabling • Can be recurrent • Most treated conservatively
• Leg pain worse than back pain – in many cases no LBP • Not always dermatomal • Cross over sign • Slump if SLR less reactive
Imaging for sciatica • MRI helpful • Worsening neurological compromise • Severe leg pain at 6 weeks.
Management • Analgesics • Neuropathic mediators if after 2 weeks symptoms unchanging and sleep is disturbed • Seek investigation with motor loss/worsening leg pain • Injections/surgery
The Neck • • Whiplash Referred pain Neurological compromise Myelopathy
Myelopathy • • • UMN tests Babinski Hoffmans Roos Hyper-reflexia If suspect – needs specialist assessment
Whiplash • • • Advice Gentle exercise Appropriate pain medication Clear any neurological loss Physio is helpful Can take many months to resolve
Radicular pain • • As per sciatica Tends to resolve Injections are risky Do well with neuropathic medication
Management • • Physiotherapy Analgesia Injections Surgery
• Age • Pain, stiffness and crepitus • Observation • Loss of range of motion – active & passive • +/- cuff weakness • Xray
Frozen Shoulder • • • Age: Normally >45 yrs Typical onset – pain & stiffness Natural history -9/12 to 2 yrs + Loss of active & passive ROM No true loss of power Normal X-ray
Management • • Physiotherapy – in some cases It has a natural history Injections for night pain V rare need surgery
Rotator Cuff • Age and vascularity of the tendon • Natural history –Repetitive movement of the arm • Presentation • Management options
Impingement • Loss of ROM • Painful arc • No massive loss of External Rotation • Passive Rom improves • • • Rest/NSAIDs Physiotherapy Time X-ray Injection Refer
Knee • • OA Trauma – soft tissue Degenerative meniscal Patella-femoral
OA knee
Management • • • Physiotherapy – lifestyle Weight loss Exercise – therapies Injections If all fails - surgery
Patella-femoral • • • Young Tends to affect females more than males Worse up and down stairs Pain at front of knee No obvious swelling
Soft tissue • Locked knee – immediate referral • Trauma – 2 weeks if not improving RICEM – needs assessment • Degenerative meniscal after 50 • Tendonitis/bursitis
Hip • • OA Bursitis Labral Tear Dysplasia
OA • • • Groin Buttock Anterior thigh pain – referral pattern Loss of rotation Putting shoes on/etc
Bursitis • Lateral or posterior thigh pain • Biomechanical • Worse at night and after sitting • Rest, ICE etc • Can be injected
• • Labral Tear Catching/after actvity Younger/sporting FABER/FADIR/Scoop • Modify activity • X-ray – Cam/Pincer lesion/impingement • Ortho Consultant opinion
Elbow • • • Tennis/golfers elbow Natural resolution in most cases Inflammatory/chronic tendon changes Physio/relative rest Injections Surgery
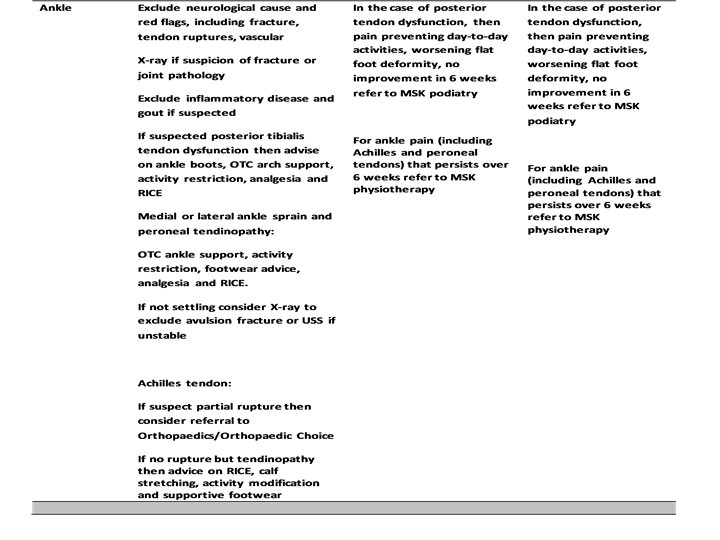
Foot/Ankle • Sprain – lateral • Plantar Fascia • Hallux valgus
Inversion injuries This patient decided to play on for 30 minutes after serious tendon injury!
• Thank you for your attention.