COMMON INJURIES AROUND THE HIP BY ALI IBRAHIMMD

COMMON INJURIES AROUND THE HIP BY ALI IBRAHIM<MD

COMMON INJURIES AROUND THE HIP

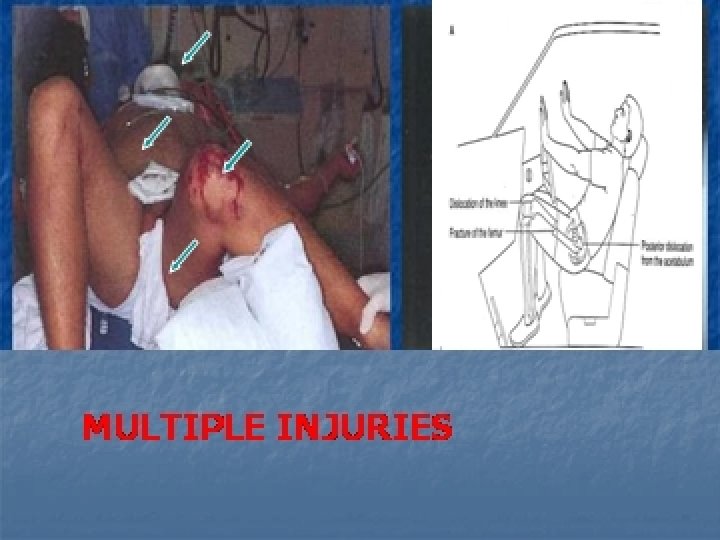
Fracture and dislocation • Fractures of the femoral side • trochanteric area • Neck femur • Femoral head • Fractures of pelvic side (acetabulum) • Fracture dislocation • Dislocations : posterior (most common) • anterior • Central

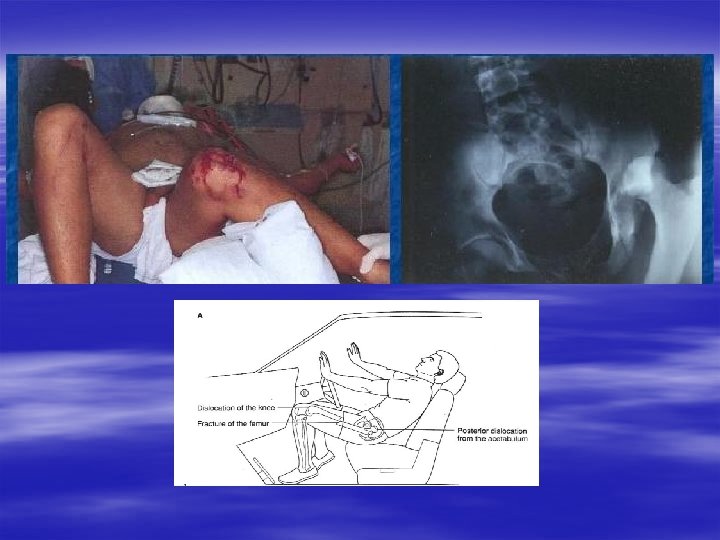
TRAUMA Direct Indirect § § Vehicular accedents Fall from height Crushing accidents Avulsion fractures DASH BOARD INJURY

FRACTURES OF THE PROXIMAL FEMUR

Fractures around the hip 250. 000 hip fractures/year 90% in patients >50 ys old Mortality related to hip fracture – 25% at one year 80% of patients recover their walking ability, Only 70% recover their ability to perform ADLs (activities of daily living)

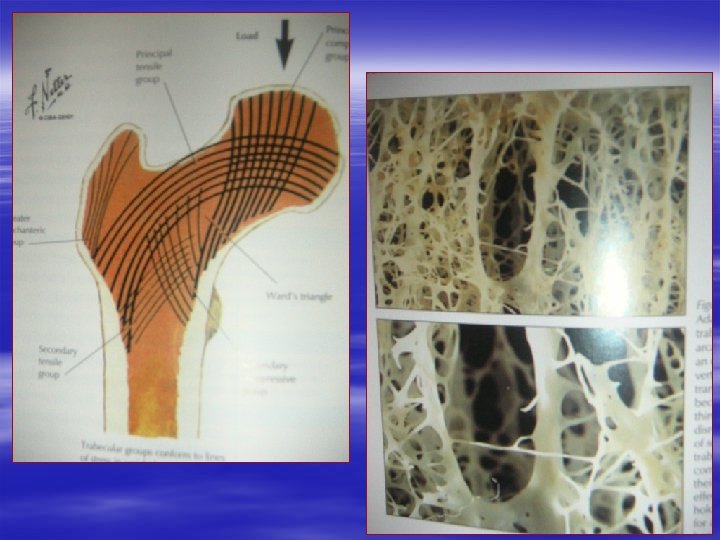
Risk Factors Age: incidence doubles for each decade after 50 ys Sex: 2 -3 times higher in women Race 2 -3 times higher in white women than in nonwhite women Habits Excessive alcohol or caffeine Physical inactivity Low body weight Previous hip fracture Dementia Psychotropic meds Visual impairment Osteoporosis

Hip Fractures § Femoral neck 45% – intracapsular, – disruption of blood supply to femoral head, – high incidence of healing complications (nonunion, osteonecrosis) § Intertrochanteric 45% – extracapsular, – no interference with the blood supply of the femoral head, – less complications – Malunion § Subtrochanteric – extracapsular – Malunion – Blood loss

Femoral Neck fracture

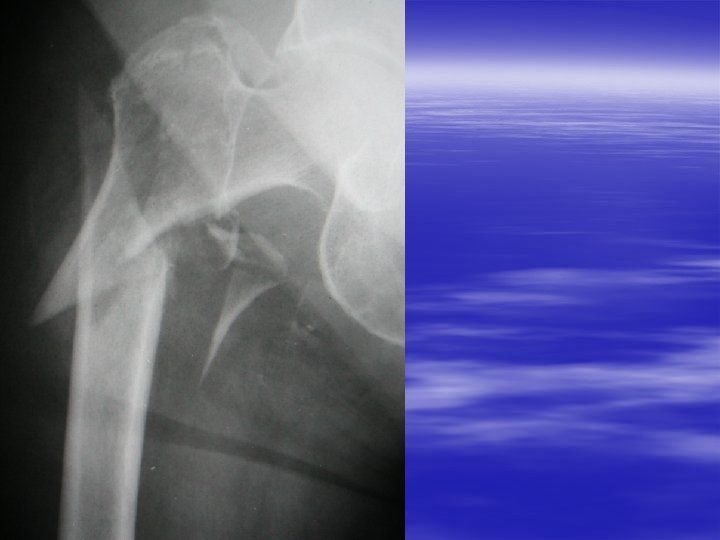
Trochanteric fracture

Subtrochanteric fracture

Clinical Assessment History: H/o fall – in a small percentage it occurs spontaneously C/o pain and inability to move the hip. Inability to put weight H/o other osteoporotic fractures: Colles or vertebral fractures

Clinical Assessment Physical Exam Complete exam: 69% of pts have major associated injuries – neck, head, other extremities, pelvis VS: look for signs of shock – blood loss in hip fractures can be up to 1500 cc Look for deformity, hematoma, asymmetry,

Clinical Assessment Physical Exam State of shock ? Leg externally rotated, shortened - severe in intertrochanteric fractures -moderate in fracture of the neck ROM limited and painful Crepitus at injured area • Inability to lift the extended leg Check the pelvis - Move posterior to anterior at the level of iliac crests Lateral to medial through the iliac crests

CLINICAL PICTURE SYMPTOMS: History of trauma, Pain, Swelling, Limited movements. SIGNS LOCAL: Swelling, Ecchymosis, Tenderness, Limited movements Deformity, Length discrepancy, Abnormal movements, Crepitus EXTERNAL ROTATION INABILITY TO LIFT EXTENDED LEG

Clinical findings • History of trauma • Pain • Loss of active movment • Abnormal movment • Painful passive movment • Crepitus at injured area • Deformity of the limb: • external rotation ; severe in intertrochanteric moderate in fracture of the neck fractures and • Flexion, abduction, external rotation in anterior dislocation • Flexion, adduction, internal rotation in posterior dislocation

Diagnostic Imaging § Xray: – AP and lateral. – Check the neck shaft angle 120 -130°. – No results but fracture still suspected: AP rotated 1012° - best visualization of femoral neck § MRI – most sensitive – order if Xray negative but fracture still suspected § Bone scan: sensitive, but has many interferences with the degenerative changes



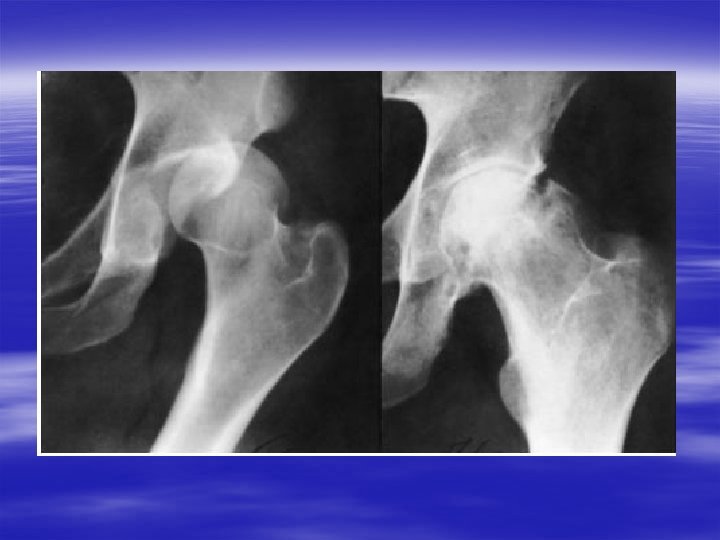
PATHOLOGICAL FR.

treatment Coservative tractoin: skin traction skeletal traction Operative reduction and internal fixation arthroplasty : Hemiarthroplasty total arthroplasty

Treatment Principles § Early surgery / 24 -48 h in patients who are medically stable § May wait up to 72 h to stabilize COPD, acute infections, decompensated CHF, § Assess cardiac risk § Delay in surgery/prolonged bed rest means: – increased risk of DVT, UTI, pulmonary complications, skin breakdown, – delayed functional recovery

Treatment Principles – DVT Prophylaxis Fatal PE in 4 -7% of patients undergoing hip surgery, Risk of bleeding 3. 5% compared to 2. 9% without anticoagulation Discuss anticoagulation with the orthopaedics specialist Heparin 5000 U q 12 h or LMWH upon admission

Treatment Principles – DVT Prophylaxis Warfarin on admission with target INR 23, if unable/unwilling to take heparin If anticoagulation is contraindicated – aspirin Pneumatic compression additional to heparin, warfarin or aspirin Continue prophylaxis until patient is fully ambulatory

TREATMENT OF CLOCED FRACTURES UNDISPLACED REDUCIBLE CONSERVATIVE TREATMENT 1 -TRACTION SKELETAL TRACTION

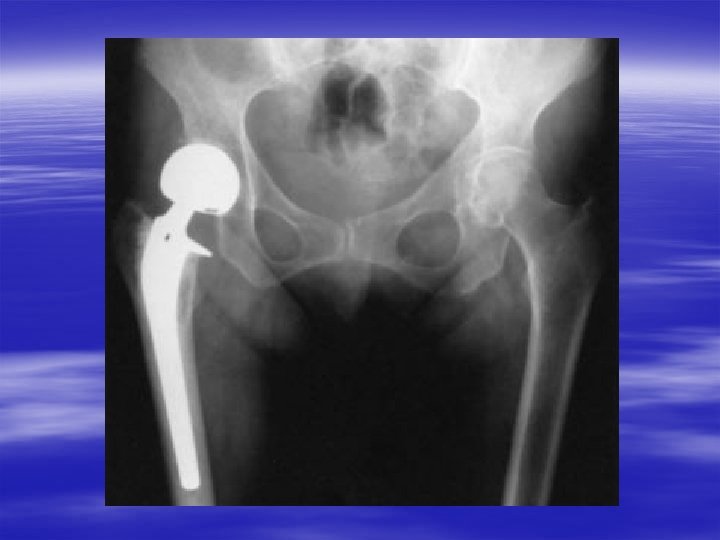
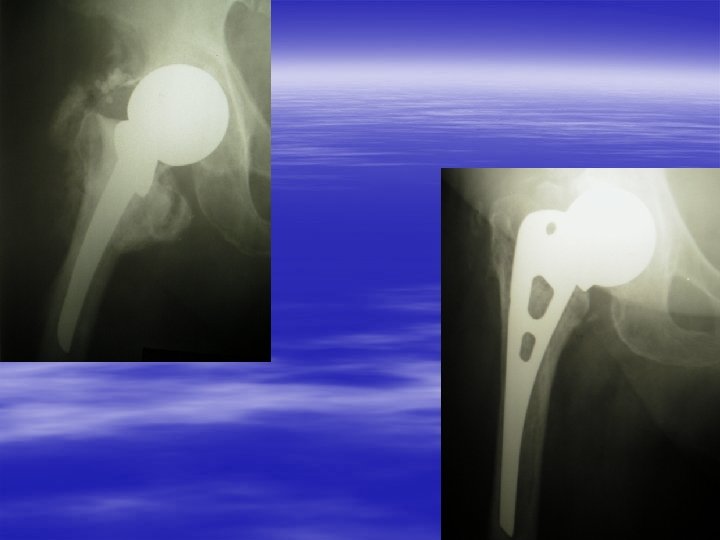
Prosthetic replacement Displaced Femoral neck Fracture esp. in elderly pt. HEMIARTHROPLASTY TOTAL ARTHROPLASTY

Prosthetic replacement: HIP PROSTHESIS TOTAL ARTHROPLASTY HEMIARTHROPLASTY

INTER TROCHANTERIC FRACTURE DHS

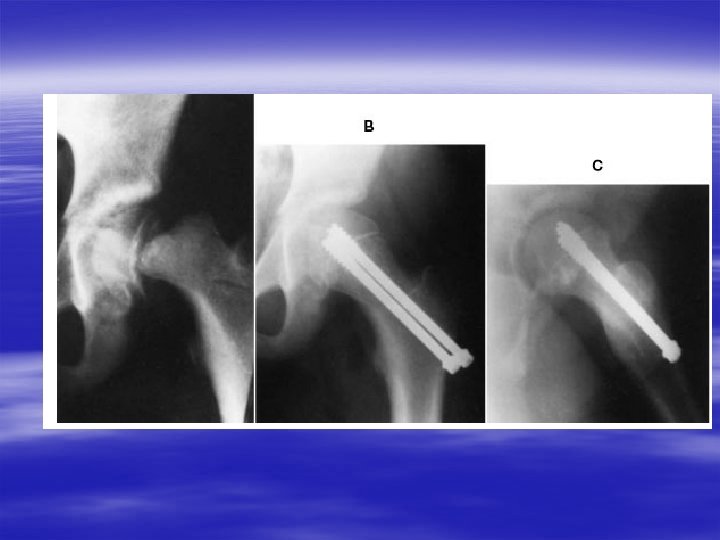
Types of Surgery Minimally displaced femoral neck fracture Internal fixation with multiple screws
")
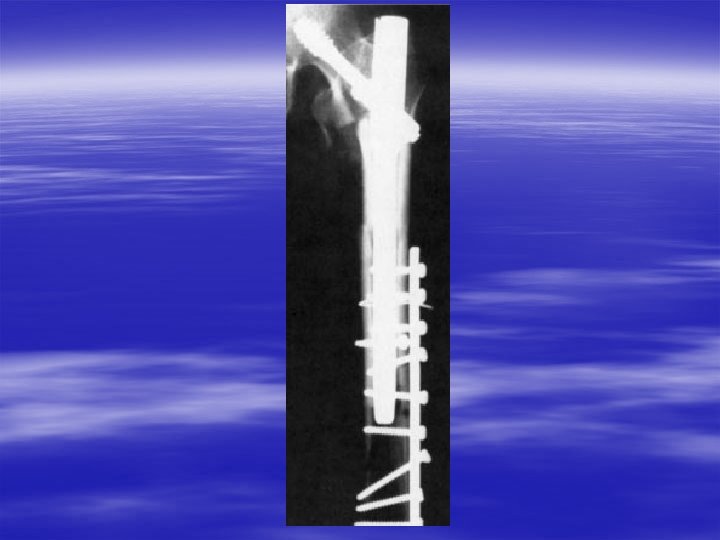
Types of Surgery Intertrochanteric fracture Internal fixation with dynamic hip screw(DHS)

Types of Surgery Displaced Femoral neck Fracture Prosthetic replacement


Types of Surgery Intertrochanteric fracture Internal fixation with sliding hip screw




Post-operative Care Nutrition: oral protein supplementation a/w with shorter hospital stay Foley - for 24 h only, - early removal is a/w less retention, earlier spontaneous voiding, less UTI Total hip precautions: - No adduction past midline – use abduction pillows, - No hip flexion beyond 90° (tall comode, no bending >90 ° - No internal rotation – keep toes upright in bed

complications • Non union of the fractures in femoral neck fr • Malunion of the fractures in trochanteric, subtrochanteric fr • AVN of the femoral head • Degenerative changes of the hip joint • DVT, complications of long recumbancy • Neurovascular injuries

Coxa vara Neck shaft angle

COMPLICATIONS Loss of fixation – 15%of patients: internal fixation for displaced fractures Nonunion/osteonecrosis – mo/years after SX in internal fixation for displaced fractures Dislocation of the prosthesis – early, related to infections Loosening of prosthesis – years after Sx Infections – 5% cases DVT, PE Delirium

Rehabilitation § Goal – independent living § Rehabilitation should begin first day after surgery with transfer from bed to chair § Progress as soon as possible to standing and walking (2 nd day post op) § Promote weight bearing with assistance – walker

Hip Dislocation POSTERIOR · 80% of hip dislocations · Limb internally rotated and adducted · Neutral/adduction at time of injury - simple dislocation only · Abduction at time of injury - fracture posterior acetabular wall Complications · Associated knee ligament injuries especially PCL, posterolateral complex · Sciatic nerve injury 10 -14% · Superior gluteal artery injury

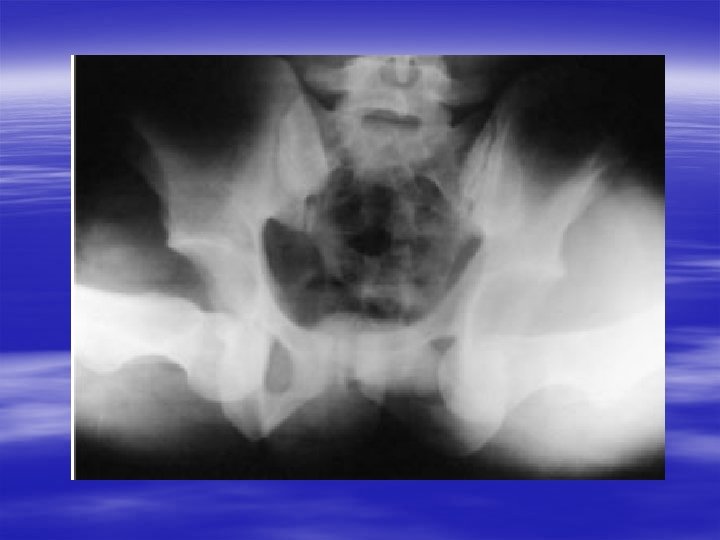
ANTERIOR DISLOCATION HIP

Clinical findings • History of trauma • Pain • Loss of active movment • Painful passive movment • Crepitus at injured area if + fr • Deformity of the limb: • Flexion, abduction, external rotation in anterior dislocation • Flexion, adduction, internal rotation in posterior dislocation LOOK FOR EVIDENCE OF NEURO-VASCULAR INJURY

treatment Coservative : Closed Reduction under G. A & muscle relaxant then tractoin: skin traction skeletal traction Operative reduction and internal fixation of acetabular fr arthroplasty : total arthroplasty

complications • Neurovascular injuries • DVT • AVN of the femoral head • Entrapped intra-articular fragment • Missing an injury • Myositis ossificans • Degenerative changes of the hip joint

THANK YOU
- Slides: 57