Coming of Age as Communicators Implementation of Common

















 Internal Medicine (n=31) Obstetrics and Gynecology")
 in 4 disciplines n To")





 Context Input Process Product")

















- Slides: 43
Coming of Age as Communicators: Implementation of Common Training in 4 Residency Programs Saleem Razack MD FRCPC, Associate Professor, Pediatrics, Member, Centre for Medical Education, Mc. Gill University Medical Education Rounds, February 23, 2006
Educational Objectives: n n To understand the rationale for the explicit teaching of communication skills in residency training (Why? ) To describe the evaluation of a program in which common content communication skills training was adapted to 4 residency level disciplines (What we did? ) n To consider shared training initiatives for other core competencies (How? )
The Can. MEDS Communicator Role: Definition: As Communicators, physicians effectively facilitate the doctor-patient relationship and the dynamic exchanges that occur before, during, and after the medical encounter --Can. MEDS 2005 (© RCPSC)
Communication as a Core Clinical Skill n n n Medical interview is most commonly performed procedure in medicine In surgical specialties 75% of clinical time is spent communicating with patients (Rotor et al. ) The physician performs at least 200, 000 interviews in a 40 year career
Communication Skills—Patient Benefits n Effective interpersonal and communication skills are associated with: n n Greater symptom improvement and resolution Greater patient adherence to therapy Better management of chronic conditions Greater patient satisfaction with care
Communication Skills—Physician Benefits n n The physician-patient relationship is the most consistently reported determinant of physician satisfaction Residents at the end of their training report that their relationships with patients are “healing”
Communication Skills—Mutual Benefits to the Patient and Physician n Physicians who focus on the patient as a person-n n Obtain more timely reports from patients of important symptoms Obtain more adequate histories
Ineffective Communication: n Ineffective communication in clinical encounters is associated with: n n More malpractice suits and claims Medication errors
Summary of Evidence-Based Communications Practice The Medical literature supports: n n n greater patient-satisfaction with care 1 greater symptom improvement 1 decreased medication errors 1 improved patient adherence to therapy 1 better management of chronic conditions 2 decreased malpractice suits 3 1: Stewart MA: CMAJ 1995, 152: 1423 -33 2: Kaplan SH, Greenfield S, Wai JE: Med Care 1989 275: 5110 -27 3: Levison W: JAMA 1994, 272 (20)
Teaching Communication Skills: Communication Theory 101 n 3 Broad Approaches, each with pros/cons/and applicability n n n Attitudes Related Approach (Encourages Empathy) Issues Related Approach (Gives Issue Specific Vocabulary) Skills/Behaviour Related Approach (Provides Logistics)
Skills/Behaviour Related Approach n Premise: n n n Pros: n n Effective Communication: a series of learned skills Requires practice, reflection, and feedback Skills/Behaviours can be taught, observed, and evaluated Cons: n Attitudes and values guiding behaviours should be made explicit
Training Frameworks: n n Many Frameworks for effective communication exist in the literature All share ideas of: n n relationship building understanding patient perspective information exchange (I. e. 2 way vs. 1 way) consensus and agreement (collaborative vs. directive)
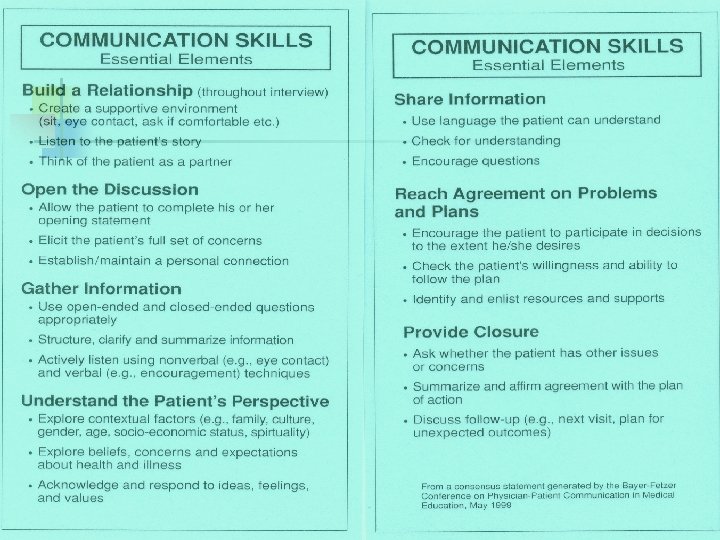
The Kalamazoo Consensus Statement: n n n Derived from expert consultation of medical educators across North America (Bayer-Fetzer Institute Working Group on Physician-Patient Communication in Medical Education) Broad Based Consensus (21 North American Leaders in the field) Coherent set of essential elements (Skills and Behaviours) in physician-patient communication
What Are We Really Teaching? n Core Skills: n n Effective Listening & Observation Respectful Engagement Self-Awareness and Reflection Core Values: n n Shared Decision Making Information Transfer goes two ways
Important External Stimulus: Can. MEDS and Accreditation Scholar Communicator Collaborator Medical Expert Advocate Manager Professional
The Needs that Suggested an Educational Research Project Multiple Programs wanted to incorporate training in communications skills n Many programs lacked local “experts” Questions: 1. How can we take the common content in communication skills training and adapt it effectively to different training environments? 2. What would make it work? n
Effective Sharing of Expertise in Teaching the Physician’s Communicator Role: Evaluation of the Implementation of Communication Skills Training in 4 Residency Programs Saleem Razack, Sarkis Meterissian, Lucie Morin, Linda Snell, Yvonne Steinert, Diana Tabatabai, Anne-Marie Mac. Lellan
The Four Programs n n General Surgery (n=18) Internal Medicine (n=31) Obstetrics and Gynecology (n=20) Pediatrics (n=11)
Objectives: To implement common content communication skills training (CST) in 4 disciplines n To describe thematic similarities and differences as the common material is adapted in each context Overall goal: identify context specific factors to consider for successful shared training initiatives n
Hypothesis: n 4 distinct pedagogic and practice “subcultures” n n Describe and categorize similarities and differences Learn how context may be used for more effective shared training initiatives
Applying “Culture” to Residency Training Definitions of Culture: n A system of meaning shared by a group of people, passed on from one generation to the next n Includes beliefs, traditions, values, customs, communication styles, behaviours, practices, and institutions (Other terms: Hidden Curriculum, Implicit Curriculum, Ethos)
Methodology: n n Educational intervention Learning outcomes Session transcript/field note analysis Session transcript quantitative analysis
Educational Intervention: n n n Content: Kalamazoo Consensus Statement 45 -Minute Plenary 1 Hr. 15 minutes: Break-out groups n n Role Plays Reflection on own context Facilitator Training Learning outcomes measured by retrospective-post questionnaire
Transcript/Field Note Analysis n n Trained observer Field notes and audio recordings Grounded ethnographic approach (Qualitative) Transcript word counts (quantitative)
Program Evaluation Paradigm: n CIPP methodology (Shufflebeam et al. 1974) Context Input Process Product
Context: n n n Location and Timing Motivation for training Milieu or discipline-specific factors
Input: n n n Proposed participants Proposed facilitators Content adaptations Baseline skill level Values and attitudes towards CST
Process: n n Outside or within-discipline presenter Modalities used The learning process during small groups (continuum: skill acquisition to reflective practice) Locus of participation
Product: n n Ideal product of training (e. g. good communicator of good teacher of communication skills) Specific knowledge, skills, and attitudes that programs want to promote
Learning Outcomes: Retrospective Pre-Post Data All Results Significant, with P<0. 05 Q 1. My ability to articulate the essential elements of communication in clinical encounters using the Kalamazoo Model Q 2. My appreciation of communications skills as a set of skills that I can explicitly learn and practice Q 3. My ability to evaluate and effect positive change in my own communication effectiveness with patients Q 4. My ability to apply what I’ve learned here today to the teaching of more junior residents and students in my own context (Candidates rated the above statements on a 5 point Likert scale (1=strongly disagree; 5= strongly agree)
Results: Trans-discipline Role Play Grid
CIPP Program Evaluation: Program Analysis Domain Thematic Similarities: Thematic Differences Context Motivation to Develop Training: o Accreditation Standards of credentialing bodies Location: o Perceived “uniqueness” of communications skills training in curriculum (PED: Regular Academic ½ day session, IM: Special ½ day session, SURG: Special Academic ½ day, OBGYN: Residents’ Retreat) Delivery: o Use of within- specialty communications experts to deliver workshop perceived as very important in PEDS/IM for effective intervention; opposite true in OBGYN and SURG
CIPP Program Evaluation: Program Analysis Domain Thematic Similarities: Input Thematic Differences Barriers: o Residents in all disciplines identify the same barriers to effective communication in their practices Time Space Constraints Language and Culture Lack of formal training, observation and feedback), o Perceived as impacting negatively on the quality of care Value of Communications skills training: o Majority of residents in all disciplines perceive communications skills training as a positive step and are open to it Residents: o All years participated in PEDS, SURG, OBGYN; only 1 st years in IM Skill Level: o Peds/IM: Implicit emphasis on reflective practice (Higher level) o Surg/Ob-Gyn: Implicit emphasis on Skill/Behavior acquisition (More basic level) Workshop Facilitators: o Marked differences in comfort with facilitating small groups and role plays (IM/PEDS-generally comfortable; SURG-less experienced but comfortable; OBGYN-somewhat apprehensive of the process)
CIPP Program Evaluation: Program Analysis Domain Thematic Similarities: Thematic Differences Process Content: o Common core content, workshop format, and role play stems adapted to each discipline Facilitator Training: o done with all groups together Specific to SURG: o Concern over resident seniority hierarchy (i. e. putting senior residents “on the spot” in interactive small groups perceived as having a negative impact on group dynamics)
CIPP Program Evaluation: Program Analysis Domain Thematic Similarities: Thematic Differences Product Skill Level: o Despite different emphases (teaching role vs. core competence) all residents showed improvement in perception of change in skill level (retrospective pre-post testing) and showed progression of these with the progression of role plays Value of Training: o Majority in all disciplines appreciated intervention as beneficial (slightly less in SURG) PEDS/IM: o Emphasis on residents’ teaching role in communication skills for junior trainees SURG/OBGYN: o Emphasis on residents gaining a core competence for clinical practice
Locus of Participation Data: Facilitator Utterances Resident Total Utterances % of talk by residents OB-GYN 961 4775 5609 84% SURGERY 7544 4637 13221 35%* (Significant) MEDICINE 3195 3251 6446 50%
Discussion: What did we learn? n n n It is possible to take core content and successfully adapt it to different residency training contexts “Front-office/Back-office” analogy Positive learning outcomes demonstrated
“Cultural” Sensitivity in Pedagogy n n n Communication skills traditionally viewed as “soft” Learning of CST is a socio-cultural process, affected by behavioral norms and group values The hidden curriculum revealed, as the “pluripotent” graduate “differentiates” to a specific field of residency training?
Discipline-specific Values: n Different behavioral/value norms associated with each discipline: n n n E. g. Peds/IM—Emphasis on Teaching role vs. skill acquisition Differences in Reflective language vs. behavioral skills Caveat: Observations not meant to generate a discipline-specific “trait” list
Translating Sensitivity to “Culture” into Intervention Efficacy: n n n Many opportunities for shared training initiatives in non-medical expert core competencies Sensitivity to context may promote more successful initiatives We found the CIPP program evaluation tool useful in planning shared training initiatives
Provocative Speculation: n n By analyzing the implementation of communication skills training in 4 disciplines, we got a hint at the sociocultural process of developing group identity in specific disciplines Further study of this discipline-specific “hidden curriculum” may yield useful information in core competency training
Thank You for your Attention!