Combitube Training Mandatory training every 2 years for

Combitube Training Mandatory training every 2 years for all BLS Providers Verde Valley Emergency Medical Services


Topics § Airway and Respiratory Anatomy and Physiology § Basic Airway Management § Combi-Tube Airway Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Introduction § The importance of establishing and maintaining an airway in the patient can never be overstated. § Despite the majority of patients’ responding favorably to manual and/or simple mechanical adjuncts, some may need more advanced airway procedures. § It is for this reason that advanced airway skills are now included as an elective in the EMT-B curriculum. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Upper airway § Opening of the nose and mouth to the larynx § Includes the nasopharynx, oropharynx, and hypopharynx – Lower airway § Lower portion of the larynx § Trachea § Bronchi Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Nose § § § Warms the air. Provides humidification. Coarse hairs serve as an initial filter for inhaled air. – Mouth § Also a conduit for airflow. § Oropharynx contains special reflexes to guard the airway. – Pharynx § Conducts airflow, and gives rise to the openings of the lower airway and the esophagus. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Larynx § § Lies inferior to the pharynx and superior to the trachea Directs air from pharynx to trachea Houses the vocal cords Comprised of three cartilaginous structures – Thyroid cartilage is the large shield shaped structure. – Cricoid cartilage is the first compete cartilaginous ring that is attached to the trachea (inferior aspect of larynx). – Epiglottis is the leaf shaped structure that covers the larynx during swallowing. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Larynx § The vallecula is a depression located between the base of the tongue and the anterior surface of the epiglottis. § The glossoepiglottic ligament which suspends and supports the epiglottis is located at the center of the vallecula. § These structures are important as they are sometimes manipulated during advanced airway procedures to lift the epiglottis (making it possible to visualize the glottic opening). Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Larynx § View of the laryngeal structures which shows the vallecular space and glossoepiglottic ligament Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. insert fig 45 -1 Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Larynx § § § Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. True vocal cords False vocal cords Arytenoid cartilages Corniculate cartilages Cuneiform cartilages All of the above can be important visual landmarks during the intubation procedure. insert 45 -2 Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Larynx Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Trachea, Bronchi, and Bronchioles § Trachea is comprised of 16 -20 “C” shaped cartilage rings. § Rings are posteriorly incomplete as they share a common wall with the esophagus (trachealis muscle). § The trachea gives rise to two mainstem bronchi at about the level of the 5 th thoracic vertebrae. § The point of bifurcation is called the carina. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Trachea, Bronchi, and Bronchioles § The right mainstem bronchi is of a larger diameter with a lesser angle than the left (that has a sharper angle due to the position of the heart). – The lesser angle makes it easier to misdirect a tracheal tube into the right mainstream bronchus than into the left. – The lesser angle also accounts for the fact that aspiration of foods, liquids, or foreign bodies occurs more commonly in the right than in the left. § Finally, the bronchi continue to subdivide into smaller and smaller bronchioles until the alveolar sacs are reached. § The alveolar sacs are the sites of gas exchange for the pulmonary system. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy – Lungs § Right and left lungs § Separated by the mediastinum § Wrapped by the pleural linings Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Airway and Respiratory Anatomy and Physiology § Airway Anatomy in Infants and Children – Differences that are important to remember § Larger occipital region of the head. § Mouth, nose, and pharynx smaller, more pliable, and easier to obstruct. § Tongue is proportionally larger. § Larynx and trachea are funnel shaped, the cricoid ring the narrowest portion. § Trachea, since it is more flexible, can kink from excessive hyperextension of the head during airway procedures. § Chest wall more pliable, fails to adequately support ribs. § In concert, all these differences add up to a more difficult airway to manage under even the best circumstances. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Basic Airway Management § Often, the best situation to use advanced airway procedures is when you have a patient needing prolonged ventilation. § Beyond this, you will only use these skills when basic airway maneuvers fail to provide you an airway. § Remember, you should only use these skills when you need to; do not use them simply because you can. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

Basic Airway Management § As mentioned previously, the EMT-B will be able to establish a patent airway in the majority of the patients by just using the following skills: – Nasopharyngeal or oropharyngeal suctioning – Manual airway techniques (head-tilt chin-lift, and jawthrust) – Simple mechanical adjuncts (OPA/NPA) – Patient positioning and use of cricoid pressure (Sellick’s) § If, however, the above fails to work – or becomes ineffective – then the implementation of advanced airway skills becomes the only other option. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren
 – Dual Lumen Airway Devices")
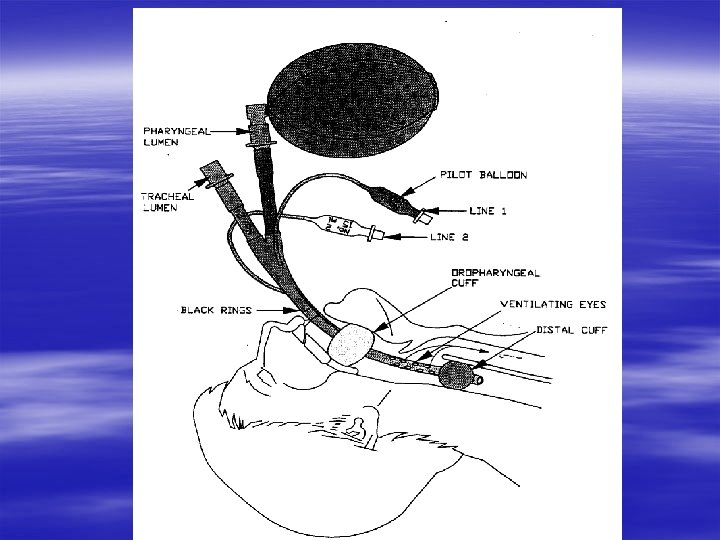
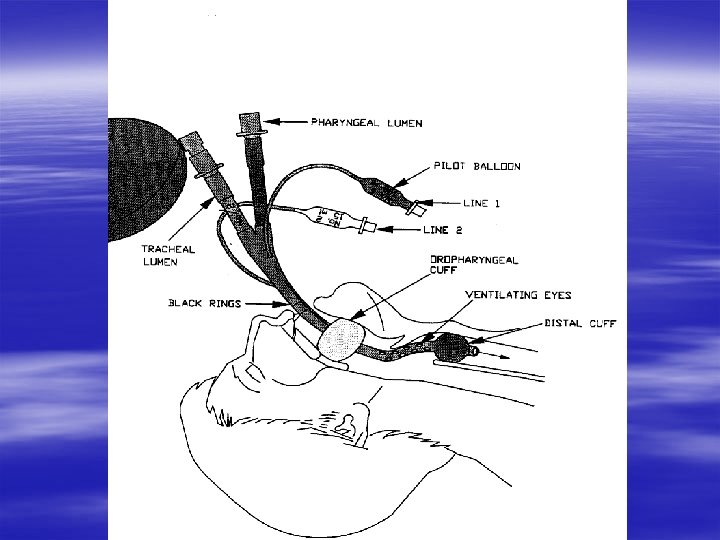
Combi-Tube § Esophageal Tracheal Double Lumen Airway Device (ETDLAD) – Dual Lumen Airway Devices § These airway devices are designed with dual lumens side-by -side, but of varying length. § The premise is that upon insertion and inflation of the appropriate cuffs, one of the tubes will result in lung inflation while the other winds up directing air into the esophagus. § The goal naturally is to use the lumen that ventilates the lungs, but the beauty of the device is that regardless of where the longer tube is positioned (either in the esophagus or in the trachea), successful ventilation can be achieved. Copyright 2004 Prentice Hall Publishing A division of Pearson Inc. Prehospital Emergency Care 7 e Mistovich/Hafen/Karren

The Combitube § An Esophageal Tracheal Double Lumen Airway

Combitube / Combitube SA § § SA = SMALL ADULT Small Adult = Less than 5 ft 6 inches tall Small Adult = Taller than 4 ft 0 inches Combitube SA can be used on small adults who are between 4 ft and 5 ft 6 inches tall.

Combitube / Combitube SA § Combitube is used for patients over 5 ft tall.
")
Black Lines Used for Proper Tube Insertion Depth. (Straddle upper teeth or gums)
")
Inflation Point Pilot Balloon for Large Pharyngeal Cuff Large Proximal Pharyngeal Cuff (#1)

Large Syringe Attached to Pilot Balloon #1 Ready to Inflate with 100 cc’s of Air
 Remains Inflated. Large Pharyngeal Cuff Inflated")
Pilot Balloon (#1) Remains Inflated. Large Pharyngeal Cuff Inflated
 Pilot Balloon for Esophageal Cuff (#2)")
Inflation Point Small Distal Esophageal Cuff (#2) Pilot Balloon for Esophageal Cuff (#2)

Small Syringe Attached to Pilot Balloon #2 Ready to Inflate with 15 cc’s of Air

Pilot Balloon #2 for Small Distal Esophageal Cuff #2 Remains Inflated Small Distal Esophageal Cuff #2 Inflated

2 Lumens allow for ventilation if the tube is inserted into the Esophagus (most common) or into the Tracheal Lumen (#2) Esophageal Lumen (#1)
")
Esophageal Lumen (#1)
")
Tracheal Lumen (#2)

Skills / Testing Stations § Basic airway maintenance techniques. – Equipment, techniques, oxygen, suction. § § Combitube familiarity. Combitube insertion & AED incorporation. Combitube tracheal and problem insertion. Written exam.
- Slides: 35