Combining nonspecific and adaptive immune response Bacterial infection

Combining non-specific and adaptive immune response Bacterial infection: At first: phagocytes, histamine release, inflammatory response Inflammation brings phagocytes, plasma proteins (complement system, clotting proteins) Bacteria antigen stimulates helper T cells, B cells get activated: antibodies Bacteria get labeled w/antibodies, killed by complement, macrophages, killer cells. This slide is just another way to organize things for immune response to help study. I won’t use in lecture

Combining non-specific and adaptive immune response Viral infection: Virus inside body cells do not trigger macrophages, B-cells, or complement. Virus-infected or cancerous cells release interferon, signaling neighboring cells and attracting natural killer cells, macrophages, complement. Virus ‘out in the open’ can be attacked. Antigen-self combination triggers T-helpers, which help stimulate killer T cells (takes days) and attract macrophages to the area. This slide is just another way to organize things for immune response to help study. I won’t use in lecture

Anaphylactic shock Systemic anaphylaxis- when large amounts of histamine and inflammatory signals are released all at once to blood. Widespread dilation - hypotension. Airway constriction. Victim can die within minutes. due to penicillin, bee venom. Often

Does the immune system react differently for different allergies? Skin: Besides Ig. E response, can be a T-cell response to substance (ex: urushiol oil) Airway: besides histamine, leukotrienes are released – airway constricted Gut: traditional food allergies are Ig. E (egg, milk, wheat, nuts, shellfish, etc. ) Histamine dilation, leukotriene constriction. Some are T-cell allergies w/delayed effects (gluten, milk).

What do allergy medications do beside reduce inflammation? They generally reduce the histamine signal They can be bronchodilators, reduce leukotrienes, decongestants (constrict capillaries), injectable epinephrine, anti Ig. E Corticosteroids inhibit expression of cytokines and other signals of inflammation

Development of ‘tolerance’ Tolerance of substances develops early via clonal deletion of specific lymphocytes Central tolerance: B and T cells that respond to self-antigen are destroyed Error can result in autoimmune disease Peripheral tolerance: regulatory cells inhibit response to environmental antigens Error can result in allergies Allergies can have late onset, even in adulthood

Hygiene hypothesis Keeping a child’s environment ‘too clean’ may prevent proper development of immune system Recent study: Exposing ‘high-risk’ infants to peanuts reduced later allergies by 80%

What are autoimmune diseases? Immune system wrongly attacks body cells, often caused by production of autoantibodies Rheumatoid arthritis – autoantibodies attach to joints and induce inflammation & attack by complement, and WBCs

A few immune related disorders: Diabetes Type I Crohn’s Disease Multiple Sclerosis Pernicious anemia Addison’s disease Lupus

Why do autoimmune diseases begin? AI diseases often have an environmental trigger, those with certain genotypes can be more susceptible to it A trigger can be an infection w/antigen that is molecularly similar to markers on body cells Possible environmental agents: silica, mercury, nitrates in drinking water, groundwater pollutants, drugs, many other chemicals…

Question: Lupus A problem with apoptosis causes formation of autoantibodies Apoptotic cells aren’t removed normally, they instead degrade, proteins left are engulfed by cells that present antigen. Autoantibodies created against these proteins.

How can I boost my immune system? Vitamin D – helps trigger T cell response Zinc – if early in infection Sleep Diet Exercise

Respiratory system External vs. cellular respiration

Respiratory system Airway: from nasal passages down to trachea, bronchioles and alveoli. The trachea and bronchi are reinforced with cartilage Larynx (voicebox) has vocal cords Bronchioles can dilate and constrict

Respiratory system Smooth muscle bronchioles Pulmonary capillaries Alveolus

chest cavity

Lung wall l al w t s C ty he l Pl ra u e vi a c Lungs Transmural pressure gradient lungs will always expand to fill pleural cavity

Increasing cavity volume, air enters If lung pressure is less than atmospheric pressure, air enters the lungs.

Inspiration and expiration: how we change chest volume

Pneumothorax: How a lung can ‘collapse’ Puncture wound in chest wall 760 756 760 760

What determines airflow? F= P same equation as blood flow! R Major determinant of resistance is radius of bronchioles Disease can increase resistance (asthma, bronchitis)

Surface tension at alveoli Surface tension – whenever water layer meets air – water molecules are attracted to each other. Surface tension along the lining of alveoli resists expansion of alveoli. Surfactant reduces surface tension.

Gas exchange and partial pressure gradients Air is a mixture of gases Nitrogen is 79% of air. Its partial pressure: 0. 79 x 760 = 600. 4 PO 2 PCO 2 Alveoli 100 40 Capillaries 40 46

Hemoglobin saturation Most O 2 is carried by Hb Oxygen saturation curve some is dissolved in plasma and determines partial pressure Hb saturation is high where PO 2 is high (lungs). Saturation remains high even PO 2 is 60 Small decrease in PO 2 makes Hb unload much more O 2

Shifting the curve Increase in CO 2 from tissue shifts the saturation curve to the right Increased acidity (H+, carbonic acid) and temperature has the same effect - Bohr effect

Most O 2 carried on hemoglobin A teensy bit of O 2 is dissolved in plasma

Chemoreceptors sense O 2 dissolved in blood Carotid and aortic bodies send info to the medulla PO 2 and PCO 2 and H+ can be detected O 2 saturation is not detected

Spirometry Measures airflow and volume of inspiration and expiration

Urinary system Aids homeostasis by removing cellular wastes and foreign compounds, and maintains salt and water balance of plasma

Kidney anatomy Renal cortex Renal medulla Cortex Renal pelvis Ureter Medulla

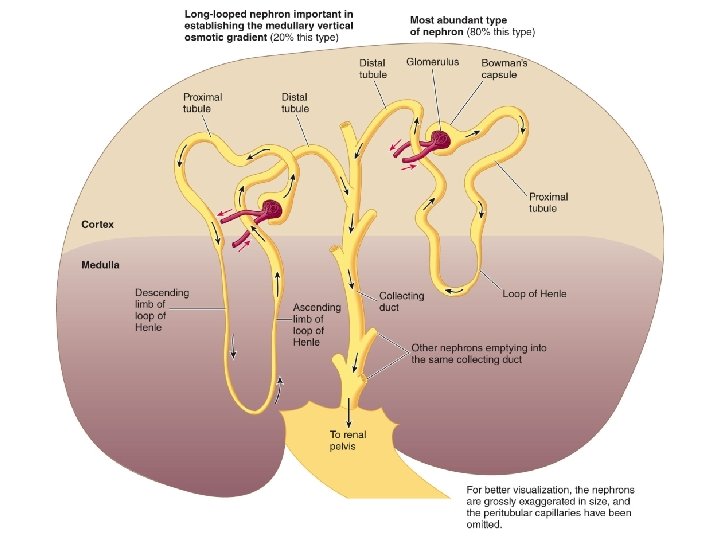
Nephrons Each kidney has about one million nephrons Afferent arteriole brings blood to glomerulus and then forms efferent arteriole. Efferent arteriole branches to peritubular capillaries

Let’s make the filtrate. . . Blood is filtered at the glomerulus. Water and solutes leave the blood and enter Bowman’s capsule.

Glomerulus physiology Bowman’s capsule contains podocytes that encircle the glomerulus. Normally blood cells and plasma proteins are not filtered.

Glomerular filtration is similar to ultrafiltration of capillaries 20% of plasma becomes filtrate Osmotic pressure 55 30 Capillary blood pressure 15 Hydrostatic pressure Glomerular filtration rate (GFR) determined by: Net filtration pressure and glomerulus permeability

Adjusting GFR Blood pressure Radius of afferent arteriole Decreasing GFR helps retain fluid and salts

Filtrate is adjusted along the nephron Proximal tubule Distal tubule Cortex region Bowman’s capsule Juxtaglomerular apparatus - helps in adjustments to filtration rate Loop of Henle Medulla region

Tubular reabsorption and secretion 180 liters per day are filtered, most is reabsorbed Reabsorption: filtered substances leave the nephron and enter peritubular capillaries Secretion: some substances from the peritubular capillaries enter the nephron

So what is urine, then? Everything in the nephron that does not get reabsorbed into the blood leaves as …. urine!!!

Reabsorption physiology
 + Na")
Reabsorption of (the key to it all…) + Na
 drives the movement of many other substances in the tubule Water")
Na+ reabsorption (RA) drives the movement of many other substances in the tubule Water will “follow” Na+ movement

Lumen Proximal tubular cell Interstitial fluid Figure 14. 22 Page 533 Osmosis Water channel Osmosis Hydrostatic pressure Peritubular capillary
- Slides: 43