Combatting Physician Burnout Evidence Summary 2017 Chris Simmons

Combatting Physician Burnout Evidence Summary 2017 Chris Simmons, MD, Ph. D 9. 29. 17

Burned out about burnout?

Objectives - Grasp the scope and impact of burnout - Investigate the driving factors behind physician burnout - Weigh evidence surrounding interventions to reduce or prevent burnout - Be inspired to equip yourselves for change

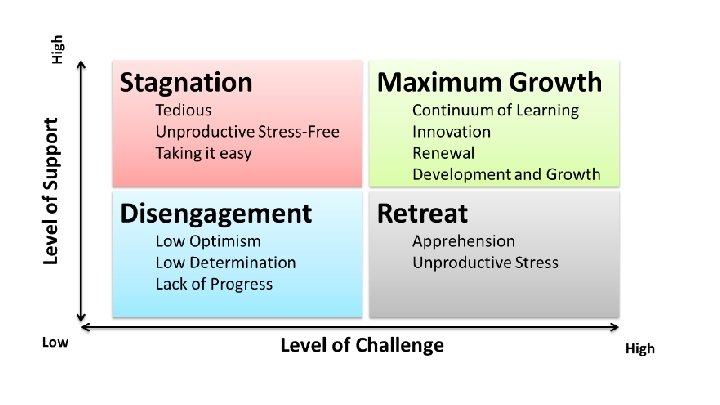
Burnout Once motivated individuals experience progressive work dissatisfaction due to both external and internal stimuli

Maslach Index 22 Question inventory At on point, cost $0. 50 per copy Now costs $2. 00 per copy. . . Maslach C, Jackson SE

Components of Burnout Emotional Exhaustion Depersonalization Lack of personal achievement

Scope of The Problem Regardless of profession, the American workforce is facing a burnout crisis ● $125 -190 billion annually in healthcare spending due to symptoms of burnout Garton E, Harvard Business Review 4. 6. 17

Scope of The Problem As few as 39% of physicians experience burnout with many estimates exceeding 50% Burnout directly attributed to losing 1. 2% of workforce between 2011 -2014 Shanafelt TD, Mayo Clin Proc, 2016

Scope of The Problem

Scope of The Problem Example for a large academic center: ● 450 physician employees ● 50% burned out ● 7. 5% annual turnover Estimated $5, 625, 000 cost of physician turnover per year due to burnout

Why burnout matters to physicians Gittlen S, NEJM Catalyst, 2017

The Problem is it us?


Duty Litigation Society Colleagues Workload Bureaucracy Time Individual Mental Health Policies Regulation Division/ Practice Debt Salary Health System

Where do we start?

Burnout PTSD Depression

Depression - 6. 7% prevalence in US adults - 27% of medical students and residents - Up to 24% of interns suffer suicidal thoughts during their first year Sen et al. Arch Gen Psy 2010, Rotenstein LS et al. JAMA 2016, NIMH 2016

85. 2%

Physician suicide. ➔ 300 -400 physicians commit suicide every year, or ~1 physician per day ➔ 1. 4 -2. 3 x the rate of the general population ➔ 2. 5 -4 x higher for women ➔ Not exclusive to the U. S. Frank et al 1999, Schernhammer et al 2004, Sobowale et al 2014, Hope et al 2014, Cuttilan et al 2016

How did this happen?

Burnout begins during medical school Life events Environment ● ● ● ● ● First patient death The Match Licensure requirements Job search Adapted from Dyrbye L and Shanafelt T, Med Ed, 2016 Lack of control Work compression Academic support Autonomy vs. supervision Cynicism Lack of personal care

“Yet, what about beneficence? We tried to be beneficent, but a slow, ghastly, death in front of strangers in white coats doesn’t seem to be good for anybody, including me. “

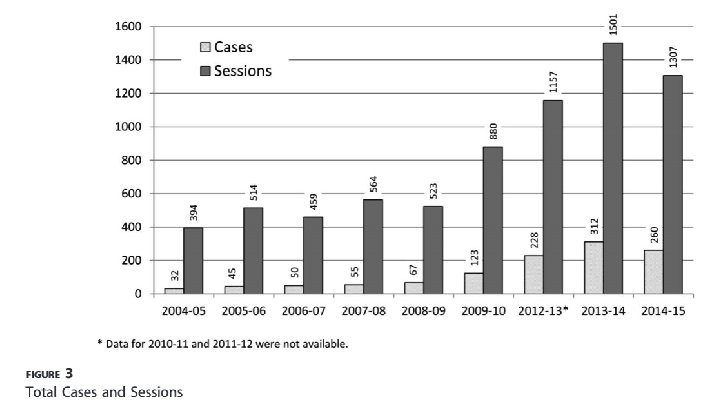
Program Structure ● ● ● 2, 000 Resident Physicians, Academic Hospital Wellness orientation, follow-up workshops Suicide prevention screening (opt-out) Resident support groups/luncheons (monthly) Individual counseling, med management Consultation with program leadership
 - 85% goes toward physician FTE")
$$$ - Start-up costs of $200, 000/year (GME) - 85% goes toward physician FTE - 5% on-site clinic space - 10% administrative expenses

Conclusions - Can be implemented with high utilization and high satisfaction rates - Unclear if depression or suicide incidence actually reduced. . .

Interventions - Faculty development - Provisions for private/university counseling services - Well-being workshops and handbook for students Depression prior to intervention Depression after intervention Mild/Moderate depression Major depression Suicidal ideation 44 (76%) 14 (24%) 4 (7%) 10 (17%) 1 (3%)

Ok, I’m not depressed… But I’m still burned out

Duty Litigation Society Colleagues Workload Bureaucracy Time Individual Mental Health Policies Regulation Division/ Practice Debt Salary Health System

Study Components ● Medical students and non-physician providers excluded ● Data from both academic and community settings ● 15 RCTs (716 physicians) ● 37 unique cohort studies (2914 physicians)

Interventions Included: ●Duty hour requirements ●Shortening attending rotation length ●Practice delivery changes ●Modifications to clinical workflow ●Communication skills training ●Facilitated and non-facilitated small group curricula ●Stress management & Self care ●Mindfulness-based approaches
 NNT = 10")
Absolute reduction in overall burnout of 514% (54 ->44%) NNT = 10

Organizational interventions more effective than individual efforts in reducing overall burnout Mindfulness and stress management strategies appeared more effective in reducing depersonalization

Limitations ● Many studies lacked a control arm ● Personal accomplishment not specifically addressed

19 studies 7 of which included in previous meta-analysis Organization led or directed efforts may have more impact on burnout than individuallevel efforts

“. . . burnout is rooted in the organizational coherence of the health care system. If burnout is a problem of whole health care systems, it is less likely to be effectively minimized by solely intervening at the individual level. It requires an organization-embedded approach. ”

25 studies from the Western Hemisphere examining the general work environment: Job Control Emotional Demands Co-worker support Work Load Job development Lack of feedback Physical environment

“The potential importance of organizational interventions is illustrated by the findings that the development of the burnout syndrome is influenced by structural work environment factors such as job demands, low possibility to exert control and non-supportive workplaces. ”

Duty Hours and Burnout Improved Emotional Exhaustion Improved? ? Depersonalization

Duty Hours and Burnout Impaired Personal Accomplishment? ? ?
")
Adverse effects of duty hours ● Decreased continuity of patient care ● Less (formal/bedside) educational time ● Limits assessment of resident skills, judgement and professionalism

“More time at the bedside. Shared sense of teamwork. Decreased burden of administrative tasks. Adequate nonclinical support staff. Mentorship and education. ” “Returning to why we entered the profession. Practicing self-reflection. Peer-support and a sense of community. ”

Gittlen S, NEJM Catalyst, 2017

Physicians spend 49% of their time on the EHR and desk work vs only 27% of their time face to face with patients (2: 1 ratio)
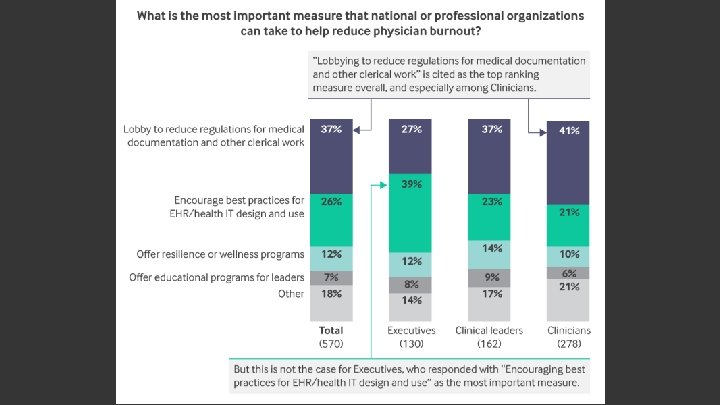

Estimated that by 2020 there will be 1 scribe for every 9 physicians. Gellert GA et al, JAMA 2015

Physician satisfaction working with scribes Outcome OR 95% CI P-Value Overall satisfaction 10. 75 5. 36 -21. 58 <. 001 Face time with patients 3. 71 1. 91 -7. 21 <. 001 Charting time 86. 09 19. 58 -378. 41 <. 001 Chart quality 7. 25 3. 42 -15. 39 <. 001 Chart accuracy 4. 61 2. 11 -10. 06 <. 001

Patient Satisfaction Outcome OR 95% CI P-Value Physician explains things to me 0. 82 0. 48 -1. 40 . 468 Physician listens to me 0. 88 0. 49 -1. 58 . 681 Physician cares about me 1. 15 0. 67 -1. 97 . 609 Physician encourages me to talk 1. 07 0. 63 -1. 808 Physician spends enough time with me 1. 12 0. 70 -1. 79 . 642

April, 2016

Qualitative study using descriptive themes ● 18 physicians ● 17 scribes ● 36 patients Documentation - requires letting go of some control Patient Care - teaching and summarizing with patients Teamwork - it’s like a dance. . .

“. . . not doing administrative things, he’s being the doctor. ” “I felt more cared for today…” “the bulk of the time should really be on the assessment and plan and I really feel like we're having…very effective conversations about that. ”

5 Studies included - Satisfaction, efficiency and interaction quality all seem to improve with scribes Productivity - RVUs increased. 18 to. 24 per hour - Patients increased 2. 2 to 3. 5 per hour - Estimated revenue increase of $2500 per hour in one cardiology clinic

Scribes aren’t an excuse to quit improving the EMR

Questions?

Conclusions ● The scope of burnout is extensive ● Organizational change is likely essential, but self -care may be of beneficial magnitude ● Controlled studies of medical scribes, EHR workflow and care delivery models are coming

Thank you!
- Slides: 70