Colon Rectal and Anal Cancers After the Colonoscopy









 • Pathologic (p) • Post -therapy (y) • Recurrence (r)")


 • Address Øclinical")





 – p. TNM,")















- Slides: 35
Colon, Rectal and Anal Cancers After the Colonoscopy Karen Norris, BSN, RN, OCN Nurse Navigator Franciscan Health March 10, 2018
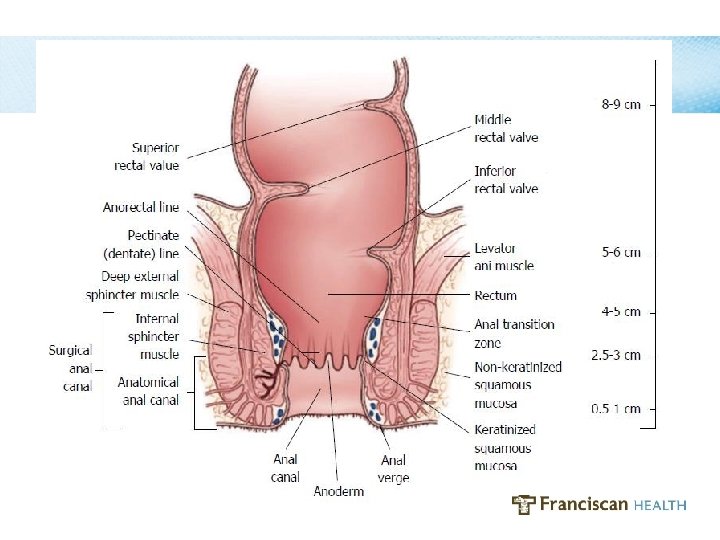
Learning Objectives At the conclusion of this presentation, participants will be able to… • Identify the anatomic landmarks and histology that differentiate colon, rectal and anal cancers from one another • Identify one test and one procedure used to confirm the location of a rectal cancer • Identify appropriate workup/staging tests for colon, rectal and anal cancers
Learning Objectives At the conclusion of this presentation, participants will be able to… • Identify one resource at Franciscan Health that is available to patients and families following a diagnosis of colon, rectal and anal cancer
Colorectal Cancer • Second most lethal cancer in the U. S. • Risk factors- – Personal history of Crohn’s or UC – Personal/family history (1 st degree) of CRC or CR polyps – Familial history of Lynch Syndrome or FAP – Age, gender – Obesity/physical inactivity – ETOH, Tobacco – High fat/calorie diet & diets low in fiber, fruits, veggies
Colorectal Cancer • Prevention -Schedule an appt at IG&H -Screening Colonoscopy- Gold Standard -removal of precancerous polyps -early detection
Referrals Receive at any and every point of care Receive from every type of provider Physician calls directly Staff call/fax pertinent information Name, DOB, demographics, H&P, colonoscopy report, pathology report • •
Histopathologic Type • • • Adenocarcinoma in situ Adenocarcinoma Medullary carcinoma Mucinous carcinoma Signet ring cell carcinoma Squamous cell (epidermoid) carcinoma Adenosquamous carcinoma High-grade neuroendocrine carcinoma (sm, lg) Undifferentiated Carcinoma, NOS (not otherwise specified)
Staging Franciscan Tumor Registry State Cancer Registry NCDB Prognosis/Prognostic Models/Prognostic Features • Treatment • Incidence • Cancer Research • •
Staging • T=Tumor – Size and extent of the primary tumor • N= Node – Involvement of regional lymph nodes • M= Metastases – Presence or absence of distant metastases
Staging • Clinical (c) • Pathologic (p) • Post -therapy (y) • Recurrence (r) • Autopsy (a) • Multiple primary tumors (m)
Staging • Prognostic Features ØLVI ØPNI ØTumor deposits ØSurgical margin status ØNumber of lymph nodes harvested ØTumor grade
Staging • Prognostic Features ØMSI ØKRAS, NRAS, BRAF, Pik 3 Ca ØTumor regression in rectal cancer ØObstruction or perforation
NCCN Guidelines • Disease site- clinicians, patients • Updated annually (minimum) • Address Øclinical presentation Øinitial work-up Øfindings Øprimary treatment Øsurveillance Ørecurrence
NCCN Guidelines • All Colon and Rectal Cancers: ØInvasive cancer confirmed pathologically ØChest/abd/pelvic CT with contrast ØCEA (prior to treatment if appropriate)
NCCN Guidelines • All Rectal Cancers: -Pelvic MRI – rectal protocol -Physical exam by Colorectal Surgeon • Confirm anatomic location of the tumor -above/below the peritoneal reflection -measure distance from internal sphincter to distal edge of tumor
NCCN Guidelines • All Anal Cancers: -DRE -Inguinal Lymph Node evaluation -Anoscopy -Chest/abd/pelvic CT -Consider PET for T 2 -T 4, N 0 or any T, N+ -Consider HIV testing and CD 4 level -GYN exam, screen for cervical CA -HPV
NCCN Guidelines • Exceptions to the rule – Not pathologically confirmed ØClinician expertise – Obstructing – Perforated
Colon Cancer Initial Work-up Initial Work Up * Colonoscopy C / I * Pathology Review Marking of cancerous polyp site (pedunculated and sessile polyp with invasive cancer) at time of colonoscopy or within 2 weeks if deemed necessary by the surgeon * CEA * CBC * Chemistry profile – CMP/BMP/LFT’s Chest/Abd/Pelvic CT Scan * CXR - PA/LAT/Single for suspected or proven metastatic * adenocarcinoma RAS (KRAS/NRAS) and BRAF M 1 -Needle Bx if clinically indicated M 1 -Multidisciplinary team evaluation including surgeon experienced in * resection of hepatobiliary and lung metastatses Consider PET/CT scan if potentially * surgically curable M 1 disease in selected cases IHC, MSI, Colaris Clinical Trial (surgical) Appropriate MD Consult? Date Guideline Met Notes
Colon Cancer Primary Treatment • Surgery (excluding Stage IV diagnosed pre-op) – p. TNM, Stage 0 -IV – Stage 0 - p. Tis- non invasive – Stage 1 and some Stage 2 - surgical cure – Stage 2 with high-risk features- chemo may be recommended – Stage 3 - chemo recommended – Stage 4 - chemo recommended Medical Oncology referral- port, start within 3 -4 wks
Rectal Cancer Initial Work-up Initial Work Up Date Colonoscopy C / I Biopsy Confirming Cancer Marking of cancerous polyp site (pedunculated or sessile polyp with invasive cancer) at time of colonoscopy or within 2 wks if deemed necessary by the surgeon Guideline Met Chest/Abd/Pelvic CT Scan Pelvic MRI CEA prior to Definitive Treatment ET as indicated for pre-op marking of site, teaching Molecular markers should be assessed when appropriate: RAS (KRAS/NRAS) for suspected or proven metastatic adenocarcinoma (if RAS non-mutated, consider BRAF testing) PET/CT Scan (not routinely indicated) Clinical Stage IHC Clinical Trial (neo-adj or surgical) Appropriate MD Consult? * 2. 1 * 2. 3 2. 4 2. 14 * Rigid Proctoscopy Notes
Rectal Cancer Primary Treatment • c. T 1 -2, N 0: TEM (below peritoneal reflection) or resection • c. T 3 -4, N 0 -2: neoadjuvant concurrent chemoradiation, surgery, adjuvant chemotherapy
Anal Cancer Initial Work-up * * * * Initial Work Up Biopsy: Squamous cell carcinoma Digital Rectal Exam (DRE) Inguinal lymph node evaluation -Biopsy or FNA if suspicious nodes Anoscopy – Chest/Abd/pelvic CT or MRI Consider PET/CT scan for T 2 -T 4, N 0 or Any T, N+ Consider HIV testing and CD 4 level if indicated Gynecological exam for women, including screening for cervical cancer * Clinical Stage Appropriate MD Consult? Chemotherapy Regimen • Start date • Completion date Radiation Therapy • T 1 -T 2, N 0 - RT @ (45 -59 Gy) • T 3 -T 4, N 0 or Any T, N+ RT @ (55 -59 Gy) Start date Completion date Guideline Met Date Notes Tx Phase- Anal Canal Notes Guideline Met Date
Anal Canal Primary Treatment • Locoregional Disease Concurrent chemoradiation- Nigro Protocol • Metastatic Disease Systemic monotherapy. Cisplatin-based therapy
Potential Side Effects Nausea/vomiting Diarrhea Skin dryness Sun sensitivity Neuropathy Vision changes Depression Weight Loss Mouth sores Hair Loss Anemia Neutropenia Thrombocytopenia Fatigue “Chemo brain” Acneform rash
Side Effect Prevention • Prevention is key -6 -8, 8 oz glasses of fluid daily -Small, frequent meals- low fiber, low spice -Increase calorie and protein intake -Good oral hygiene -Use medications at first indication -Sunscreen -Report temp ≥ 100. 5
Side Effect Prevention • Prevention is key -Frequent hand washing -Keep skin moisturized, fragrance-free -Avoid large crowds during nadir -Get plenty of rest daily Post tx: females- radiation- vaginal dilators
What the Future Holds • Immunotherapy – Check point inhibitors and immune modulators – Monoclonal antibodies – Therapeutic vaccines – Adoptive cell therapy – Oncolytic virus therapy – Adjuvant immunotherapies – Cytokines • Personalized Treatment – Next-generation sequencing technology
Colorectal Cancer • Reducing Risk after Cancer -30 minutes moderate activity 4 x/wk -Low glycemic index diet -MVI daily -Coffee (caffeinated) 4 c/d -tree nuts or tree nut products 2 serv/wk -ASA 81 -325 mg/d
Resources • Support Groups- Cancer Support Community – Patients, Caregivers • • • Look Good Feel Better- ACS Live Strong at the Y Massage Therapy Oasis Cancer Center Social Worker Supportive Care Clinic Genetic Counseling Moving Beyond Well Beyond
Resources • Site Specific Cancer Nurse Navigators – Colorectal – Breast – Lung – Gyn – Melanoma – Prostate – Second Opinion
Resources • Franciscan Cancer Center Administration 317 -528 -8918 • Karen Norris, RN, BSN, OCN Colorectal Nurse Navigator 317 -528 -7145
Colon, Rectal and Anal Cancers Thank you!
References • ACS at https: //www. cancer. org/ • https: //www. geoface. com • AJCC Cancer Staging Manuel, Eighth Edition: Editors: Amin, M. B. , Edge, S. , Greene, F. , Byrd, D. R. , Brookland, R. K. , Washington, M. K. , Gershenwald, J. E. , Compton, C. C. , Hess, K. R. , Sullivan, D. C. , Jessup, J. M. , Brierley, J. D. , Gaspar, L. E. , Schilsky, R. L. , Balch, C. M. , Winchester, D. P. , Asare, E. A. , Madera, M. , Gress, D. M. , Meyer, L. R. (Eds. ) • NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Colon Cancer. Version 2. 2017. © 2017 National Comprehensive Cancer Network. https: //www. nccn. org/professionals/physician_gls/default. aspx#site • Reducing Risk After Cancer: Healthy Lifestyle (and Tree Nuts) - Medscape May 18, 2017.