COLON CANCER PRESENTED BY RAHAF HASANEIN ANATOMY BLOOD

COLON CANCER PRESENTED BY: RAHAF HASANEIN

ANATOMY+ BLOOD SUPPLY
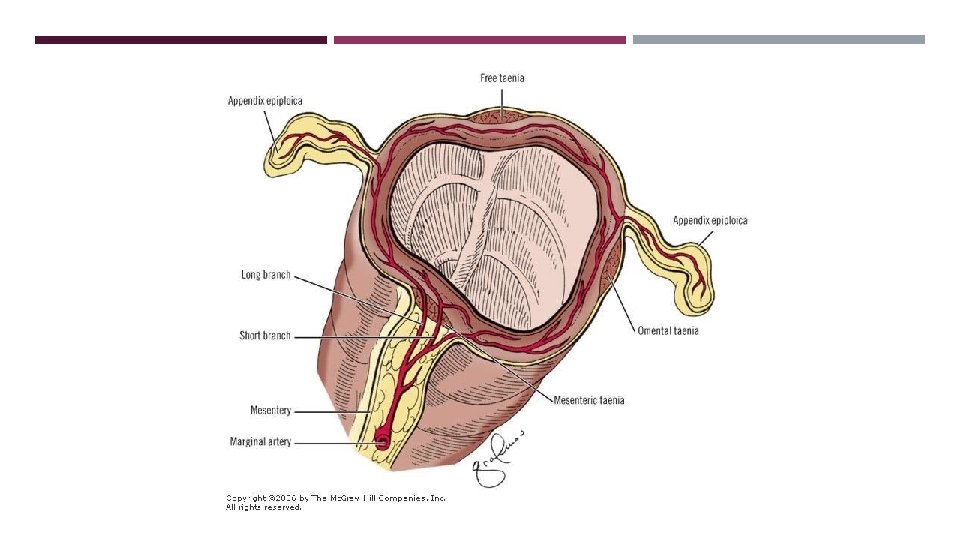

COLON ARTERIAL SUPPLY SMA branches into : Ileocolic artery (terminal ileum and proximal ascending colon). Right colic artery (ascending colon). Middle colic artery (transverse colon). IMA branches into: Left colic artery (descending colon). Several sigmoidal branches (sigmoid colon) Superior rectal artery (proximal rectum). The terminal branches of each artery form anastomoses with the terminal branches of the adjacent artery and communicate via the marginal artery of Drummond.

VENOUS DRAINAGE The veins of the colon parallel their corresponding arteries and bear the same terminology. IMV ascends in the retroperitoneal plane over the psoas muscle and continues posterior to the pancreas to join the splenic vein.

THE LYMPHATIC DRAINAGE Lymphatic vessels and lymph nodes follow the regional arteries.

COLON NERVE SUPPLY The Sympathetic nerves arise from T 6 -T 12 and L 1 -L 3. The parasympathetic innervation to the right and transverse colon is from the vagus nerve; the parasympathetic nerves to the left colon arise from sacral nerves S 2 -S 4.

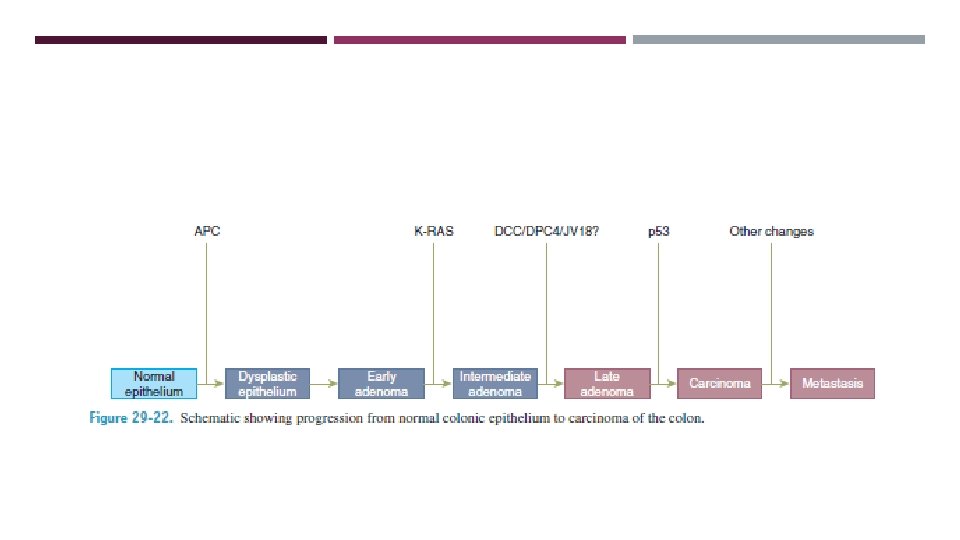
POLYPS Nonspecific clinical term that describes any projection from the surface of the intestinal mucosa regardless of its histologic nature. Most colorectal carcinomas evolve from adenomatous polyps.

ADENOMATOUS POLYPS 25% of the population older than 50 years of age. Increase risk of malignancy? Classification: (acc. To histology) Tubular adenomas (5%). villous adenomas (40%). Tubulovillous adenomas (22%).
 § Pedunculated -> colonoscopic snare excision. § Sessile § Complications of")
(Acc. To shape) § Pedunculated -> colonoscopic snare excision. § Sessile § Complications of polypectomy include perforation and bleeding.
 -> hyperplasia without")
HYPERPLASTIC POLYPS Extremely common. These polyps are usually small (<5 mm) -> hyperplasia without any dysplasia. Large hyperplastic polyps (>2 cm) -> foci of adenomatous tissue and dysplasia Hyperplastic polyposis is a rare disorder in which multiple large hyperplastic polyps occur in young adults. These patients are at slightly increased risk for the development of colorectal cancer.

SERRATED POLYPS Saw-toothed appearance under the microscope. Some of these polyps will develop into invasive cancers. A familial serrated polyposis syndrome. Serrated polyps should be treated like adenomatous polyps.
 Not premalignant. Associated with mutation in PTEN. Bleeding is a common")
HAMARTOMATOUS POLYPS (JUVENILE) Not premalignant. Associated with mutation in PTEN. Bleeding is a common symptom, and intussusception and/or obstruction may occur. Treated by polypectomy.

FAMILIAL JUVENILE POLYPOSIS AD disorder in which patients develop hundreds of polyps in the colon and rectum. Annual screening should begin between the ages of 10 and 12 years. Treatment is surgical and depends on the degree of rectal involvement If the rectum is relatively spared, a total abdominal colectomy with ileorectal anastomosis. If the rectum is carpeted with polyps, total proctocolectomy is the more appropriate operation and ileal pouch–anal reconstruction to avoid a permanent stoma

PEUTZ-JEGHERS SYNDROME polyposis of the small intestine, the colon and rectum. Characteristic melanin spots on the buccal mucosa and lips of these patients. . Carcinoma may develop. Surgery for symptoms. Screening consists of a baseline colonoscopy and upper endoscopy at age 20 years, followed by annual flexible sigmoidoscopy thereafter.

CRONKITE-CANADA SYNDROME GI polyposis in association with alopecia, cutaneous pigmentation, and atrophy of the fingernails and toenails. Diarrhea is a prominent symptom, and vomiting, malabsorption, and protein-losing enteropathy may occur. Most patients die of this disease. Surgery for complications.

COWDEN’S SYNDROME AD. Hamartomas of all three embryonal cell layers. Facial trichilemmomas, breast cancer, thyroid disease and gastrointestinal polyps. Patients should be screened for cancers. Treatment is otherwise based on symptoms.

INFLAMMATORY POLYPS Not premalignant. In inflammatory bowel disease After amebic colitis, ischemic colitis, and schistosomal colitis. Microscopic examination shows islands of normal, regenerating mucosa (the polyp) surrounded by areas of mucosal loss. Polyposis may be extensive, especially in patients with severe colitis, and may mimic FAP.

INHERITED COLORECTAL CARCINOMA

FAMILIAL ADENOMATOUS POLYPOSIS AD, 1% of all colorectal adenocarcinomas. Mutation in the APC gene, on chromosome 5 q (positive in 75% of cases). Up to 25% present without other affected family members. Hundreds to thousands of adenomatous polyps shortly after puberty. Risk of colorectal cancer 100% by age 50 years.

APC gene testing + annual flexible sigmoidoscopy beginning at age 10 to 15 years is done until polyps are identified. - Refused or unavailable annual flexible sigmoidoscopy beginning at age 10 to 15 years is performed until age 24 years. every 2 years until age 34 years every 3 years until age 44 years then every 3 to 5 years.

Risk for the development of adenomas anywhere in the gastrointestinal tract, particularly in the duodenum. Upper endoscopy (every 1 to 3 years beginning at age 25 to 30 years). Treatment is surgical. Three operative procedures can be considered: 1. Total proctocolectomy with an end (Brooke) ileostomy 2. Total abdominal colectomy with ileorectal anastomosis 3. Restorative proctocolectomy with ileal pouch–anal anastomosis with or without a temporary ileostomy.

FAP may be associated with extraintestinal manifestations such as congenital hypertrophy of the retinal pigmented epithelium, desmoid tumors, epidermoid cysts, mandibular osteomas (Gardner’s syndrome) central nervous system tumors (Turcot’s syndrome). Desmoid tumors are often hormone responsive, and growth may be inhibited in some patients with tamoxifen. COX-2 inhibitors and nonsteroidal, anti-inflammatory drugs may also be beneficial in this setting.

ATTENUATED FAMILIAL ADENOMATOUS POLYPOSIS Variant of FAP. Present later in life with fewer polyps (usually 10– 100) predominantly in the right colon. CRca develops in more than 50% of these patients, but occurs later (average age, 55 years). Patients are also at risk for duodenal polyposis. APC gene mutations are present in only about 30% (AD) Mutations in MYH also result in the(AR).

Genetic testing. When positive, screen at-risk family members. If the family mutation is unknown, screening colonoscopy is recommended beginning at age 13 to 15 years, then every 4 years to age 28 years, and then every 3 years. These patients are often candidates for a total abdominal colectomy with ileorectal anastomosis because the limited polyposis in the rectum can usually be treated by colonoscopic snare excision. Prophylaxis with COX-2 inhibitors.
. HNPCC (Lynch’s syndrome) is more common than FAP.")
HEREDITARY NONPOLYPOSIS COLON CANCER (LYNCH’S SYNDROME). HNPCC (Lynch’s syndrome) is more common than FAP. (1%– 3% of all colon cancers). AD, Errors in mismatch repair. Development of colorectal carcinoma at an early age (average age, 40– 45 years). Approximately 70% Cancers appear in the proximal colon and have a better prognosis regardless of stage. The risk of synchronous or metachronous colorectal carcinoma is 40%. May also be associated with extracolonic malignancies, including endometrial carcinoma, which is most common, and ovarian, pancreas, stomach, small bowel, biliary, and urinary tract carcinomas.

The diagnosis is made based on family history. The Amsterdam criteria for clinical diagnosis of HNPCC are: Three affected relatives with histologically verified adenocarcinoma of the large bowel (one must be a first-degree relative of one of the others) in two successive generations of a family with one patient diagnosed before age 50 years. The presence of other HNPCC-related carcinomas should raise the suspicion of this syndrome.

Screening colonoscopy is recommended annually for at risk patients beginning at either age 20 to 25 years or 10 years younger than the youngest age at diagnosis in the family, whichever comes first. Because of the high risk of endometrial carcinoma, transvaginal ultrasound or endometrial aspiration biopsy is also recommended annually after age 25 to 35 years.

Because there is a 40% risk of developing a second colon cancer, total colectomy with ileorectal anastomosis is recommended once adenomas or a colon carcinoma is diagnosed. Annual proctoscopy is necessary because the risk of developing rectal cancer remains high. Similarly, prophylactic hysterectomy and bilateral salpingo-oophorectomy should be considered in women who have completed childbearing.

FAMILIAL COLORECTAL CANCER 10% to 15% of patients with colorectal cancer. Diagnosis before the age of 50 years is associated with a higher incidence in family members. Screening colonoscopy is recommended every 5 years beginning at age 40 years or beginning 10 years before the age of the earliest diagnosed patient in the pedigree.

ADENOCARCINOMA AND POLYPS Most common malignancy of the GIT. Third most common cancer in women and men. Third leading cause of cancer-related deaths. F: M 1: 1

RISK FACTORS Aging Hereditary Risk Factors Environmental and Dietary Factors Inflammatory Bowel Disease Cigarette smoking Patients with ureterosigmoidostomy Acromegaly Pelvic irradiation
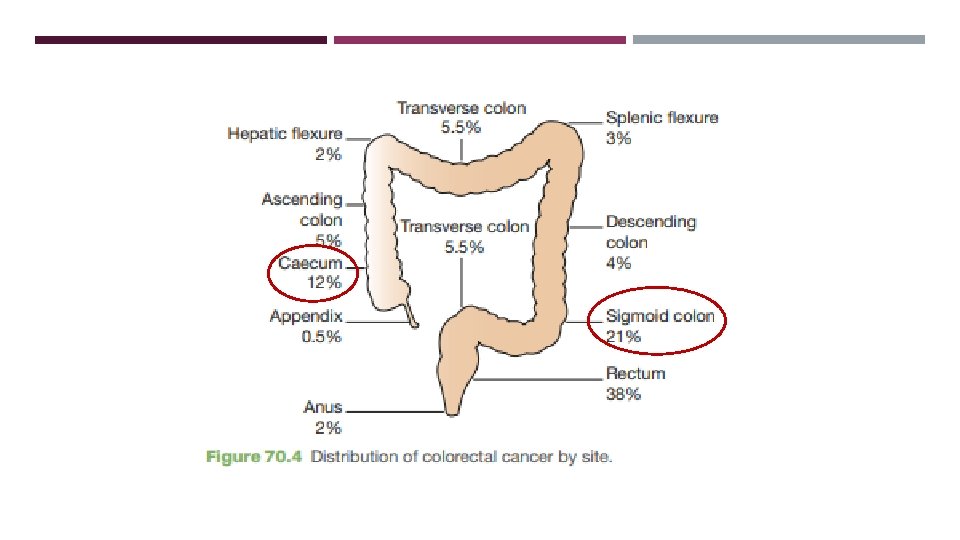

CLINICAL FEATURES Depend on: Site, Presence of complications and metastases.

SPREAD Direct extension Hematogenous lymphatic
 OR")
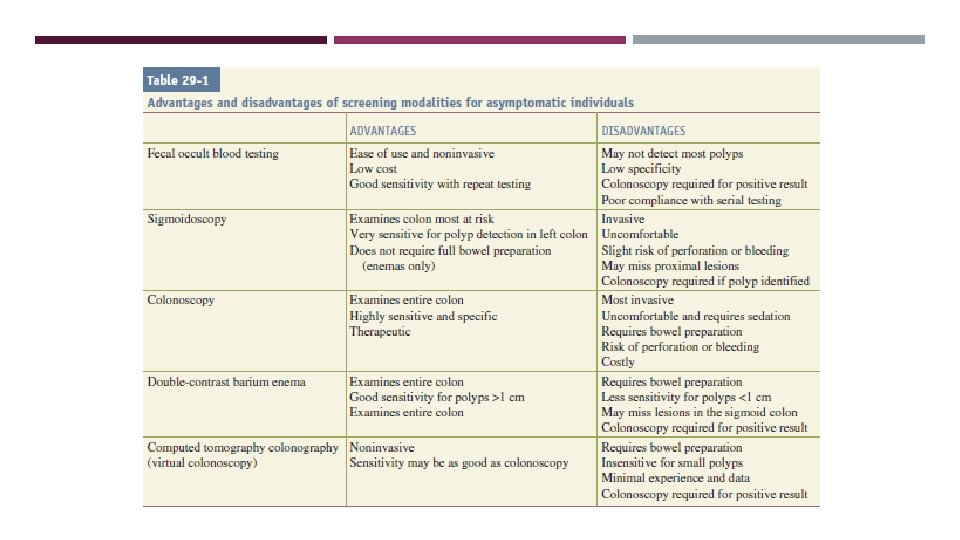
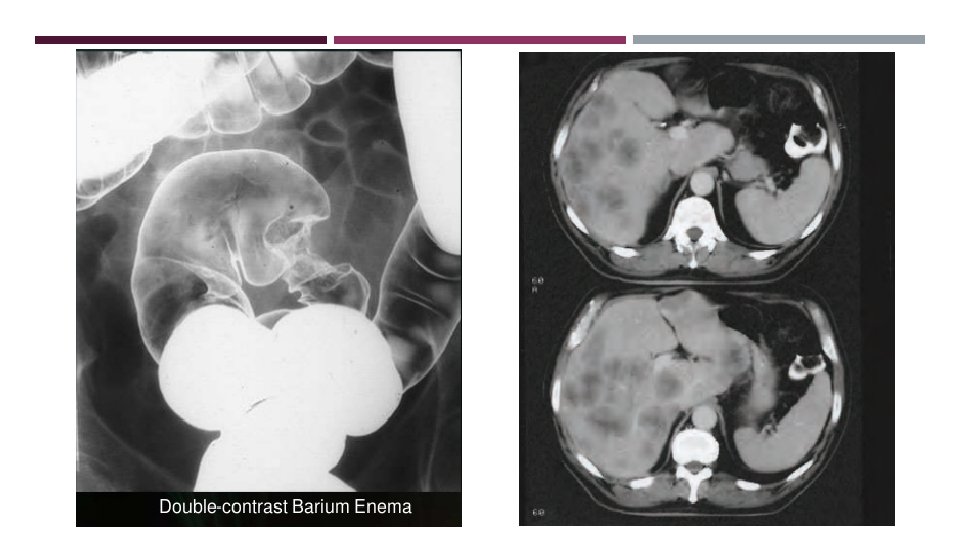
DIAGNOSIS Hx+ PE Colonoscopy to obtain biopsy and evaluate for synchronous tumors (5%) OR flexible sigmoidoscopy and barium enema. CBC, LFT Water-soluble contrast enema is performed to assess the degree and level of obstruction and to “clear” the colon proximal to the obstruction. A chest/abdominal/pelvic CT. PET scan (It is routinely performed prior to concurrent colectomy and liver resection for hepatic metastases) CEA

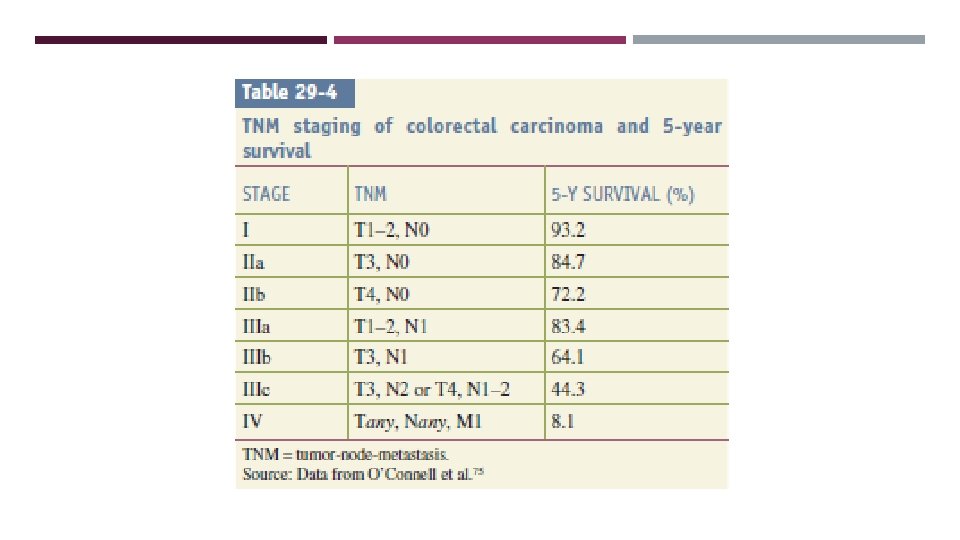
STAGING

MANAGEMENT surgical resection: Remove the primary tumor along with its lymphovascular supply ➢ Surgeries could be curative or palliative Adjuvant chemotherapy: stage III / VI or locally advanced stage II combination of 5 -fluorouracil/leucovorin with either irinotecan (FOLFIRI) or oxaliplatin (FOLFOX).
: Polypectomy Segmental resection.")
STAGE-SPECIFIC THERAPY Stage 0 (Tis, N 0, M 0): Polypectomy Segmental resection.
: Invasive carcinoma in")
Stage I: The Malignant Polyp (T 1, N 0, M 0): Invasive carcinoma in pedunculated polypectomy or Segmental colectomy. Invasive carcinoma arising in a sessile polyp extends into the submucosa and is usually best treated with segmental colectomy
:")
Stages I and II: Localized Colon Carcinoma (T 1 -3, N 0, M 0): Surgical resection. Adjuvant chemotherapy has been suggested for selected patients with stage II disease (young patients, tumors with “high-risk” histologic findings).
 Adjuvant chemotherapy has been")
Stage III: Lymph Node Metastasis (Tany, N 1, M 0) Adjuvant chemotherapy has been recommended routinely in these patients.
. Highly selected patients with isolated, resectable")
Stage IV: Distant Metastasis (Tany, Nany, M 1). Highly selected patients with isolated, resectable metastases may benefit from resection (metastasectomy). All patients require adjuvant chemotherapy.

colonic stenting for obstructing lesions of the left colon also provide good palliation. More limited surgical intervention such as a diverting stoma or bypass procedure may be appropriate in patients with stage IV disease who develop obstruction. Hemorrhage in an unresectable tumor can sometimes be controlled with angiographic embolization. External beam radiation also has been used for palliation.

RIGHT HEMICOLECTOMY Carcinoma of the caecum or ascending colon. The ileocolic vessels, right colic vessels, and right branches of the middle colic vessels are ligated. Ileal-transverse colon anastomosis

EXTENDED RIGHT COLECTOMY Lesions located at the hepatic flexure or proximal transverse colon. Right hemicolectomy + reminder of transverse colon and splenic flexure. resection of right colic artery, iliocecal artery and middle colic artery. Anastomosis relies on the marginal artery of Drummond

TRANSVERSE COLECTOMY Lesions in the mid and distal transverse colon Resecting the transverse colon Ligating the middle colic vessels. Colocolonic anastomosis. Extended right may be a safer anastomosis with an equivalent functional result.

LEFT COLECTOMY Lesions in distal transverse colon, splenic flexure, or descending colon. The left branches of the middle colic vessels, the left colic vessels, and the first branches of the sigmoid vessels are ligated. A colonic anastomosis.

EXTENDED LEFT COLECTOMY Option for removing lesions in the distal transverse colon. In this operation, the left colectomy is extended proximally to include the right branches of the middle colic vessels.

SIGMOID COLECTOMY Lesions in the sigmoid colon Ligation of the sigmoid branches of the inferior mesenteric artery. anastomosis created between the descending colon and upper rectum.

TOTAL OR SUBTOTAL COLECTOMY The superior rectal vessels are preserved. If the sigmoid is to be resected (total abdominal colectomy with ileorectal anastomosis). preserve the sigmoid, the distal sigmoid vessels are left intact (subtotal colectomy with ileosigmoid anastomosis).

HARTMANN PROCEDURE.

PROCTOCOLECTOMY Total Proctocolectomy. In this procedure, the entire colon, rectum, and anus are removed, and the ileum is brought to the skin as a Brooke ileostomy. Restorative Proctocolectomy (Ileal Pouch–Anal Anastomosis). The entire colon and rectum are resected, but the anal sphincter muscles and a variable portion of the distal anal canal are preserved. Anastomosis of an ileal reservoir to the anal canal

FOLLOW-UP Stool guaiac test Annual CT scan of abdomen/pelvis and CXR for up to 5 years Colonoscopy at 1 year and then every 3 years until negative then every 5 years. CEA levels are checked periodically (every 3 months in the first year) and then every 6 months the next 4 years.

OTHER TYPES Carcinoid Tumors. Lipomas. Lymphoma. Leiomyoma and Leiomyosarcoma.

REFERENCES: Schwartz’s Principles of Surgery. Bailey and love’s short practice of surgery Surgical recall. The washington manual of surgery.

THANK YOU
- Slides: 61