Coagulation Disorders Dr S Nishan Silva MBBS HEMOSTASIS
")
Coagulation Disorders Dr. S. Nishan Silva (MBBS)

HEMOSTASIS 1. VASCULAR PHASE 2. PLATELET PHASE 3. COAGULATION PHASE 4. FIBRINOLYTIC PHASE
 • PTT BV Injury Tissue Factor")
Lab Tests Hemostasis • CBC-Plt • BT, (CT) • PTT BV Injury Tissue Factor Neural Blood Vessel Constriction Platelet Aggregation Coagulation Cascade Primary hemostatic plug Reduced Blood flow Platelet Activation Fibrin formation Plt Study Stable Hemostatic Plug Morphology Function Antibody

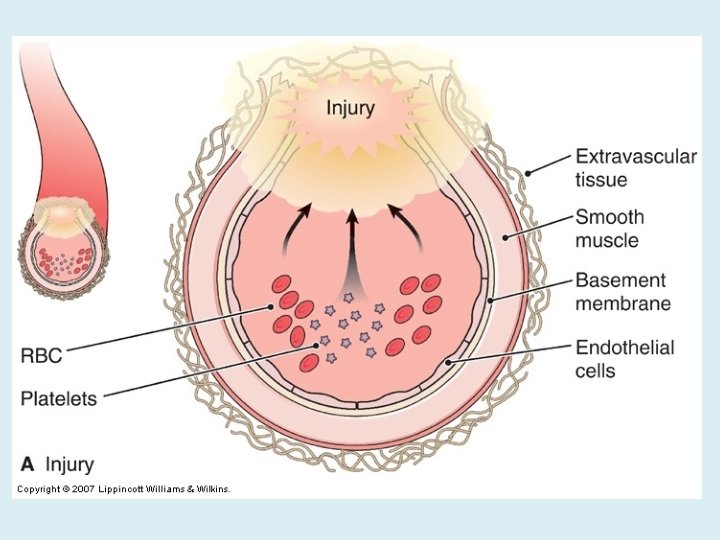
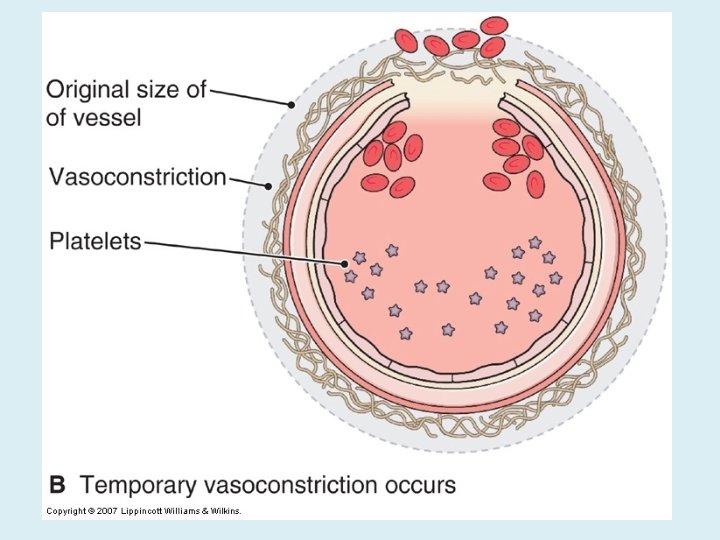
NORMAL CLOTTING Response to vessle injury 1. Vasoconstriction to reduce blood flow 2. Platelet plug formation (von willebrand factor binds damaged vessle and platelets) 3. Activation of clotting cascade with generation of fibrin clot formation 4. Fibrinlysis (clot breakdown)

CLOTTING CASCADE Normally the ingredients, called factors, act like a row of dominoes toppling against each other to create a chain reaction. If one of the factors is missing this chain reaction cannot proceed.

VASCULAR PHASE WHEN A BLOOD VESSEL IS DAMAGED, VASOCONSTRICTION RESULTS.

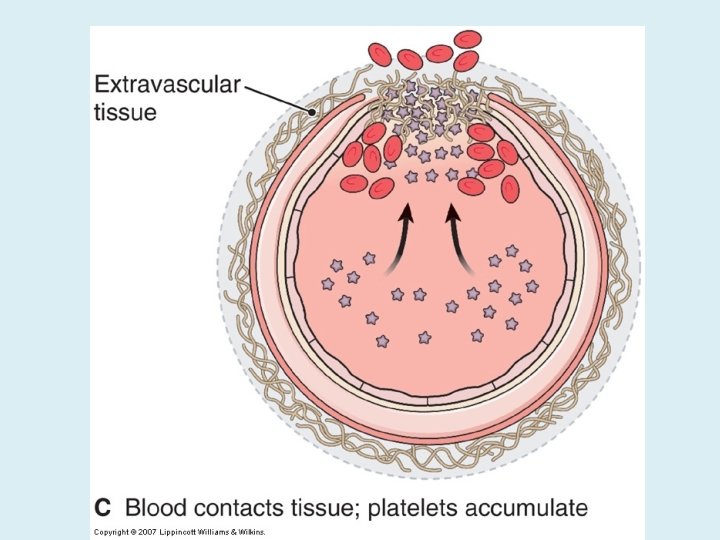
PLATELET PHASE PLATELETS ADHERE TO THE DAMAGED SURFACE AND FORM A TEMPORARY PLUG.
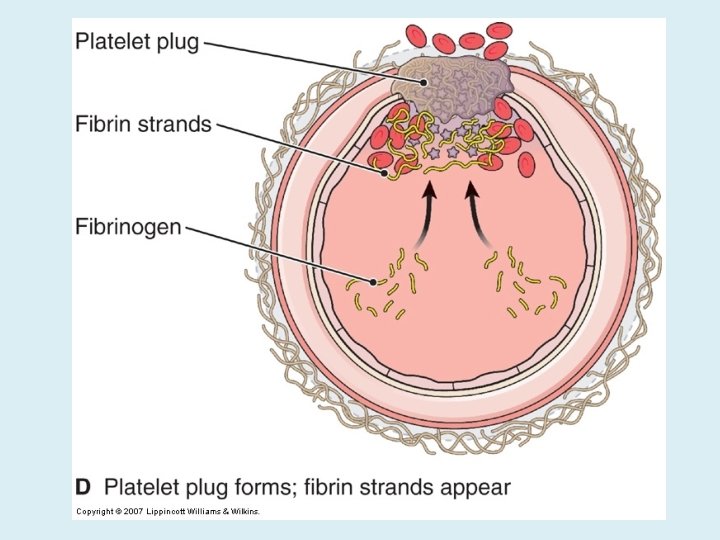
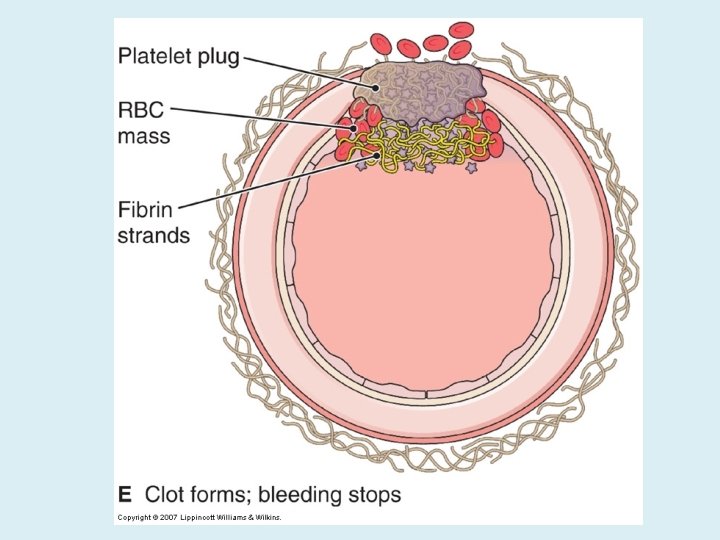

COAGULATION PHASE THROUGH TWO SEPARATE PATHWAYS THE CONVERSION OF FIBRINOGEN TO FIBRIN IS COMPLETE.

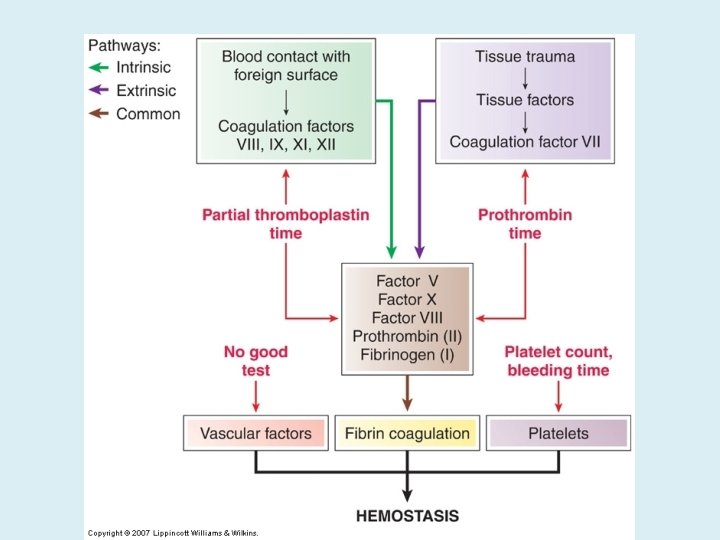
THE CLOTTING MECHANISM INTRINSIC Collagen EXTRINSIC Tissue Thromboplastin XII XI IX VIII VII X FIBRINOGEN (I) V PROTHROMBIN (II) THROMBIN (III) FIBRIN

FIBRINOLYTIC PHASE ANTICLOTTING MECHANISMS ARE ACTIVATED TO ALLOW CLOT DISINTEGRATION AND REPAIR OF THE DAMAGED VESSEL.

HEMOSTASIS DEPENDENT UPON: ¬ Vessel Wall Integrity Adequate Numbers of Platelets ® Proper Functioning Platelets ¯ Adequate Levels of Clotting Factors ° Proper Function of Fibrinolytic Pathway
 PROTHROMBIN TIME (PT) PARTIAL THROMBOPLASTIN")
LABORATORY EVALUATION • • PLATELET COUNT BLEEDING TIME (BT) PROTHROMBIN TIME (PT) PARTIAL THROMBOPLASTIN TIME (PTT) • THROMBIN TIME (TT)

PLATELET COUNT p NORMAL 100, 000 - 400, 000 CELLS/MM 3 < 100, 000 Thrombocytopenia 50, 000 - 100, 000 Mild Thrombocytopenia < 50, 000 Sev Thrombocytopenia

BLEEDING TIME l PROVIDES ASSESSMENT OF PLATELET COUNT AND FUNCTION NORMAL VALUE 2 -8 MINUTES

PROTHROMBIN TIME l Measures Effectiveness of the Extrinsic Pathway l Mnemonic - PT NORMAL VALUE 10 -15 SECS

PARTIAL THROMBOPLASTIN TIME l Measures Effectiveness of the Intrinsic Pathway l Mnemonic - PTT NORMAL VALUE 25 -40 SECS

THROMBIN TIME l Time for Thrombin To Convert Fibrinogen Fibrin l A Measure of Fibrinolytic Pathway NORMAL VALUE 9 -13 SECS
")
Clinical Features ( Of Bleeding Disorders )

Platelet Petechiae, Purpura Coagulation Hematoma, Joint bl.
 Do not blanch with pressure (cf. angiomas) Not palpable")
Petechiae (typical of platelet disorders) Do not blanch with pressure (cf. angiomas) Not palpable (cf. vasculitis)

Hemarthrosis

Hematoma

Petechiae

Purpura

Ecchymosis

Senile Purpura

Petechiae in patient with Rocky Mountain Spotted Fever

Henoch-Schonlein purpura •
")
Ecchymoses (typical of coagulation factor disorders)


Hematuria

Menorrhagia

CT scan showing large hematoma of right psoas muscle
 Blood Vessel Issues…")
(1) Blood Vessel Issues…

VESSEL DEFECTS p VITAMIN C DEFICIENCY p BACTERIAL & VIRAL INFECTIONS p ACQUIRED & p. HEREDITARY CONDITIONS

Vascular defect - cont. l Infectious and hypersensitivity vasculitides - Rickettsial and meningococcal infections - Henoch-Schonlein purpura (immune)
 Platelet Problems….")
(2) Platelet Problems….

THROMBOCYTOPENIA INADEQUATE NUMBER OF PLATELETS

THROMBOCYTOPATHY ADEQUATE NUMBER BUT ABNORMAL FUNCTION

Thrombocytopenia • Characterized by petechiae in skin or mucous membranes • 130, 000 – 400, 000/ml is normal • No concern until < 100, 000/ml • No excessive bleeding until < 50, 000/ml • Spontaneous hemorrhage at 20, 000/ml • Abnormal bleeding time • Causes include – – primary bone marrow disorder toxicity due to drugs nutritional deficiencies hypersplenism

Immune Thrombocytopenic Purpura • ITP • Common cause of low platelet count • Platelets destroyed by immune system – covered with antibodies & removed by spleen • Insidious onset • Usually presents as – – – easy bruising epistaxis bleeding gums unusual bleeding after minor trauma subungual or conjunctival petechiae
 Clotting Factor Deficiency")
(3) Clotting Factor Deficiency
 p HEMOPHILIA A p HEMOPHILIA B p von WILLEBRAND’S DISEASE")
FACTOR DEFICIENCIES (CONGENITAL) p HEMOPHILIA A p HEMOPHILIA B p von WILLEBRAND’S DISEASE
 • 80 -85% of all Hemophiliacs •")
FACTOR DEFICIENCIES l HEMOPHILIA A (Classic Hemophilia) • 80 -85% of all Hemophiliacs • Deficiency of Factor VIII • Lab Results - Prolonged PTT l. HEMOPHILIA B (Christmas Disease) F 10 -15% of all Hemophiliacs FDeficiency of Factor IX FLab Test - Prolonged PTT

Classic Hemophilia aka Hemophilia A Factor VIII deficiency X linked Most common serious inherited coagulation disorder • Normal bleeding time, PT, & platelet count • PTT is prolonged • •
 Hemarthrosis (most common) Fixed joints")
Hemophilia Clinical manifestations (hemophilia A & B are indistinguishable) Hemarthrosis (most common) Fixed joints Soft tissue hematomas (e. g. , muscle) Muscle atrophy Shortened tendons Other sites of bleeding Urinary tract CNS, neck (may be life-threatening) Prolonged bleeding after surgery or dental extractions
")
Hemarthrosis (acute)
 – made in")
von Willebrand Disease • Deficiency of von Willebrand factor (v. WF) – made in endothelial cells & megakaryocytes • One of the most common inherited coagulation disorders • Prolonged bleeding time • Normal platelet count • Platelets cannot adhere to endothelium well

PLATELET ACTIVATION Resting Platelets v. WF Platelet Adhesion

Severe Christmas Disease • • aka Hemophilia B Factor IX deficiency Named for 1 st patient it was identified in X linked
")
Acquired Causes ( For Bleeding )

Disseminated Intravascular Coagulation • DIC • Clotting inside vessels • May cause obstruction in smaller vessels • Eventually begin to bleed due to consumption of coagulation factors – consumptive coagulopathy • Not a primary disease • Anemia, thrombosis, & hemorrhage • Initiated by – obstetrical complications • toxemia • abruptio placentae – infections • gram-negative sepsis • malaria – neoplasms – tissue trauma • crush injuries • burns – others • snakebite • heat stroke

Primary Events in DIC Underlying Disorder Systemic Activation of Coagulation Widespread Intravascular Fibrin Deposition Thrombosis Consumption of Platelets and Clotting Factors Bleeding K. Mc. Inerny. American Academy of Pediatrics textbook of pediatric care. 2009 59

Post-varicella purpura fulminans De. Loughery, ASH Image Bank, 2004 60
 Prothrombin")
Diagnosis of DIC • Screening tests: – – Activated partial thromboplastin time (prolonged) Prothrombin time (prolonged) Fibrinogen (decreased) Platelet count (decreased) • Confirmatory tests: – D-dimer (elevated) – Fibrin degradation products (elevated) 61

Liver Disease • Liver synthesizes and clears both procoagulants and inhibitors • Paradoxically factor VIII is often elevated – Likely due to decreased clearance • Reduced factor V helps distinguish liver synthetic dysfunction from vitamin K deficiency • Fibrinogen the last to fall • Structural manifestations of liver disease contribute to bleeding – Portal hypertension, varices, gastritis, hemorrhoids 62

Vitamin K deficiency • Vitamin K cycle • Mechanisms of Vitamin K deficiency • Warfarin action 63

Mechanisms of Vitamin K deficiency • Nutritional depletion – Alcoholics, long-term IV nutrition • Antibiotic administration – Interfere with bacteria synthesis and absorption • Warfarin – Inhibition of epoxide reductase and (to a lesser degree) quinone reductase 65

Acquired coagulation disorders dr msaiem

Renal Disease. • In acute and chronic renal diseases there is often bleeding tendency associated several haemostatic abnormalities. • Thrombocytopenia frequently develop in uremia • Vitamin K deficiency due to malnutrition, associated liver disease with factor V deficiency. dr msaiem

Massive Transfusion • Defined as transfusion of more than 1. 5 times the patient’s blood volume in 24 h • Acquired coagulopathy results from dilution of plasma and platelets and excess anticoagulant – 10% of transfusion is anticoagulant • Prevention: – Administer 1 unit FFP and calcium chloride for every 4 -6 units PRBC’s 68

- Slides: 70