CNS ABSCESSES M MOLAVI MD CNS ABSCESSES Focal

CNS ABSCESSES M. MOLAVI MD

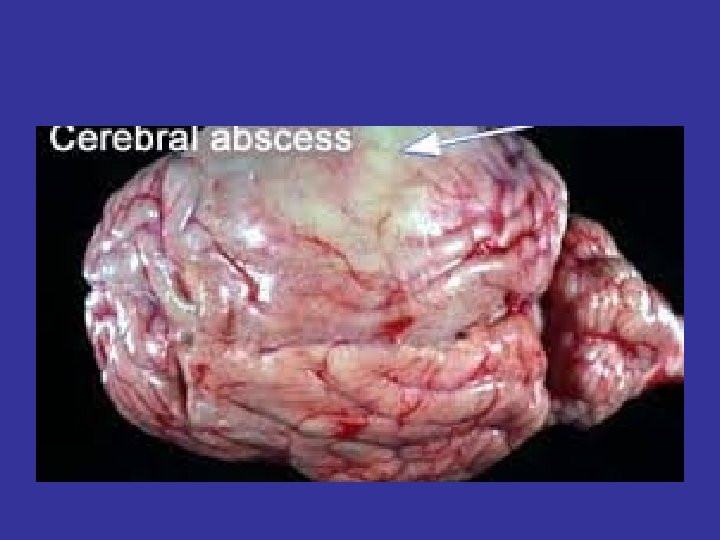
CNS ABSCESSES • Focal pyogenic infections of the central nervous system • Exert their effects mainly by: – Direct involvement & destruction of the brain or spinal cord – Compression of parenchyma – Elevation of intracranial pressure – Interfering with blood &/or CSF flow • Include: Brain abscess, subdural empyema, intracranial epidural abscess, spinal cord abscess

BRAIN ABSCESS • Accounts for ~ 1 in 10, 000 hospital admissions in US (1500 -2500 cases/yr) • Major improvements realized in diagnosis & management the last century, & especially over the past three decades, with:

BRAIN ABSCESS • Was uniformly fatal before the late 1800’s • Mortality down to 30 -60% from WWII-1970’s – Introduction of abx (penicillin, chloramphenicol. . . ) – newer surgical techniques • Mortality down to 0 -24% over the past three decades, with: – – – Advent of CT scanning (1974), MRI Stereotactic brain biopsy/aspiration techniques Further improvement in surgery Newer abx (e. g. cephalosporins, metronidazole. . ) Better treatment of predisposing conditions
 – Marked")
CHANGES IN EPIDEMIOLOGY OF BRAIN ABSCESS (in the last 2 -3 decades) – Marked drop in mortality overall – Lower incidence of otogenic brain abscesses – improved treatment of chronic ear infections – With increase in No. of immunosuppressed patients: • increased incidence of brain abscess seen in that population (Transplant, AIDS, …) • More incidence of brain abscess caused by opportunistic pathogens (fungi, toxo…)
 • Evolves into a collection")
PATHOPHYSIOLOGY • Begins as localized cerebritis (1 -2 wks) • Evolves into a collection of pus surrounded by a well-vascularized capsule (3 -4 wks) • Lesion evolution (based on experimental animal models): – – Days 1 -3: “early cerebritis stage” Days 4 -9: “late cerebritis stage” Days 10 -14: “early capsule stage” > day 14: “late capsule stage”
 • Hematogenous (25 -35%) •")
PATHOGENESIS • Direct spread from contiguous foci (40 -50%) • Hematogenous (25 -35%) • Penetrating trauma/surgery (10%) • Cryptogenic (15 -20%)
 • Occurs by: – Direct extension through infected bone")
DIRECT SPREAD (from contiguous foci) • Occurs by: – Direct extension through infected bone – Spread through emissary veins, diploic veins, local lymphatics • The contiguous foci include: • Otitis media/mastoiditis • Sinusitis • Dental infection (<10%), typically with molar infections • Meningitis rarely complicated by brain abscess (more common in neonates with Citrobacter diversus meningitis, of whom 70% develop brain abscess)
 • Sources: – Empyema, lung abscess, bronchiectasis, endocarditis, wound")
HEMATOGENOUS SPREAD (from remote foci) • Sources: – Empyema, lung abscess, bronchiectasis, endocarditis, wound infections, pelvic infections, intra-abdominal source, etc… – may be facilitated by cyanotic HD, AVM. • Results in brain abscess(es) at middle cerebral artery distribution • Often multiple

PREDISPOSING CONDITION & LOCATION OF BRAIN ABSCESS Otitis/mastoiditis Temporal lobe, Cerebellum Frontal/ethmoid sinusitis Frontal lobe Sphenoidal sinusitis Dental infection Remote source Frontal lobe, Sella turcica Frontal > temporal lobe. Middle cerebral artery distribution (often multiple)

Microbiology of Brain Abscess • Dependent upon: • Site of primary infection • Patient’s underlying condition • Geographic location • Usually streptococci and anaerobes • Staph aureus, aerobic GNR common after trauma or surgery • 30 -60 % are polymicrobial

Predisposing Conditions & Microbiology of Brain Abscess Predisposing Condition Usual Microbial Isolates Otitis media or mastoiditis Streptococci (anaerobic or aerobic), Bacteroides and Prevotella spp. , Enterobacteriaceae Sinusitis (frontoethmoid or sphenoid) Streptococci, Bacteroides spp. , Enterobacteriaceae, Staph. aureus, Haemophilus spp. Dental sepsis Fusobacterium, Prevotella and Bacteroides spp. , streptococci Penetrating trauma or postneurosurgical S. aureus, streptococci, Enterobacteriaceae, Clostridium spp. PPID, 2000

PREDISPOSING CONDITION USUAL MICROBIAL ISOLATES Lung abscess, empyema, bronchiectasis Bacterial endocarditis Fusobacterium, Actinomyces, Bacteroides Prevotellaspp. , streptococci, Nocardia S. aureus, streptococci Congenital heart disease Streptococci, Haemophilus spp. Neutropenia Aerobic gram-negative bacilli, Aspergillus Mucorales, Candidaspp. Transplantation Aspergillus spp. , Candida spp. , Mucorales, Enterobacteriaceae, Nocardia spp. , Toxoplasma gondii HIV infection Toxoplasma gondii, Nocardia spp. , Mycobacterium spp. , Listeria monocytogenes, Cryptococcus neoformans PPID, 2000
 Streptococci (S. intermedius, including S. anginosus) 60–")
MICROBIOLOGY OF BRAIN ABSCESS AGENT FREQUENCY (%) Streptococci (S. intermedius, including S. anginosus) 60– 70 Bacteroides and Prevotella spp. 20– 40 Enterobacteriaceae 23– 33 Staphylococcus aureus 10– 15 Fungi * 10– 15 Streptococcus pneumoniae <1 Haemophilus influenzae <1 Protozoa, helminths † (vary geographically) <1 *Yeasts, fungi (Aspergillus Agents of mucor Candida Cryptococci Coccidiodoides Cladosporium trichoides Pseudallescheria boydii) †Protozoa, helminths (Entamoeba histolytica, Schistosomes Paragonimus Cysticerci) CTID, 2001

CLINICAL MANIFESTATIONS • Non-specific symptoms • Mainly due to the presence of a spaceoccupying lesion • H/A, N/V, lethargy, focal neuro signs , seizures • Signs/symptoms influenced by • • Location Size Virulence of organism Presence of underlying condition

CLINICAL MANIFESTATIONS OF BRAIN ABSCESS Headache Fever Altered mental status Triad of above three Focal neurologic findings Nausea/vomiting Seizures 70% 50 50 -60 <50 50 25 -50 25– 35 Nuchal rigidity 25 Papilledema 25 CTID, 2001. PPID, 2000
, nonspecific – Abrupt, extremely")
CLINICAL MANIFESTATIONS Headache • Often dull, poorly localized (hemicranial? ), nonspecific – Abrupt, extremely severe H/A: think meningitis, SAH. – Sudden worsening in H/A w meningismus: think rupture of brain abscess into ventricle (often fatal)

LOCATION & CLINICAL FEATURES • FRONTAL LOBE: H/A, drowsiness, inattention, hemiparesis, motor speech disorder, AMS • TEMPORAL LOBE: Ipsilateral H/A, aphasia, visual field defect • PARIETAL LOBE: H/A, visual field defects, endocrine disturbances • CEREBELLUM: Nystagmus, ataxia, vomiting, dysmetria

DIFFERENTIAL DIAGNOSIS • Malignancy – Abscess has hypo-dense center, with surrounding smooth, thinwalled capsule, & areas of peripheral enhancement. – Tumor has diffuse enhancement & irregular borders. – SPECT (PET scan) may differentiate. CRP too? • • CVA Hemorrhage Aneurysm Subdural empyema/ICEpidural abscess

DIAGNOSIS • High index of suspicion • Contrast CT or MRI • Drainage/biopsy, if ring enhancing lesion(s) are seen

IMAGING STUDIES • MRI – more sensitive for early cerebritis, satellite lesions, necrosis, ring, edema, especially posterior fossa & brain stem • CT scan • 99 m Tc brain scan – very sensitive; useful where CT or MRI not available • Skull x-ray : insensitive, – if air seen, consider possibility of brain abscess
")
LABORATORY TESTS BRAIN ABSCESS • Aspirate: Gram/AFB/fungal stains & cultures, cytopathology (+/-PCR for TB) • WBC Normal in 40% ( only moderate leukocytosis in ~ 50% & only 10% have WBC >20, 000) • CRP • ESR • BC • LP almost invariably elevated Usually moderately elevated Often negative BUT Should still be done Contraindicated in patients with known/suspected brainabscess Risk of herniation 15 -30% If done, may have normal CSF findings, but: Usually elevated CSF protein & cell count (lymphs) Unremarkable glucose & CSF cultures rarely positive

TREATMENT • Combined medical & surgical • Aspiration or excision • empirical abx • Empirical antibiotics are selected based on: • Likely pathogen (consider primary source, underlying condition, & geography) • Antibiotic characteristics: usual MICs, CNS penetration, activity in abscess cavity • Modify abx based on stains • Duration: usually 6 -8 wks • after surgical excision, a shorter course may suffice

CT Scan

MRI scan

MRI Scan

MRI scan

MR spectroscopy

Tips for Dx on MRI

Treatment Options

Goals & advantages of stereotactic-guided surgical approach

Surgical indications

Contraindications

Complications

Outcome & prognosis







Armstrong ID, Mosby inc 1999

MEDICAL TREATMENT ONLY • Only in pts with prohibitive surgical risk: – poor surgical candidate, – multiple abscesses, – in a dominant location, – Abscess size <2. 5 cm – concomitant meningitis, ependymitis, – early abscess (cerebritis? ) – with improvement on abx, [Better-vascularized cortical lesions more likely to respond to abx alone] [ Subcortical/white-matter lesions are poorly vascularized]

CTID, 2001

SERIAL IMAGING IMPORTANT TO MONITOR RESPONSE

Before Rx After completion of Rx Armstrong ID, Mosby inc 1999

POOR PROGNOSTIC MARKERS • Delayed or missed diagnosis • Inappropriate antibiotics. • Multiple, deep, or multi-loculated abscesses • Ventricular rupture (80%– 100% mortality) • Fungal , resistant pathogens. • Neurological compromise at presentation • Short duration w severe AMS, • Rapidly progressive neuro. Impairment • Immunosuppressed host • Poor localization, especially in the posterior fossa (before CT) Modified from CTID, 2001

 • Intracranially, the dura is adherent")
EPIDURAL ABSCESSES • Spinal > intracranial (9: 1) • Intracranially, the dura is adherent to bone • True spinal epidural space is present posteriorly throughout the spine, thus posterior longitudinal spread of infection is common. – Anterior spinal epidural very rare (usually below L 1 & cervical)

American Family Physician April 1, 2002

SPINAL EPIDURAL ABSCESS INTRODUCTION • Rare, 0. 2 -1. 2 per 10, 000 hospital admissions • Median age 50 yrs (35 yrs in IVDU) • Thoracic>lumbar>cervical • Majority are acquired hematogenously

COMMON PREDISPOSING CONDITIONS • HEMATOGENOUS SPREAD: from remote infections & w IVDU • DIRECT SPREAD: Vertebral osteomyelitis, diskitis, decubitus ulcers, penetrating trauma, surgery, epidural catheters • Via paravertebral venous plexus: from abdominal/pelvic infections

PATHOGENESIS SPINAL EPIDURAL ABSCESS • Often begins as a focal disc or disc-vertebral junction infection • Damage of spinal cord can be caused by: – – – Direct compression Thrombosis, thrombophlebitis Interruption of arterial blood supply Focal vasculitis Bacterial toxins/mediators of inflammation • Even a small SEA may cause serious sequelae

MICROBIOLOGY SPINAL EPIDURAL ABSCESS The most common pathogens are: • Staph aureus >60% • Streptococci 18% • Aerobic GNR 13% • Polymicrobial 10% (Note: TB may cause up to 25% in some areas)

CLINICAL MANIFESTATIONS SPINAL EPIDURAL ABSCESS Four clinical stages have been described: 1. Fever and focal back pain; 2. Nerve root compression with nerve root pain; “shooting pain” 3. Spinal cord compression with accompanying deficits in motor/sensory nerves, bowel/bladder sphincter function; 4. Paralysis (respiratory compromise may also be present if the cervical cord is involved). Armstrong, ID, Mosby inc, 2000

DIAGNOSIS SPINAL EPIDURAL ABSCESS (Thinking of it is key, in a pt with fever, severe, focal back pain) • • MRI, CT Abscess drainage Blood cultures Routine Labs rarely helpful • ESR, CRP usually elevated, BUT non-specific • WBC may or may not be elevated • LP contraindicated

D/DX SPINAL EPIDURAL ABSCESS • • • Metastases Vertebral diskitis and osteomyelitis Meningitis Herpes Zoster infection Other disc/bone disease
 •")
TREATMENT SPINAL EPIDURAL ABSCESS • Early surgical decompression/drainage (preferably within first 24 h) • Antibiotics – Empiric abx should cover Staph, strep, & GNR – Duration of Rx : 4 -6 weeks
 • • 90% epidural abscesses are spinal Most SEA occur in thoracic (the")
(SEA/SDE) • • 90% epidural abscesses are spinal Most SEA occur in thoracic (the longest) Majority of SEA (>70%) are posterior to the cord Most SEA caused hematogenous spread & Staph aureus is the leading cause. • 95% SDE are in intracranial • Majority of SDE pts have associated sinusitis


INTRACRANIAL EPIDURAL ABSCESS • Less common & less acute than SEA • Rounded, well-localized (because dura is firmly adherent to bone) • Pathogenesis: – Direct ext. from contiguous foci (sinusitis, otitis/mastoiditis) – trauma, or surgery

INTRACRANIAL EPIDURAL ABSCESS • MICROBIOLOGY: Micraerophillic Strep, Propioni, Peptostrept, few aerobic g. NR, fungi. Postop: Staph, GNR. • CLINICAL MANIFESTATION: from SOL/ systmic igns of infection – Fever, HA, N/V, lethargy • • DX: - Think of it, imaging, drainage D/Dx: Tumor, other ICAbscesses Rx: Surgery + abx Mortality w appropriate Rx < 10%

SUBDURAL EMPYEMA • 15 -20 % of all focal intracranial infections • Motly a complication of sinusitis, otitis media, mastoiditis. • Most common complication of sinusitis (60% of such cases), mostly from frontal/ethmoid sinusitis. • Trauma/post-op & rarely hematogenous • M>F

SUBDURAL EMPYEMA Clinical Manifestations • Fever • Headache • Focal Neuro defects • Vomiting • Mental status changes • Seizures • Mass effect more common w SDE than w ICEA DX: CT, MRI (LP contraindicated) Rx: Surgery. Abx (3 -6 wks)
")
(Armstrong, ID, 1999, Mosby Inc)


PARASITIC BRAIN ABSCESS • • Toxoplasmosis Neurocysticercosis Amebic Echinococcal
 • >50% no known predisposing factor")
NOCARDIA BRAIN ABSCESS • Usually in immunosuppresed (CMI) • >50% no known predisposing factor • All pts w pulmonary nocardiosis should undergo brain imaging to r/o subclinical CNS nocardiosis • Rx: Sulfa (T/S invitro synergy), imipenem, ceftriaxone, amikacin, minocin – Duration of abx <a year. – Needle aspiration or surgical excision needed in most. • Relapse common

BRAIN ABSCESS IN AIDS • Toxoplasmosis is the most common • Seropositive • d/dx lymphoma • Often empiric Rx given & biopsy only nonresponders • Listeria, Nocardia, tb, fungi…

BRAIN TB • Rare cause of brain abscess • Usually in immunocompromised • Tuberculoma is a granuloma (not a true abscess ) • Biopsy/drainage (send for PCR too )
 • IMMUNOCOMPROMISED • Poor inflammatory response,")
FUNGAL BRAIN ABSCESS (Aspergillus, Mucor. . . ) • IMMUNOCOMPROMISED • Poor inflammatory response, less enhancement on CT. • May present w much more advanced disease (seizure, stroke more common) • High mortality • Rx: aggressive surgery + antifungal

BRAIN ABSCESS SEQUELAE • Seizure in 30 -60% • Neuro deficits 30 -50% • Mortality 4 -20%

YIELD OF CULTURES SPINAL EPIDURAL ABSCESS SOURCE • Abscess fluid aspirate • Blood culture • CSF* *LP often contraindicated YIELD 90% 62% 19%
- Slides: 75